
 ALEX-MIT / ISTOCK / GETTY IMAGES PLUS
ALEX-MIT / ISTOCK / GETTY IMAGES PLUS
Understanding Orthognathic Surgery
An exploration of the use of orthodontics-only treatment versus a combination approach utilizing orthodontics and orthognathic surgery.
One of the procedures in dentistry that best exemplifies true interdisciplinary care is that of orthognathic surgery. It requires, at a minimum, excellent cooperation between an orthodontic provider and oral surgeon. In many cases, even more aspects of dentistry are involved, especially in adult patients with more complex dental needs where restorative treatment, prosthodontic treatment and endodontic treatment may be necessary after a combined orthodontic/orthognathic surgical approach is utilized.

Orthognathic surgery is used to correct malocclusions of a skeletal origin that are so severe that growth modification, orthodontic treatment alone (i.e., dental camouflage), and even the use of temporary anchorage devices are unable to significantly correct the malocclusion. The indications for orthognathic surgery are often functional deficits and unsatisfactory facial esthetics.1 Functional issues that can cause patients to seek orthognathic surgery include problems with biting and chewing, adverse impacts on the dentition as a result of the malocclusion, sleep disorders, speech issues, and temporomandibular joint problems.2

Esthetic issues generally include the desire to improve facial appearance outside of what orthodontics alone can provide. The improvement in facial esthetics can have profound effects ranging from elimination of self-esteem issues associated with poor facial esthetics, a positive change in personality due to treatment of facial features the patient considered undesirable, and an overall improvement in quality of life and elimination of some psychosocial factors following treatment.3

ANTERIOR-POSTERIOR ORTHODONTIC AND SURGICAL CHANGES
Some dental providers, especially general practitioners, are not always clear on the major differences between orthodontics-only treatment and a combined orthodontic/orthognathic surgical approach. Although orthodontics-only and combined orthodontic/orthognathic surgery both involve the wearing of orthodontic appliances, the intent of each treatment is entirely different for each type of malocclusion. In orthodontics-only correction of a malocclusion, clinicians utilize the dentition to mask or camouflage the underlying skeletal discrepancy. In a patient with a moderate Class II skeletal pattern in which (1) the maxilla and maxillary dentition is positioned too far forward relative to the face and a normally positioned mandible, or (2) the maxilla and dentition are normally positioned and the mandible and its dentition are posteriorly positioned, or (3) there is both a maxillary skeletal/dental malposition and a mandibular skeletal/dental malposition, the lower dentition is positioned more forward on the dental base and the maxillary dentition, especially the maxillary incisors, is positioned more posteriorly and upright on its skeletal base.
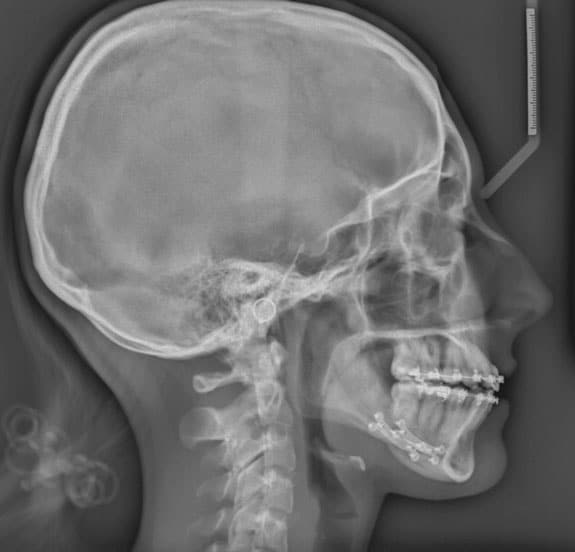
The above-described positioning of the maxillary dentition (uprighting maxillary incisors and proclination of mandibular incisors) utilize Class II mechanics (a force acting distally on the maxillary dentition and in a mesial direction on the mandibular dentition) to effect changes in the dentition. This type of mechanics can be done with auxiliary appliances or elastics from the lower molar region to the maxillary anterior region (Class II elastics). The cephalometric radiographs in Figure 1 and Figure 2 demonstrate the Class II compensation movements with orthodontics-only as the correction modality.

However, with a Class II surgical case, the teeth should be moved in the opposite fashion than when using orthodontics-only correction. The incisors in both arches should be in a position similar to how they would be positioned in a Class I corrected malocclusion. This “opposite” movement of the incisors is called decompensation, which make malocclusion worse before surgery due to the movement of the incisors. In this case, the malocclusion is corrected through movement of the bony bases. When the incisors are decompensated in preparation for a Class II surgery, the mandibular incisors are uprighted and the maxillary incisors are proclined to a normal Class I position, which makes the overjet worse before the surgery. Figure 3 and Figure 4 demonstrate decompensation of the incisors in setting up the dentition for a Class II correction surgery.

In the orthodontics-only correction of a Class III malocclusion, the opposite is true. The mandibular incisor crowns are more posteriorly positioned or retroclined, while the maxillary incisor crowns are moved anteriorly or proclined to correct the malocclusion and establish positive overbite and overjet. Figure 5 and Figure 6 illustrate this compensation for correction of a Class III malocclusion.

Using an orthodontic/orthognathic surgical correction of a skeletal Class III malocclusion, the tooth movement is just the opposite. In preparation for a surgical correction, the maxillary incisors are uprighted and moved distally, while the mandibular incisors are proclined. Figure 7 and Figure 8 demonstrates this Class III decompensation. Again, this increases the negative overjet before the surgery and the malocclusion appears worse.

If one looks at the overall picture of tooth positioning prior to an orthognathic surgical procedure, it becomes apparent the teeth are generally moving in the opposite direction than the respective jaws in which the teeth are positioned prior to surgery.4 The purpose of this is to place the teeth in an ideal position for a Class I skeletal relationship before allowing the surgical movements to move the bony bases to establish the Class I skeletal relationship. By allowing the surgical movements of the jaws to be increased once the incisors are decompensated, it places the teeth in the most stable position possible to assist in minimizing postsurgical orthodontic relapse.5
Despite the positive influences on the surgery itself, esthetic improvements, and increasing stability of the final result, orthodontic decompensation also can move the surgical treatment planning from a one-jaw procedure into the two-jaw surgical realm.6 With the increased awareness of jaw positions and intraoral volume and their relationship to obstructive sleep apnea, many surgeries that were once a single-jaw procedure (mandibular reduction) are now treated with both maxillary advancement and mandibular reduction in patients with significant Class III malocclusions.7 Figures 9 through 12 illustrate this principle.

Many oral surgeons are reluctant to do surgical movements in one jaw that approach the limits of surgical movement and opt instead for surgical movements of two jaws that reduce the movement of each and increase surgical stability. For example, a severe Class III malocclusion with a negative overjet of 10 mm with a normally positioned maxilla and dentition will often be treated with a 4 to 5 mm advancement of the maxilla and a 5 to 6 mm reduction of the mandible instead of a 10 mm mandibular set-back surgery. This reduces the posterior movement of the mandible and its subsequent effect of moving the hyoid bone posteriorly (which can lead to sleep apnea issues), and also increases intraoral volume by moving the maxilla forward, which allows the tongue more intraoral space to occupy and also helps reduce the chances of sleep apnea.8 An example of a maxillary only surgery on a patient with obstructive sleep apnea is demonstrated in Figure 13 and Figure 14.

VERTICAL CHANGES
The vertical dimensions of the lower face are also changed with surgical procedures. This vertical change can be the primary purpose of the surgery or a welcome corollary change as a result of the antero-posterior (A-P) correction of the skeletal units. In patients with long, narrow faces, referred to as a leptoprosopic facial form, one of the surgical goals is to reduce the vertical height of the lower face (the portion between the inferior aspect of the nose and soft tissue menton). The maxilla is often impacted posteriorly to reduce the posterior dental height, which allows the mandible to rotate counterclockwise in a Class II patient; this improves not only the A-P position of the mandible, but also shortens the lower facial height. In more severe Class II patients with vertical facial excess, the autorotation of the mandible may not be adequate to correct the dental malocclusion and a mandibular advancement may be necessary.

In a Class II patient with a short lower face (referred to as a euryprosopic facial form), often the desired outcome of the surgery is not only to correct the A-P relationship, but also increase the lower facial height. In this case, there is no impaction of the maxilla; rather, the increase in facial height comes from opening the deep bite with the surgical advancement of the mandible.

With Class III surgical patients with an open bite, often there is a need to not only reduce the A-P discrepancy between the two jaws, but also shorten the lower facial height. This is done by impacting (more in the posterior than anterior) and advancing the maxilla, and then doing a mandibular reduction procedure.

In Class III patients exhibiting a posteriorly positioned maxilla with a decreased lower facial height and deep bite, the maxilla is often moved forward and the mandible rotates in a clockwise direction, which helps in the Class III A-P correction and increases the lower facial height. When the discrepancy is significant, there will often be the need for a mandibular reduction procedure, as well.
The correction of the vertical relationship of the jaws may be the primary reason for the surgical procedure, but may also result from the A-P correction (Figure 15 and Figure 16).9

TRANSVERSE CHANGES
Transverse relationships are often corrected surgically. The transverse discrepancies may be relative (i.e., the original position of the jaws and dentition in malocclusion may appear to be abnormal in the original malocclusion and normal once the jaws are positioned in a Class I relationship) or the transverse discrepancy may be absolute (when the jaws are positioned in a Class I relationship, the maxillary width is deficient for the mandibular dentition). The relative transverse deficiency is often found in a Class III patient who appears to have a posterior crossbite in the malocclusion state, but the crossbite is resolved when the surgical procedure is done and a wider portion of the maxilla is juxtaposed to a narrower portion of the mandible. An example of an absolute deficiency would be a mandibular advancement in which the Class II relationship and buccal overjet appear normal, but when the mandible is advanced there exists a palatal crossbite with the maxilla not having enough width when the first molars are placed in a Class I position. That is, the wider part of the mandibular arch is positioned more anteriorly with the surgical advancement and a crossbite results.10,11
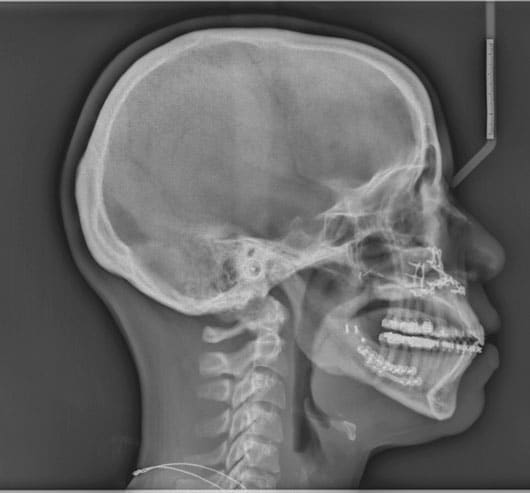
radiograph of same Class I patient with a
surgically corrected open-bite.
Dental correction of the posterior crossbite prior to surgery was once considered inappropriate due to the high probability of relapse. Advances in recent decades have given the orthodontist/oral surgeon team options to correct transverse deficiencies prior to surgery with fairly good stability. The first method involves a surgery to widen the maxillary arch prior to the primary orthognathic procedures. This is called a surgically assisted rapid palatal expansion (SARPE), in which an expander is placed, the maxillary alveolar bone is cut superiorly to the roots of the dentition, and the soft tissue incision is closed. The patient turns the expander several times a day postsurgically to increase the transverse dimension of the maxillary dental arch to simplify or eliminate any maxillary treatment at the time of the orthognathic surgical procedures. It effectively eliminates the need to cut the maxilla into multiple segments to increase the width of the dental arch at the time of the orthognathic surgery (Figure 17 and Figure 18).

The second option in certain cases of a mild transverse discrepancy is to use a miniscrew assisted rapid palatal expansion technique to widen the maxillary arch prior to the surgical procedure.12 This shows promise in younger adult patients by providing true skeletal expansion at the mid-palatal suture; it also eliminates the need for the more invasive SARPE or segmented maxillary surgery (Figure 19 and Figure 20).


THE CHIN
Often for patients who need or desire orthognathic surgery, the surgical movements may still leave the desire for a stronger or weaker chin unresolved. In such cases, it may be necessary to either do an advancement genioplasty or a reduction genioplasty.13 The advancement genioplasty not only moves the chin point anteriorly in space but, depending on the direction of the cut, can also slightly reduce the vertical aspect of the lower facial height (Figure 21 and Figure 22).

A reduction genioplasty, in cases with a very strong chin point projection, can not only reduce the chin point prominence in space, but also (depending on the direction of the cut) increase the vertical height of the lower face.
SUMMARY
Skeletal malocclusions often exceed the limits of orthodontic correction of the dentition without placing the teeth in compromised positions that result in both immediate and long-term deleterious effects. With orthognathic surgery combined with orthodontic tooth movements, the skeletal components of the maxillomandibular complex can be repositioned in such a manner the dentition can be appropriately positioned over the skeletal bases. The benefits to the patient include resolution of the malocclusion, increased stability of the results, and often significant improvement in esthetic outcomes.

The overarching benefit is that orthognathic surgery can often resolve the patient’s chief complaint, whereas orthodontics-only correction of a malocclusion can leave aspects of the patient’s concerns unresolved. Despite the costs and risks of surgery, it is often a worthwhile endeavor and a life-changing event for the patient.
REFERENCES
- Larsen MK, Thygesen TH. Orthognathic surgery outcome in a Facebook group. J Craniofac Surg. 2016;27:350–355.
- Cunningham SJ, Johal A. Orthognathic correction of dento-facial discrepancies. Br Dent J. 2015;218:167–175.
- Esperao PTG, de Oliveira BH, de Oliveira Almeida MA, Kiyak HA, Miguel JAM. Oral health-related quality of life in orthognathic surgery patients. Am J Orthod Dentofacial Orthop. 2010;137:790–795.
- Larson B. Orthodontic preparation for orthognathic surgery. Oral Maxillofac Surg Clin North Am. 2014:26:441–458.
- Jacobs J, Sinclair P. Principles of orthodontic mechanics in orthognathic surgery cases. Am J Orthod. 1983;84:399–407.
- Tompach PC, Wheeler JJ, Fridrich KL. Orthodontic considerations in orthognathic surgery. Int J Adult Orthodon Orthognath Surg. 1995;10:97–107.
- Pereira-Stabile CL, Ochs MW, De Moraes M, Moreira RWF. Peroperative incisor inclination in patients treated with orthognathic surgery. Br J Oral Maxillofac Surg. 2012;50:533–536.
- Haryani J, Nagar A, Mehrotra D, Ranabhatt R. Management of severe Class III malocclusion with bimaxillary orthognathic surgery. Contemp Clin Dent. 2016;7:574–578.
- Bryan DC. Surgical accuracy in orthognathic surgery. Br J Oral Maxillofac Surg. 1993;31:343–349.
- Reyneke JP, Conley RS. Surgical/orthodontic correction of transverse skeletal discrepancies. Oral Maxillofac Surg Clin North Am. 2020;32:53–69.
- Jacobs JD, Bell HM, Williams CE, Kennedy JW III. Control of the transverse dimension with surgery and orthodontics. Am J Orthod. 1980;73:284–306.
- Carlson C, Sung J, McComb RW, Machado AW, Moon W. Microplant-assisted rapid palatal expansion appliance to orthopedically correct transverse maxillary deficiency in an adult. Am J Orthod Dentofacial Orthop. 2016;149:716–728.
- Veltkamp T, Buschang PH, English JD, Bates J, Schow SR. Predicting lower lip and chin response to mandibular advancement and genioplasty. Am J Orthod Dentofacial Orthop. 2002;122:627–634.
From Decisions in Dentistry. November 2022;8(11)10, 13-14, 16.
