
 ANSAJ/ISTOCK/GETTY IMAGES PLUS
ANSAJ/ISTOCK/GETTY IMAGES PLUS
Managing Dental Trauma: A Review
By periodically reviewing appropriate diagnostic and treatment methods, oral health professionals will be better prepared to render appropriate care when treating dental trauma and related emergencies.
PURCHASE COURSE
This course was published in the September 2019 issue and expires September 2022. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the September 2019 issue and expires September 2022. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Provide an overview of effective management strategies for dental emergencies.
- Discuss appropriate clinical responses when patients present with dental trauma or other oral health emergencies.
- Describe approaches to diagnostic testing and evaluation when treating dental emergencies.
Dental emergencies are commonly associated with toothaches and dental trauma. Many patients do not regularly visit the dentist and the reasons are varied, including cost, lack of access to care, and fear.1 However dental visits become a priority for patients when emergencies arise. This article will review common dental emergencies, endodontic diagnoses, and treatment options for permanent teeth. Although dentists receive training in this area, some clinicians are not comfortable treating dental trauma and refer patients to other providers. In other cases, referrals are made because the dentist cannot determine the source of pain. Ultimately, knowing how to effectively diagnose and treat dental emergencies will lead to better clinical outcomes and greater patient satisfaction.
As with all treatment, a thorough medical and dental history should be completed for all patients. Vital signs should also be recorded. Questions specific to an emergency examination are listed in Table 1.2 An intraoral and extraoral assessment should be completed next. If the emergency is due to trauma, the face or oral cavity can be cleaned with water to visualize damaged tissue. The dentist should make note of swelling, fistulas, mobility, tooth discoloration, wear facets and broken teeth. A periodontal assessment will provide information about tooth restorability and periodontal health. Probing should be completed circumferentially and the presence of purulent exudate should be noted. Mobility, attachment levels and bone loss should be documented. Appropriate radiographs of the tooth or area of chief complaint should be taken. If available, cone beam computed tomography can be useful in dental emergencies involving wisdom teeth, bone pathology and serious injuries, such as fractures of the alveolar ridge.2
TOOTHACHES
Toothaches are a common concern among dental emergency patients. Generally, patients will state the emergency involves pain, swelling, or problems with the integrity of their teeth and restorations.2 If the patient can point to a tooth or there is a broken tooth, determining the cause of the pain should be straightforward. Other times, localizing the source of pain is not as simple. A patient might say a general area is hurting, or even that the pain has been “moving around” to different locations of the oral cavity — and there might not be any obvious signs suggesting the source. A dental abscess might be present, but possibly located between two teeth. At this point, the dentist needs to decide if the toothache is odontogenic in origin; and, if so, accurately determine the tooth, diagnosis and treatment options for the patient.
DIAGNOSTIC TESTING
Diagnostic testing helps determine the pulpal and periapical diagnosis, which, in turn, affects the appropriate course of treatment. Multiple teeth within the quadrant of concern and contralateral side of the mouth should be tested.3 Testing teeth outside the area of concern serves as a baseline by providing a patient’s “normal” response to any given stimulus. It is advisable to test teeth furthest away from the source of pain first, and end with the tooth suspected of causing symptoms last, so the patient will be more relaxed and less likely to provide inaccurate results. Testing multiple teeth allows the clinician to evaluate possible referred pain.
Thermal Testing requires the clinician to apply a hot or cold stimulus to the teeth and evaluate the patient’s response. Cold testing, often done with refrigerant spray, works by causing expansion or contraction of fluid within the dentinal tubules, resulting in movement that stimulates Aδ fibers. Conversely, heat testing stimulates C-fibers.4,5 Heat testing, although less common than cold testing, is useful when the patient complains about pain to hot substances. However, caution must be taken with heat because it is less reliable and can potentially damage the mucosa. Thermal testing is inherently subjective, as it relies on the patient being able to communicate his or her responses accurately, which is not always possible when a patient is anxious, emotional or taking analgesic medications.5 In cases of dental trauma, the distress of the patient, combined with a recently injured pulp, can also lead to false results in thermal testing. The clinician is advised to look for the presence of calcified canals on the radiograph, since these teeth will give no response to cold. Geriatric patients will often provide false negative results due to age-related calcifications.6,7
Electrical Pulp Testers (EPT) help determine if a tooth is vital, and are useful on teeth with calcified canals. These devices function by generating action potentials within the pulpal fibers, which the patient experiences as a tingling sensation.4 If the patient reports feeling an electrical sensation before the EPT reaches its maximum output, the tooth is considered vital.4 As with thermal testing, there is a risk of false responses. A multi-rooted tooth could have necrosis in one part of the tooth, while other areas remain vital. The use of EPTs is also extremely technique sensitive. If the tooth being tested is not completely dry, the electrical current can travel along wet tissue, resulting in a false positive response.8 Additionally, the presence of adjacent metal restorations can cause the current to spread to other teeth.8
Palpation and Percussion provide information about the health of a tooth’s periapical region. When treating dental emergencies, palpation is done to check for swelling, fluctuance, hardness or crepitation of the soft tissues. Percussion sensitivity is suggestive of inflammation in the periodontium.4 Vertical percussion sensitivity suggests an underlying endodontic issue, while horizontal percussion sensitivity typically means the periodontal tissues are involved.
Testing for Cracked Teeth or an incomplete fracture of the dentin is clinically challenging, as these conditions are notoriously difficult to diagnose. The crack might not be clinically evident upon visual or tactile inspection. Patients can present with diverse symptoms, such as pain to biting, cold temperatures or sweets. Transillumination with a fiber-optic light and magnification can help the dentist visualize the crack, and using a Tooth Slooth can help mimic symptoms.9 Pain upon biting or release of a Tooth Slooth is indicative of a cracked tooth.10
INTERPRETING THE RESULTS
Proper diagnosis of a toothache requires understanding the history of the chief complaint, combined with analysis of radiographs, clinical findings and diagnostic tests. Relying on just radiographs or one component of the emergency exam can result in misdiagnosis, incorrect treatment and a patient with unresolved pain. The online version of this article contains tables that provide a helpful clinical review of pulpal and apical diagnoses, along with recommended treatment.11,12
ENDODONTIC AND PERIODONTAL ABSCESSES
Up until this point, this paper has described lesions that are endodontic in origin. Necrotic teeth present radiographically with a periapical radiolucency, showing a breakdown of alveolar bone. Purulence or a sinus tract can also accompany the lesion clinically. This is quite similar to how a periodontal abscess appears.13 Endodontic abscesses usually occur as a result of decay, dental trauma or a failed root canal; the abscess is formed when bacteria and their byproducts exit the apical foramen.14
Periodontal abscesses originate from the periodontium, and purulence will exit from the gingival pocket or other periodontal structures. Teeth with only periodontal abscesses will test vital, and the appropriate periodontal treatment will be necessary — such as removing a foreign object in the sulcus, scaling and root planing, or antibiotic therapy.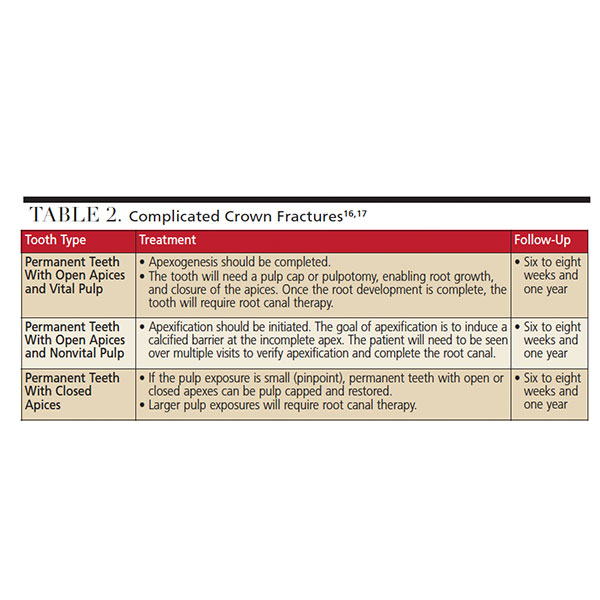
Although more rare than separate lesions, periodontal and endodontic lesions can present simultaneously in a combined lesion. This happens when there is communication between an endodontic lesion progressing toward the crown of the tooth, while a periodontal lesion travels toward the apex. Combined lesions should be treated with both endodontic and periodontal therapy for complete resolution.15
DENTAL TRAUMA AND FRACTURES
Dental trauma should be diagnosed and treated in a timely manner. Treatment depends on the size of the fracture, time elapsed since the trauma, and stage of root development. Diagnostic testing should be completed at the initial appointment, and at follow-up appointments because pulpal status can change in traumatized teeth and may require additional treatment.
Uncomplicated Crown Fractures occur when only part of the dentin and enamel is fractured from the tooth. Initial testing may show no vitality due to transient pulpal damage.16 Treatment includes rebonding the tooth fragment (if possible) or a permanent restoration. If the dentin covering the pulp is less than 0.5 mm thick, a liner should be placed under the restoration.17 The tooth’s prognosis is dependent on any injuries to the periodontal ligament and amount of exposed dentin. Follow-up should be in six to eight weeks and again at one year.17
Complicated Crown Fractures occur when there is an enamel-dentin fracture with pulpal involvement. Radiographically, the apical portion of the fracture might not be visible. Clinically, a portion of the tooth will be fractured off or split with a mobile fragment. Table 2 summarizes complicated crown fractures.16,17
Crown Root Fractures involve enamel, dentin and cementum. Uncomplicated crown root fractures do not have pulpal involvement, while complicated crown root fractures do. The tooth will usually be sensitive to palpation and percussion. A portion of the tooth will be fractured off, or split with a mobile portion. Usually the apical portion of the fracture is not visible, and a successful restorative outcome depends on accessing and sealing the margins of the tooth. Fractures that terminate close to the apex will have a poorer prognosis than fractures closer to the crown. If the fragment is available after an uncomplicated root fracture, it can be repositioned and splinted to adjacent teeth until long-term treatment can be completed. Definitive treatment options include removal of the fragment, gingivectomy (if needed) and restoration, orthodontic or surgical extrusion, decornation, or extraction.16 If the pulp is involved, treatment options are the same as in complicated crown fractures (listed in Table 2).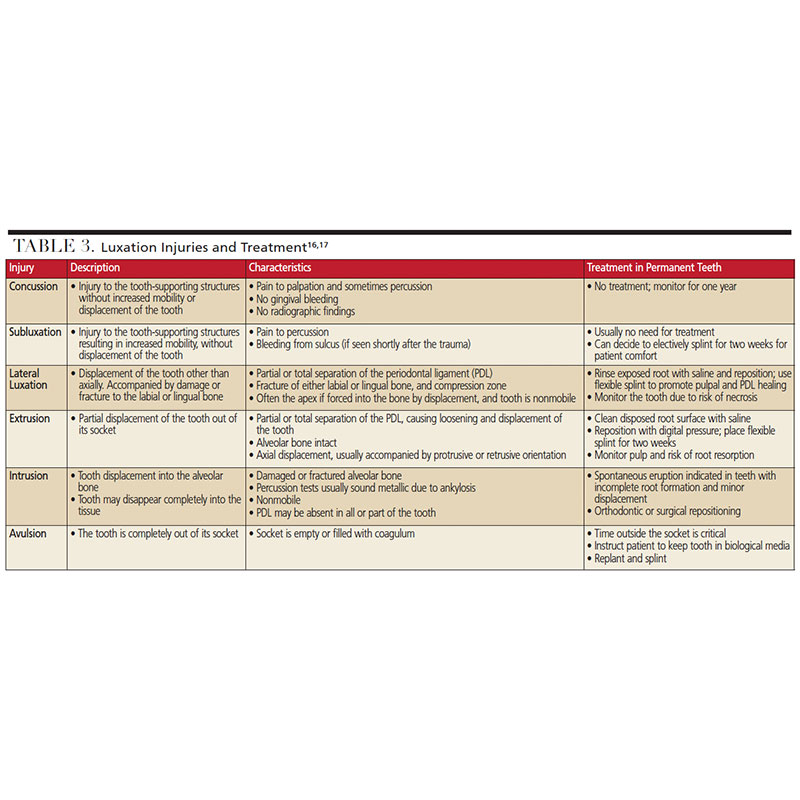
Root Fractures involve the cementum, dentin and pulp. The coronal aspect of the fractured tooth will usually be mobile. Patients will experience sensitivity to palpation and percussion. In situations where the fractured portion of the tooth has not completely avulsed, any exposed portion of the root surfaces should be rinsed with saline and the tooth should be repositioned as soon as possible. A flexible splint should be placed and left on for at least four weeks, and the tooth monitored for pulpal necrosis.17 If the coronal portion of the root becomes avulsed from the socket, treatment for avulsion should be completed, as described in the ensuing luxation injuries discussion.16 Vertical root fractures are difficult to diagnose. A clinical sign of a vertical root fracture is a narrow, deep pocket, and a radiographic sign is a J-shaped radiolucency.18 These teeth are nonrestorable and should be extracted.
Alveolar Fractures in patients with dental trauma may or may not involve the alveolar bone socket. Teeth that are involved in the fracture will be mobile in a unit together, and malocclusion will be present. Treatment requires repositioning the alveolar process manually or with forceps, and stabilizing the fracture by rigid splinting for four weeks, along with monitoring the pulpal status of associated teeth.3,16 The patient should be referred to an oral surgeon to determine if surgical repair of the alveolus is necessary.
LUXATION INJURIES
Luxation injuries occur when a tooth is dislodged, potentially damaging the hard and soft tissues. It is estimated that up to 33% of adults have experienced some kind of luxation injury to their permanent dentition.19 Patients with luxation injuries should be informed that initial treatment is likely to be temporary, and additional treatment may be required due to changes in pulpal status. Table 3 provides a summary of luxation injuries and treatment of permanent teeth.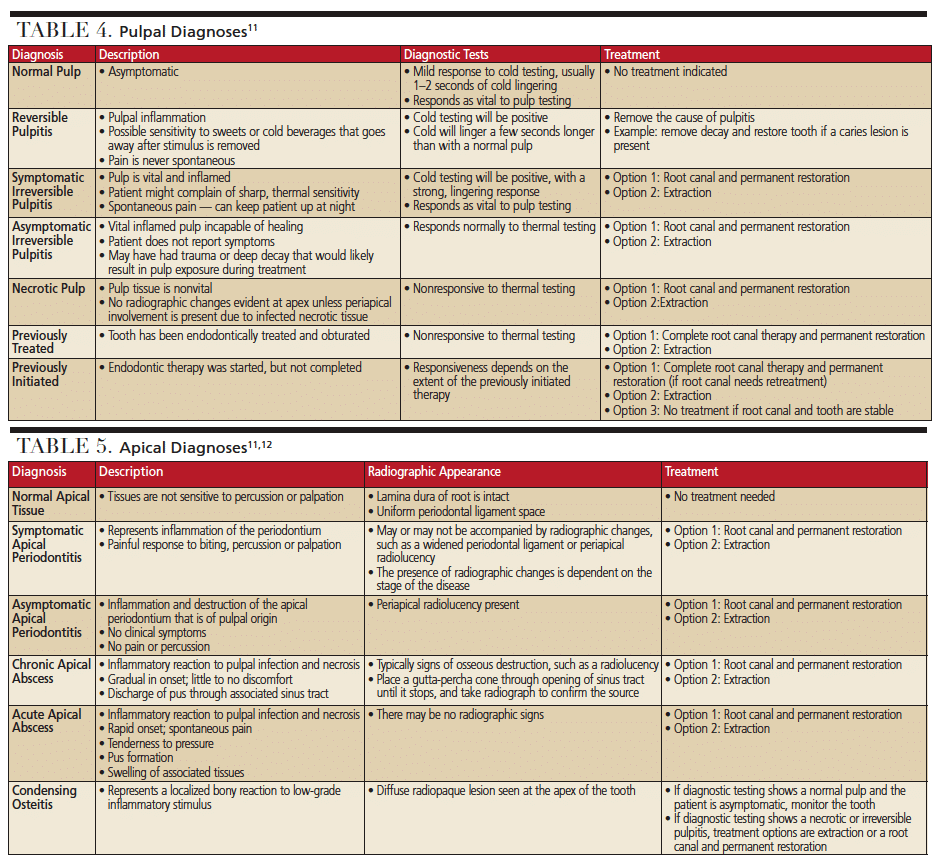
SUMMARY
Patients are often fearful and panicked when faced with dental trauma. In these circumstances, it is the role of the dental team to work with the patient and gather all necessary information from the patient’s history and examination so the dentist can make an accurate diagnosis and develop appropriate treatment options for the emergency. The clinician should also be able to effectively communicate risks, benefits, and the possibility of future treatment related to the event.
By periodically reviewing appropriate responses and diagnoses of dental trauma and related emergencies, dental teams will be better positioned to provide effective care. In short, when faced with dental trauma, being comfortable diagnosing and treating the emergency will lead to more efficient appointments and better clinical outcomes.
REFERENCES
- Wallace BB, Macentee MI. Access to dental care for low-income adults: perceptions of affordability, availability and acceptability. J Commun Health. 2011;37:32–39.
- Greenwood M, Corbett I. Dental Emergencies. Chichester, West Sussex: John Wiley & Sons; 2012.
- American Associaton of Endodontists. Guide to Clinical Endodontics. Available at: https://www.aae.org/specialty/clinical-resources/guide-clinical-endodontics/. Accessed August 1, 2019.
- Levin LG. Pulp and periradicular testing. J Endod. 2013;39(Suppl 3):S13–S19.
- Bender I. Pulpal pain diagnosis — a review. J Endod. 2000;26:175–179.
- Michaelson PL, Holland GR. Is pulpitis painful? Int Endod J. 2002;35:829–832.
- Johnstone M, Parashos P. Endodontics and the ageing patient. Aust Dent J. 2015;60(Suppl 1):20–27.
- Jafarzadeh H, Abbott PV. Review of pulp sensibility tests. Part ΙΙ: electric pulp tests and test cavities. Int Endod J. 2010;43:945–958.
- Mathew S, Thangavel B, Mathew CA, Kailasam S, Kumaravadivel K, Das A. Diagnosis of cracked tooth syndrome. J Pharm Bioallied Sci. 2012;4(Suppl 2):S242–S244.
- Yang Y, Chen G, Hua F, Yu Q, Yang W. Biting pain reproduced by the Tooth Slooth: an aid for early diagnosis of cracked tooth. Quintessence Int. 2019;50:82–87.
- Endodontic Diagnosis. Available at: https://www.aae.org/specialty/wp-content/uploads/sites/2/2017/07/endodonticdiagnosisfall2013.pdf. Accessed August 1, 2019.
- Abbott PV, Yu, C. A Clinical classification of the status of the pulp and the root canal system. Aust Dent J. 2007; 52:17–31.
- Herrera D, Retamal-Valdes B, Alonso B, Feres M. Acute periodontal lesions (periodontal abscesses and necrotizing periodontal diseases) and endo-periodontal lesions. J Clin Periodontol. 2018;45(Suppl 20):S78–S94.
- Robertson D, Smith AJ. The microbiology of the acute dental abscess. J Med Microbiol. 2009;58(Pt 2):155–162.
- Singh P. Endo-perio dilemma: a brief review. Dent Res J (Isfahan). 2011;8:39–47.
- Dental Trauma Guide. Available at: https://dentaltraumaguide.org. Accessed August 1, 2019.
- American Associaton of Endodontists. The Treatment of Traumatic Dental Injuries. Available at: https://www.aae.org/specialty/wp-content/uploads/sites/2/2017/06/ecfe_summer2014-final.pdf. Accessed August 1, 2019.
- Khasnis SA, Kidiyoor KH, Patil AB, Kenganal SB. Vertical root fractures and their management. J Conserv Dent. 2014;17:103–110.
- Diangelis AJ, Andreasen JO, Ebeleseder KA, et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations of permanent teeth. Dental Traumatology. 2012;28:2–12.
From Decisions in Dentistry. September 2019;5(8):32—34,37.

