
 MYKOLA POKHODZHAY/ISTOCK/GETTY IMAGES PLUS
MYKOLA POKHODZHAY/ISTOCK/GETTY IMAGES PLUS
Using 3D Printing to Streamline Time-Sensitive Immediate Dentures
The application of in-house three-dimensional printing technology can greatly accelerate denture delivery.

Beyond doubt, the incorporation of digital technology is at the forefront of modern dentistry. Practitioners are now realizing the many benefits these changes can bring to day-to-day practice. By utilizing three-dimensional (3D) printing systems and an efficient digital workflow, dentists find themselves in a position to simplify work, while providing timely, satisfactory results. With current technology, practitioners can deliver an esthetic, functional appliance — either the same day, or within a few days — while the patient is in an interim phase of treatment.
This is especially important in cases in which the time involved in conventional prosthetic fabrication can be of concern for the patient and dentist. Although 3D printing historically has been reserved for larger dental service organizations or practices with in-house laboratories, it is currently possible for small private practices to take advantage of this technology — where the future possibilities seem endless. This article is intended to raise awareness of the beneficial impact in-house 3D printing can offer. By way of illustration, it will present a case study involving a patient who wished to receive a denture to improve her esthetics immediately while she waited for either a definitive denture in the future, or possibly an implant-retained prosthesis.

CLINICAL CASE OVERVIEW
A 66-year-old female presented to the dental clinic with the chief complaint that her “teeth hurt, and I hate the way they look. I want them pulled and a new smile by next week!” Due to the patient’s grandchild graduating from school the following week, she expressed a strong desire to improve her smile as quickly as possible (Figure 1). Prior to the initiation of treatment, her medical and social histories were reviewed. Clinical examination revealed occlusal disharmony, with an existing improperly fitting maxillary removable partial denture, which was worn only sporadically. Radiographic examination revealed several carious and periodontally compromised teeth. A caries risk assessment deemed her as high risk.
The patient had very little foreknowledge regarding treatment options; however, both short- and long-term options were discussed, including:
- Extraction of all remaining teeth, with an immediate maxillary complete denture.
- Extraction of all remaining teeth, with an all-on-four maxillary implant-supported denture for total rehabilitation of an edentulous patient.
- Extraction of all remaining teeth, with a maxillary implant-retained overdenture. This denture is retained with a locator housing that is embedded and bonded to the intaglio surface of the denture and simply snaps into place over the implant locator abutment that is secured to the implant interface.
After discussion of her current financial status, the patient elected to extract the remaining maxillary teeth and place an immediate denture while she considered her long-term restorative options.
PREPARATION APPOINTMENT
Traditionally, taking impressions and various records would be the initial phase in creating a multistep, multiple appointment maxillary immediate complete denture. Many times, prosthesis fabrication might take several weeks. In this case, efficiency was maximized at the first appointment by using intraoral scanning instead of traditional impressions. The records appointment was initiated by scanning the patient’s maxillary and mandibular arches, while obtaining the bite relationship using an intraoral digital scanner (Figure 2). This bite relationship using the patient’s remaining teeth determined the digital interocclusal records.
While scanning, it is particularly crucial to capture the entire palate, vibrating line, tuberosities, and retromolar pads of the opposing arch for optimal accuracy in the digital imaging process. Gathering as much intraoral imaging and gingival detail as possible are paramount and the most challenging part of the scanning process. A series of intraoral and extraoral photographs were also taken to aid proper design of the denture. The patient was dismissed and scheduled three days later for extractions and delivery of the maxillary immediate denture, eliminating the need for conventional try-in appointments.
PROSTHETIC DESIGN AND DIGITAL WORKFLOW
Creation of a working model with the maxillary teeth extracted was needed in launching this design. Two options were considered for this process. The first included the rendering of a complete digital model using 3D rendering software. Although this is an adequate option, it often proves to be a time-consuming technique that creates a distinct stereolithography (STL) final digital file that is larger than desired for most denture creation programs.1 Smaller STL file sizes allow software to run faster, with less chance of program failure. Therefore, the second option of utilizing a hybrid technique, which employs both digitally rendering a 3D model and conventional border molding techniques, was chosen.

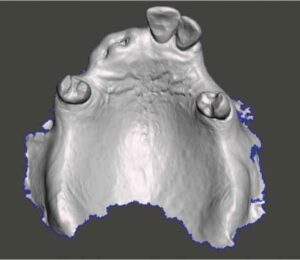
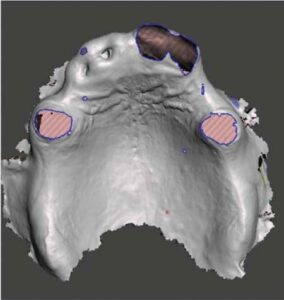
The first step was to create a hybrid extracted-tooth working model. To accomplish this, the original digital scan was imported into special software. This program was used to digitally remove the patient’s teeth from the maxillary model and create a solid 3D model that could be 3D printed (Figure 3 and Figure 4). Using a desktop, in-house 3D printer, the working model was printed, and allowed to properly cure and dry (Figure 5). Application and border molding with red baseplate wax was used to smooth the rough edges in preparation for digital scanning of the hybrid model (Figure 6). Since this was done on a model and not in the patient’s mouth, the wax should be placed in a position that approximates where the practitioner feels the borders should end. Any discrepancies will be manually adjusted at the delivery appointment. Next, the printed hybrid working model was scanned to create a digital model. This resulted in a smaller file size than if it were created entirely with digital software. Once the maxillary digital scan was completed, the information was imported into the software again to create a solid 3D digital model base.
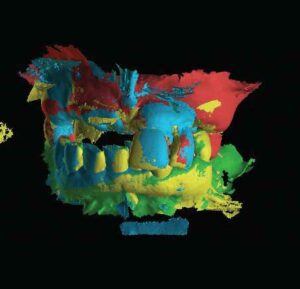
Special denture design software was used for the creation of the digital design for the immediate denture. Aligning all scanned images for the software to correctly comprehend the proper occlusal relationship of the maxilla and mandible is imperative during this step. Carefully uploading the scans while comparing the articulation of the teeth in the software to the preliminary photos is significant in ensuring software alignment is accurate. This process is commonly called stitching the scans (Figure 7). Consequently, this is the most important step to ensure a smooth delivery appointment, as scans that do not have a correct relationship will create a denture that offers poor occlusion.

BUILDING, PRINTING AND FABRICATION
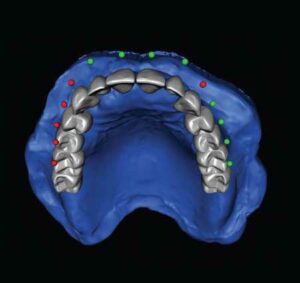
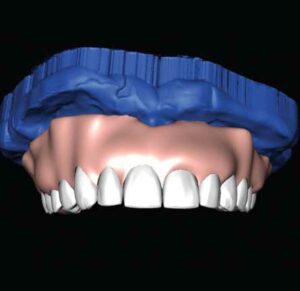
Once alignment accuracy was determined, the digital construction or building phase of the denture was initiated. The first step involves tooth selection from a library of digital teeth supplied in the software, followed by placement and positioning of the teeth against the digital model that was previously created. After the teeth were set in the correct position, the software was used to design and digitally smooth the gingiva for the prothesis (Figure 8 and Figure 9).
Finally, the denture was ready for printing. It should be noted that when 3D printing a denture, there are two printing options. The first is to print the entire denture out of the same color chosen for the denture teeth, followed by manually painting the gingival area pink using a gingival resin kit. The second option involves two-step printing: Printing the gingiva out of a pink shade of resin, followed by printing the teeth from a tooth-colored resin. For this case, a two-step printing technique was utilized with 3D printer denture resin for the gingiva, and 3D printer tooth resin for the teeth (Figure 10).
After the denture base is finished and the denture teeth are printed, they must be bonded together. Using uncured 3D printer denture resin, the inner socket surface of the denture base was painted. Next, the base and teeth were held together as the prothesis was spot cured with an ultraviolet curing light (Figure 11). The completed and bonded denture, including 3D printing scaffolding artifacts, was carefully placed into a curing unit to completely cure the resin. Following scaffolding removal, the denture was ready to be finished and polished using typical denture polishing techniques to prepare for delivery (Figure 12).
FINAL APPOINTMENT AND DELIVERY
As planned, the patient returned for extractions and delivery of the maxillary immediate complete denture within three days of the diagnostic appointment (Figure 13). After the extractions were completed, minor adjustments to the intaglio surface of the denture were made using pressure indicating paste and traditional denture adjusting burs. Postoperative instructions were given to the patient before being dismissed.
It was determined at the delivery appointment that the midline position of the denture could have been improved and this will be addressed in the final prosthesis. The patient had no concerns about the midline, however. Overall, the patient was satisfied with the improved esthetics achieved in such a short time frame, and will decide on her long-term solution in the ensuing months (Figure 14). Therefore, during her healing and decision-making process, she was instructed to return for proper periodontal and restorative care on the mandibular arch.

DISCUSSION
As recently as a decade ago, it was uncommon for a private-practice dentist to purchase an in-house 3D printer with the intention of creating dentures. Extreme costs, time constraints, and inadequate workflow systems among outside dental laboratories brought frustration for practitioners. Furthermore, the U.S. Food and Drug Administration had yet to approve intraoral use of many resins, some of which required extended curing times. Biocompatibility is essential in the 3D printing process, and, historically, traditionally engineered resins were not adequate for working in the oral cavity.2 At best, making records in an easier and more convenient fashion for patients — while reducing costs for the practitioner — seemed to be the most notable advancements at that time. With many technological improvements, these once idealistic philosophies have now come to fruition as 3D printing has evolved. Dentists now have biocompatible resins available that are also economically feasible.2 This means these resins work from both a technological and practicality viewpoint, and are safe to utilize in dental applications.2

Adequate knowledge of the proper clinical use and mechanical properties (such as strength and durability) of denture acrylic resins can be of significance in obtaining optimal results for any prosthesis. The strength advantages of heat-polymerized polymethyl methacrylate (PMMA) is still considered by many to be the gold standard in dentistry.3 However, PMMA possesses several disadvantages, such as high polymerization shrinkage, potential allergic reactions to the chemical makeup, and a higher susceptibility to microbial colonization than other resins.4 In this case study, the 3D denture material used was a type of resin similar in characteristics to PMMA, with corresponding properties compared to conventional acrylic — with the added ease of curing through ultraviolet light instead of temperature.3 While visible light-polymerized urethane dimethacrylate resin typically offers increased flexural strength over its counterpart PMMA, it also demonstrates a decrease in load limits, with a higher degree of brittleness.5 Heat-cured resins provide the strongest bonds between denture base resin and the denture teeth themselves. However, newer developments in resin biomaterials have made it possible for 3D-printed teeth to have comparable fracture resistance characteristics to prefabricated resin teeth.4

In the fabrication process of dental 3D printing, there still appears to be some debate over the building or layering orientation of the prosthesis. This topic has prompted much discussion due to the technological phases involved during incremental layering when creating the denture. It has been found that layering possibly compromises the structural integrity of the product by cracking or making the bond between the layers weaker — thus resulting in possible long-term structural failure of the 3D-printed material.6
While the strength of new 3D-printed resins is constantly increasing, the argument continues about the long-term permanence of the restorations.7 Factors such as time, cost and control are key elements in the decision to choose 3D-printed dentures over proven PMMA materials. In consideration of time — from the standpoint of initial records, digital impressions, and the actual manufacturing of the prosthesis — it is highly unlikely that a conventionally built, heat-cured PMMA immediate denture could be delivered as quickly as a 3D-printed denture.8,9 Therefore, when time is of the essence, 3D printing can be a preferable option over traditional methods.

Regarding patient cost concerns, as the market price of 3D materials continues to decrease, 3D-printed options are becoming less burdensome than conventionally produced prostheses. Oftentimes, communication challenges between the dentist and the laboratory cause delays in treatment and extended or unnecessary appointments. Possible errors that occur from the transmission of this information are eliminated within practices that use 3D printing due to the fabrication of the prosthesis in-house.10 The clinical advantages of being able to diagnose, fabricate, and deliver under the same roof cannot be overstated. In instances where more control over the case is desired, 3D printing becomes the more viable option over conventional techniques.

CONCLUSION
The use of digital dentistry offers numerous possibilities and opportunities for patients and practitioners. Depending on the complexity of the case, in-house 3D printing allows the dentist to offer turnaround times of hours or days instead of weeks. Furthermore, in-house 3D printing helps clinicians avoid possible back-and-forth exchanges with the dental lab.2 By utilizing this technology, it would even be possible for a dentist to go from an intraoral scan to a completed denture in a single visit.
While some providers might consider the learning curve to adopt 3D printing as prohibitively steep, others embrace the notion that the benefits of 3D printing are more than worth the time and commitment. Although there is a rapid growth in the use of 3D printing, the dentist must have the basic, foundational knowledge and clinical skill set of general dentistry — and the creation of full-mouth prostheses in particular — thoroughly developed before advancing to this next level of technology. Clinicians have to problem-solve, and sometimes that involves going back to basics. Moving forward, practicing dentists should approach any case with the mindset of successfully achieving the best outcome for the patient. The final result is the most important factor, not the route taken to get there.1
Key Takeaways
- Practitioners are now realizing the many benefits digital dental technologies bring to day-to-day practice.
- For example, with current three-dimensional (3D) printing technology, practitioners can deliver an esthetic, functional appliance — either the same day, or within a few days — while the patient is in an interim phase of treatment.
- This is especially important in cases in which the time involved in conventional prosthesis fabrication is an issue for the patient and dentist.
- Adequate knowledge of the proper clinical use and mechanical properties of denture acrylic resins can be of significance in obtaining optimal results for any prosthesis — and particularly with 3D-printed prostheses.
- The clinical advantages of being able to diagnose, fabricate, and deliver under the same roof cannot be overstated.
- While some providers may consider the learning curve to adopt 3D printing as prohibitively steep, others embrace the notion that the benefits of 3D printing are more than worth the time and commitment.
References
- Stumpel LJ. An analog intermezzo in a digital workflow. Compend Contin Educ Dent. 2020;41:536–542.
- Scherer M. The invention of 3D printing and its impact on dentistry. Compend Contin Educ Dent. 2020;41:504–507.
- DENTCA 3D Printed Dentures. Available at: htt/://dev.www.dentca.com/products/dentca-3d. Accessed February 9, 2022.
- Anadioti E, Musharbash L, Blatz MB, Papavasiliou G, Kamposiora P. 3D printed complete removable dental prostheses: a narrative review. BMC Oral Health. 2020;20:343.
- Palitsch A, Hannig M, Ferger P, Balkenhol M. Bonding of acrylic denture teeth to MMA/PMMA and light-curing denture base materials: the role of conditioning liquids. J Dent. 2012;40:210–221.
- Diaz-Arnold A, Vargas M, Shaull K, Laffoon J, Qian F. Flexural and fatigue strengths of denture base resin. J Prosthet Dent. 2008;100:47–51.
- Kim J, Lee D-H, Markiewicz MR, Al-Jewair T, Andreana S, Arany PR. Additive 3-dimensional printing as a novel tool for pre and postsurgical evaluation and patient education. J Am Dent Assoc. 2021;152:567–575.
- Kuckuka E. Checking References. Available at: https://www.dentaltown.com/magazine/article/8333/checking-references. Accessed February 9, 2022.
- Dorr L. Digital Dentures Delivering Esthetics, Reduced Adjustments. Available at: https://www.dentalproductsreport.com/view/digital-dentures-delivering-esthetics-reduced-adjustments. Accessed February 9, 2022.
- PunJ A, Fisselier F. Digital dentistry for complete dentures. Decisions in Dentistry. 2020;6(8):12–14, 16.
From Decisions in Dentistry. March 2022;8(3):9-10, 13-14.
