
 STANISLAVSALAMANOV/ISTOCK/GETTY IMAGES PLUS
STANISLAVSALAMANOV/ISTOCK/GETTY IMAGES PLUS
CE Sponsored by Church & Dwight: Role of pH in Remineralization And Dental Diseases
Optimal pH levels support remineralization and oral health by helping maintain homeostasis in the oral microbiome.
PURCHASE COURSE
This course was published in the September 2019 issue and expires September 2022. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the September 2019 issue and expires September 2022. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe the concepts of homeostasis, symbiosis and dysbiosis in the oral microbiome, and the role of saliva and oral pH levels in these processes.
- Explain how dietary choices and mechanical forces, including plaque removal and introducing remineralizing ions, can affect the demineralization/remineralization of tooth structure.
- Discuss the importance of evidence-based recommendations in the prevention and management of dental caries and other dental diseases.
INTRODUCTION
With a long history of providing safe and effective oral care products, Church & Dwight is dedicated to advancing oral health. As part of this vision, we strive to offer dental professionals the research and education they need to stay up to date on the provision of care. Church & Dwight — with its long-standing and trusted oral care solutions — is proud to provide an unrestricted educational grant in support of this continuing education article, “Role of pH in Remineralization and Dental Diseases,” by Martha McComas, RDH, MS. This important paper will ensure clinicians are well prepared to help their patients support remineralization and prevent dental diseases. We hope you find it helpful in your quest to provide individually tailored care for each of your patients.
Jaime Shepler
Professional Marketing
Church & Dwight Co., Inc.
Managing oral pH through diet and therapeutic agents can help fight dental diseases and support remineralization and oral health
Dental diseases develop via multifactorial processes. Although some dental diseases are the result of genetic factors (e.g., amelogenesis imperfecta), others, such as caries, are caused by local environmental factors. This article will focus on local environmental factors as a determinant of health or disease, specifically, how the oral environment plays a significant role in maintaining homeostasis that supports oral health. For example, dental caries develop through a continuum of demineralization and remineralization of the oral hard tissues (enamel and dentin) due to plaque biofilms and their metabolism byproducts.1–3 If demineralization (net mineral loss) is not interrupted by some means, an active caries lesion will eventually form. This demineralization/remineralization continuum is highly exacerbated during an acid attack when salivary pH falls to the critical level of pH 5.5 and below.1,4–6 These acidic episodes are highly dependent on the consumption of fermentable carbohydrates (such as sucrose, glucose, fructose and cooked starch),1 amount and frequency of consumption, effectiveness of mechanical biofilm removal, distribution of bioavailable remineralizing ions (key definitions are found in Table 1), and the rate and volume at which saliva is excreted.
Therefore, the objectives of this continuing education course are to:
- Describe the unique and diverse microbiome of the oral cavity, and the significance of pH on homeostasis in the oral environment.
- Explain how the consumption of fermentable sugars affects oral pH and disrupts the oral microbiome.
- Detail how mechanical plaque removal can help maintain an alkaline environment, and how depositing remineralizing ions (fluoride, calcium and phosphate) through mechanical means increases remineralization.
- Discuss the effects of salivary flow rates and salivary volume on oral biofilms, pH levels, acid neutralization and remineralization.
- Describe how sodium bicarbonate toothpaste with low abrasiveness and remineralizing ions helps to buffer acids, reduce cariogenic pathogens, and facilitate enamel remineralization.
ORAL MICROBIOME
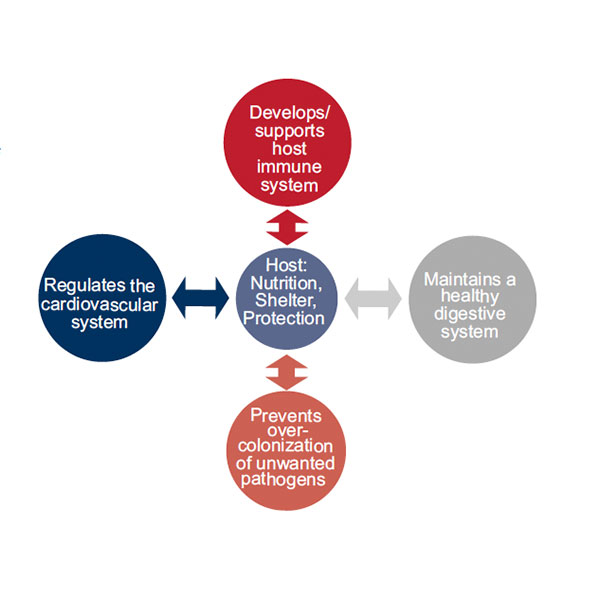
Compared to other parts of the body, the oral cavity harbors the most diverse microbiota.5–8 It has been reported that approximately 700 prokaryotic species have been identified as resident bacteria in the oral cavity, and that about 100 to 300 of those species can be isolated and cultured.5,7,8 These microbes live and grow on all exposed oral surfaces, such as enamel, exposed cementum and dentin, as well as the sulcular epithelium. Resident bacteria adhere to the intraoral surfaces via the ever-developing acquired pellicle through stages until co-adhesion occurs between oral molecules and initial and secondary colonizers.5,8 A symbiotic relationship exists between these microbial communities and their host, which in homeostasis contributes to systemic and oral well-being (Figure 1). The host provides the microbial communities a safe, wet and warm environment where nutrition is provided through saliva, gingival fluids and the host’s diet.5–8 In health, the resident bacteria help to develop the host’s immune system, keep invading pathogens to low levels, and assist in regulating the cardiovascular system and digestive tract.5–8
Currently, the most widely accepted theory for the development of dental diseases is the ecological plaque hypothesis.8 This postulates that pathogenic bacteria are part of the total diverse microbiota — even in health — and dental diseases arise from an imbalance in the oral environment in which the bacteria live.7 This complex balance between oral microbes and their environment can be transformed from symbiosis into dysbiosis with the slightest biological changes, especially changes in local pH levels.5–9
MICROBIOTA.
SIGNIFICANCE OF pH
In a neutral oral pH, the host and resident bacteria live in a symbiotic state in which biofilm communities co-aggregate, interact in metabolic activities, and engage in cell-to-cell signaling.6,8 It only takes slight changes in pH levels to induce an environment detrimental to resident nonpathogenic bacteria. This shift from alkaline to acidic allows for an oversaturation of resident pathogens that produce metabolic acids (acidogenic) and can thrive in an acidic environment (aciduric). Although hard tissue is surrounded by the protective acquired pellicle, a prolonged acidic event will allow acids to diffuse through the pellicle and initiate the demineralization process.10 This shift in pH from neutral to acidic is directly correlated with the consumption of fermentable carbohydrates, the frequency with which those sugars are consumed, and their bioavailability to the bacteria for metabolism.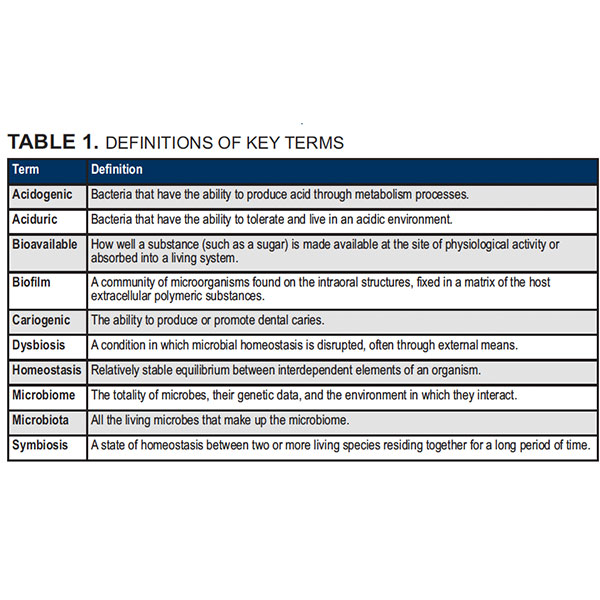
DIETARY FACTORS
A pivotal report11 published in 1940 concluded the strongest indicator of caries activity is the drop in oral pH initiated by the metabolism of dietary sucrose.11,12 There is a two-way relationship between diet and oral health. Not only does diet have a systemic effect on the integrity of the teeth and periodontal structures, it also has a significant effect on the composition of the oral biofilm, saliva and pH of the oral environment. Additionally, diet can have detrimental effects on the hard tissues, leading to caries lesion development and progression. However, it is not just sucrose and fructose that can be readily metabolized by these aciduric pathogens.13,14 Diets that include cooked or baked starches that when broken down by saliva become maltose — such as cakes, donuts and bread — provide another excellent food source for aciduric bacteria.13,14
Patients whose diets include these highly fermentable carbohydrates face increased risk of developing hard tissue caries. Individuals with this type of diet typically have an unbalanced oral microflora that is abundant in resident bacteria with cariogenic traits. By producing acids through the metabolism of sucrose, fructose, glucose and maltose, these pathogens have the ability to tolerate — and even accelerate — an acidic environment desirable for their survival.8,12,13,15
The relationship between sugar consumption and caries prevalence prompted the World Health Organization to reduce its recommendations regarding free sugar consumption for the average adult to less than 10% of the daily total energy intake — and it notes additional health benefits for those who reduce it below 5%.16,17 Although the amount and frequency of sugar intake are key factors, it is equally important to understand the importance of the bioavailability of sugar and food starches to oral biofilms; this refers to the amount of time the sugars are readily available for the bacteria to use and metabolize.14,17–21 Understanding the concept of bioavailability fosters awareness of the role of effective daily mechanical removal of plaque biofilm, food sugars, and the delivery of acid buffering/remineralizing agents.
MECHANICAL PLAQUE REMOVAL
J. Leon Williams, DDS, LDS, the first president of the American Dental Association, said, “A clean tooth will not decay,”22 suggesting that good oral hygiene is key to preventing caries. It is well established that pH in the oral cavity drops below critical levels (pH 5.5) when food sugars are introduced. However, a 2018 systematic review23 concluded that plaque removal alone does not reduce the overall caries incidence, reaffirming an earlier review study.23,24
The mechanical/physical action of toothbrushing increases tooth erosion and abrasion, as well as removal of the protective acquired pellicle, thus directly exposing enamel and dentin to oral acids.25,26 A direct exposure to lactic acids found in the oral environment increase the risk of hard tissue demineralization. Tooth wear has a multifactorial etiology, including abrasion, erosion and attrition, with the most prominent being erosion.27 Dental erosion can be defined as the dissolution of the hard tissues (enamel and dentin) due to oral acids, without the involvement of acidogenic bacteria.28 When erosion is noticeable, it can be assumed the hard tissue structure has already been initially damaged, yielding a “softer” enamel or dentin surface.28
This is important, as most over-the-counter toothpastes are packaged for specific needs, such as whitening, anti-caries action and tartar control, thus leading to a variety of abrasive levels available to consumers.26 In a 2016 study of enamel erosion and abrasion, Ganss et al26 noted the amount and size of the abrasive agent play important roles in a toothpaste’s erosion and abrasion potential. Relative dentin abrasiveness (RDA) is an American Dental Association (ADA) standardized numerical range (0 to 250) that conveys a toothpaste’s abrasiveness to oral hard tissues.29 Additionally, the ADA stipulates RDAs below 250 as the safe limit for hard tissues; however, it is best to use a toothpaste with the lowest effective RDA. Therefore, it is important to select a product with a low RDA to reduce additional iatrogenic erosion and abrasion of already softened enamel or dentin. Toothpastes with sodium bicarbonate as a predominant abrasive typically have RDAs below 80 (due to very low hardness of sodium bicarbonate itself), which can minimize abrasion of previously eroded surfaces or otherwise challenged tooth surfaces. This makes sodium bicarbonate toothpastes an excellent choice for patients who aggressively brush their teeth, have signs of erosion from diet or gastroesophageal reflux disease (GERD), or have a moderate to high caries risk.30
IMPORTANCE OF A VIBRANT SALIVARY SYSTEM
Saliva has been shown to play an essential role in maintaining the oral ecosystem through buffering acids and cleansing of the hard and soft tissues.25,31,32 The overall flow rate of a patient’s salivary system is a key influencer on his or her overall caries experience.10 In the absence of normal salivary flow (hyposalivation), food sugars are left attached to the acquired pellicle, creating an excellent source of nutrition for aciduric bacteria, as well as maintaining a prolonged acidic environment that is ideal for the reproduction of additional aciduric bacteria. However, in a vibrant salivary system, three main acid buffering agents — salivary proteins, phosphate and bicarbonate — are secreted during resting and stimulated salivary production.10,31–33 When secreted, these buffering agents help preserve the neutral pH (6.0 to 7.5) found in a healthy oral environment. When salivary pH drops to 5.5 and below, detrimental effects on dental hard and soft tissues can be noted.10,31–33 In this acidic environment, the protective and defensive properties of the acquired pellicle and resident nonpathogenic microbes are reduced and the process of hard tissue demineralization occurs.32
STRATEGIES FOR MAINTAINING NEUTRAL ORAL pH
For the prevention/management of dental diseases, such as caries, it is necessary to maintain an oral environment in which oral microbiota exist in a state of symbiosis. Maintaining a neutral pH can be accomplished through diet and attempts to change the oral environment and composition of the biofilm. One strategy that can help facilitate this change is the use of sodium bicarbonate toothpaste.34 Sodium bicarbonate, or household baking soda, which has an RDA of 7, has been used as an oral care product for centuries.35 Because baking soda alone has such a low RDA value, toothpaste with high baking soda content (> 20%) is generally extremely low in abrasion (RDA below 80).30 Toothpaste with high baking soda content can effectively neutralize an acidic oral pH, offer bactericidal properties34 and reduce gum redness and bleeding.30,33,36–38
Naturally found in saliva, bicarbonate is a primary factor in maintaining pH levels that favor homeostasis and oral health.30 The alkaline pH of sodium bicarbonate (8.3) makes it an excellent acid buffering agent, and it can be used with patients whose diet includes frequent fermentable carbohydrate intake or those who have an acidic oral environment due to systemic conditions, such as GERD.30 In addition to its buffering action, sodium bicarbonate toothpaste has been shown to have bactericidal properties.35 This is largely based on the ecological plaque hypothesis, as research has demonstrated sodium bicarbonate has the ability to change the composition of the biofilm and surrounding oral environment, making it especially useful for patients with high caries risk and/or hyposalivation.33 Similarly, a 2008 study concluded that butyric acids were significantly reduced when a preparation of sodium bicarbonate was introduced into the periodontal pocket, thereby reducing acid-induced inflammatory response.36 Therefore, sodium bicarbonate can be especially beneficial for patients with periodontitis (with or without a significant caries risk).36
The fluoride ions found in today’s toothpastes remineralize enamel and increase its ability to resist further demineralization and erosion.1,13,25,39,40 Additionally, the calcium and phosphate ions that are naturally found in saliva are key factors in the development, progression and prevention of dental caries and periodontal disease.1,41 It is the overall saturation of all three ions (fluoride, calcium and phosphate) found in saliva and oral biofilms that promotes hard tissue remineralization, in turn, reducing the effects of demineralization and susceptibility to further acid attacks.1,41 Combining the buffering capacity of sodium bicarbonate with the remineralization power of fluoride, calcium and phosphate has been shown to increase the acid resistance of enamel and dentin.42,43
It is the clinician’s responsibility to use scientific evidence when making recommendations to patients. Therefore, conversations concerning pH neutralization through means of diet and therapeutic agents can be promoted in the clinical setting as an additional means to restore oral microbial homeostasis and manage dental diseases.
REFERENCES
- Featherstone JD. The science and practice of caries prevention. J Am Dent Assoc. 2000;131:887–899.
- Loesche WJ, Hockett RN, Syed SA. The predominant cultivable flora of tooth surface plaque removed from institutionalized subjects. Arch Oral Biol. 1972;17:1311–1325.
- Loesche WJ. Role of Streptococcus mutans in human dental decay. Microbiol Rev. 1986;50:353–380.
- González-Cabezas C. The chemistry of caries: remineralization and demineralization events with direct clinical relevance. Dent Clin. 2010;54:469–478.
- Kilian M, Chapple IL, Hannig M, et al. The oral microbiome — an update for oral health care professionals. Br Dent J. 2016;221:657.
- Marsh PD. Dental plaque as a biofilm: the significance of pH in health and caries. Compend Contin Educ Dent. 2009;30:76–78.
- Avila M, Ojcius DM, Yilmaz Ö. The oral microbiota: living with a permanent guest. DNA Cell Biol. 2009;28:405–411.
- Marsh PD. Are dental diseases examples of ecological catastrophes? Microbiology. 2003;149:279–294.
- Belibasakis GN, Bostanci N, Marsh PD, Zaura E. Applications of the oral microbiome in personalized dentistry. Arch Oral Bio. 2019;104:7–12.
- Hara AT, Zero DT. The caries environment: saliva, pellicle, diet, and hard tissue ultrastructure. Dent Clin. 2010;54:455–467.
- Stephan RM. Two factors of possible importance in relation to the etiology and treatment of dental caries and other dental diseases. Science. 1940;92:578–579.
- Giacaman RA. Sugars and beyond: the role of sugars and the other nutrients and their potential impact on caries. Oral Dis. 2018;24:1185–1197.
- Featherstone JD. Prevention and reversal of dental caries: role of low-level fluoride. Community Dent Oral Epidemiol. 1999;27:31–40.
- Lingström P, van Houte J, Kashket YS. Food starches and dental caries. Crit Rev Oral Biol Med. 2000;11:366–380.
- König KG. Diet and oral health. Int Dent J. 2000;50:162–174.
- World Health Organization. Guideline: Sugars intake for adults and children. Available at: https://www.who.int/nutrition/publications/guidelines/sugars_intake/en/. Accessed July 17, 2019.
- Moynihan PJ, Kelly SA. Effect on caries of restricting sugars intake: systematic review to inform WHO guidelines. J Dent Res. 2014;93:8–18.
- Bowen WH, Amsbaugh SM, Monell-Torrens SM, Brunelle J. Effects of varying intervals between meals on dental caries in rats. Caries Res. 1983;17:466–471.
- Kalsbeek H, Verrips GH. Consumption of sweet snacks and caries experience of primary school children. Caries Res. 1994;28:477–483.
- Moynihan P, Petersen PE. Diet, nutrition and the prevention of dental diseases. Pub Health Nutr. 2004;7:201–226.
- Burt BA, Eklund SA, Morgan KJ, et al. The effects of sugars intake and frequency of ingestion on dental caries increment in a three-year longitudinal study. J Dent Res. 1988;67:1422–1429.
- Touger-Decker R, van Loveren C. Sugars and dental caries. Am J Clin Nutr. 2003;78:S881–S892.
- Hujoel PP, Hujoel ML, Kotsakis GA. Personal oral hygiene and dental caries: a systematic review of randomised controlled trials. Gerodontology. 2018;35:282–289.
- Bellini HT, Arneberg P, von der Fehr FR. Oral hygiene and caries. A review. Acta Odontol Scand. 1981;39:257–265.
- Hara AT, González-Cabezas C, Creeth J, Parmar M, Eckert GJ, Zero DT. Interplay between fluoride and abrasivity of dentifrices on dental erosion-abrasion. J Dent. 2009;37:781–785.
- Ganss C, Marten J, Hara AT, Schlueter N. Toothpastes and enamel erosion/abrasion — impact of active ingredients and the particulate fraction. J Dent. 2016;54:62–67.
- Joiner A, Pickles MJ, Tanner C, Weader E, Doyle P. An in-situ model to study the toothpaste abrasion of enamel. J Clin Perio. 2004;31:434–438.
- Zero DT, Lussi A. Erosion — chemical and biological factors of importance to the dental practitioner. Int Dent J. 2005;55(Suppl 1):285–290.
- Saxton CA, Cowell CR. Clinical investigation of the effects of dentifrices on dentin wear at the cementoenamel junction. J Am Dent Assoc. 1981;102:38–43.
- Madeswaran S, Jayachandran S. Sodium bicarbonate: a review and its uses in dentistry. Ind J Dent Res. 2018;29:672.
- Aframian DJ, Davidowitz T, Benoliel R. The distribution of oral mucosal pH values in healthy saliva secretors. Oral Dis. 2006;12:420–423.
- Marsh PD, Do T, Beighton D, Devine DA. Influence of saliva on the oral microbiota. Periodontology 2000. 2016;70:80–92.
- Zero DT. Evidence for biofilm acid neutralization by baking soda. J Am Dent Assoc. 2017;148:S10–S14.
- Legier-Vargas K, Mundorff-Shrestha SA, Featherstone JD, Gwinner LM. Effects of sodium bicarbonate dentifrices on the levels of cariogenic bacteria in human saliva. Caries Res. 1995;29:143–147.
- Newbrun E. The use of sodium bicarbonate in oral hygiene products and practice. Compend Contin Educ Dent Suppl. 1997;18:S2–S7.
- Takigawa S, Sugano N, Ochiai K, Arai N, Ota N, Ito K. Effects of sodium bicarbonate on butyric acid-induced epithelial cell damage in vitro. J Oral Sci. 2008;50:413–417.
- Ghassemi A, Vorwerk L, Hooper W, et al. Clinical evaluation of a baking soda dentifrice on gum health. Presented at: International Association for Dental Research/American Association for Dental Research 97th General Session; Vancouver, British Columbia; June 2019.
- Vorwerk L, Ghassemi A, Hooper W, et al. Six-month clinical evaluation of baking soda dentifrices on gum health. Presented at: International Association for Dental Research/American Association for Dental Research 97th General Session; Vancouver, British Columbia; June 2019.
- Bartlett DW, Anggiansah A, Owen W, Evans DF, Smith BG. Dental erosion: a presenting feature of gastro-esophageal reflux disease. Eur J Gastroenterol Hepatol. 1994;6:895–900.
- Armfield JM, Spencer AJ, Roberts-Thomson KF, Plastow K. Water fluoridation and the association of sugar-sweetened beverage consumption and dental caries in Australian children. Am J Pub Health. 2013;103:494–500.
- Rajesh KS, Zareena SH, Kumar MA. Assessment of salivary calcium, phosphate, magnesium, pH, and flow rate in healthy subjects, periodontitis, and dental caries. Contemp Clin Dent. 2015;6:461.
- Tanaka K, Iijima Y. Acid resistance of human enamel in vitro after bicarbonate application during remineralization. J Dent. 2001;29:421–426.
- Kuramochi E, Iizuka J, Mukai Y. Influences of bicarbonate on processes of enamel subsurface remineralization and demineralization: assessment using micro‐Raman spectroscopy and transverse microradiography. Eur J Oral Sci. 2016;124:554–558.
From Decisions in Dentistry. September 2019;5(8):25—30.

