

Managed Care Plans in Dental Practice: A Commentary
Along with medicine, dental practices may soon be shifting to a health care model that is managed via provider-based incentives associated with quality metrics.
Along with medicine, dental practices may soon be shifting to a health care model that is managed via provider-based incentives associated with quality metrics
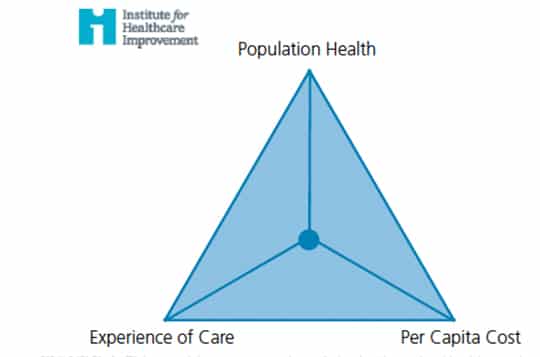
In October 2007, the Institute for Healthcare Improvement launched what is known as the Triple Aim, an initiative that is designed to help health care organizations improve the health of their populations, as well as patients’ experience in terms of quality, access and reliability.1 The initiative was introduced as part of efforts to address the rising cost of health care.2 Pursuing these objectives, it was suggested, would allow health care organizations to identify and fix problems, such as poor coordination of care and overuse of services. It would also help them focus attention and redirect resources to activities and treatments that have the greatest impact on health (Figure 1). Of course, one of the risks of implementing such a system in medical and dental practices is that it could increase costs while creating a dissatisfying patient experience. The underlying challenge is to increase quality while reducing costs — and, at the same time, improving the patient experience. Most of the problems today’s health care system faces relate to the challenge of meeting the initiative’s objectives.
Although the Triple Aim was developed with the intent and focus primarily on medicine, by extension it involves the entire health care system — including dentistry. Although oral health care represents less than 4% of the total cost of health care in the United States, its importance to health is undeniable, and it is thereby essential that dentistry is part of efforts to achieve the initiative’s objectives.
PURPOSE OF MANAGED CARE
One often hears of “managed care” as a means to implement the Triple Aim’s objectives. Recently, the concepts of managed care have been become more known in dental circles. Federally funded and state-managed health systems have challenged Medicaid programs to look at the principles of managed care to achieve the initiative’s goals.
So, what is managed care? While it has many definitions, the common thread is a health care system that is managed to minimize costs.3–5 Although there is nothing particularly new about the idea of managed care (in fact, its origins are more than 100 years old), the concept might still seem foreign to dental practices.
The Institute for Health Improvement describes two types of health care organizations: health maintenance organizations (HMOs) and preferred provider organizations (PPOs). The dental industry is familiar with PPOs, as they have become a mainstay mechanism for commercial insurance reimbursement in the dental insurance market.
There are various ways in which HMOs and PPOs strive to achieve cost reduction in their systems. They might, for example, offer innovative economic incentives to patients and providers to encourage them to select less costly forms of care. This is often done via fee controls to the provider, along with pre-authorizations. In both models, the other main mechanism for achieving cost reduction is via “utilization management.” This means rigorous attention to what is paid for, to what level it is paid, and in what circumstances. There is a need to engage in effective utilization management in order to prevent unnecessary treatment. This is good for the health care professions. Without discussing the values and concerns related to having such a system, there is no question there is a directional change toward these mechanisms in compensating for dental care.
EVOLVING CARE models
In January 2018, the CEOs of three major U.S. corporations, Amazon, Berkshire Hathaway and J.P. Morgan Chase, partnered in an announcement regarding improvements to their health care systems.6 They contended this would allow improvements in health care satisfaction for more than 1 million employees, while also reducing the cost of care. The discussion detailed how the companies would partner to achieve these goals; it also noted the impetus was the rate of cost growth and inability to manage this growth. An emphasis was also placed on the need for high quality transparent care at reasonable cost. Although not specifically mentioned, dental care is included in this directive. What does this mean for dentistry? At present, this is unknown — but looking at the directive’s objectives and its impact on the overall health system suggests major changes in oral health care models.
It was later announced the three corporations have appointed Aton Gawande as the CEO of their new health care business.7 Gawande is the author of Being Mortal: Medicine and What Matters in the End.8 He was charged with the need to focus on cost control, while improving quality and patient satisfaction. As one reads his book, it is clear the emphasis will be on eliminating middlemen, while focusing on how to achieve the Triple Aim’s objectives all at once.
In a guest editorial in the Journal of the American Dental Association, health economist Marco Vujicic noted that our “dental care system is stuck.”9 He discussed trends in health care access and the ever-increasing problem of access to care, particularly for older adults. Vujicic also discussed increasing disparities in access to health care. Cost was cited as the main reason that seniors avoid going to the dentist. In addition, it was mentioned that despite steady reductions in costs to dental care for adults in recent years, there has not been an appreciable change in utilization. While children have achieved good access across the nation for oral health services, this is not the case for adults, and particularly older adults.
Vujicic discussed significant reforms needed to create major expansions in dental care utilization and, most importantly, improvements in oral health. He described the need to address the dental coverage gap, the need to define and systematically measure oral health via development of quality metrics, and the use of such metrics to create a reimbursement system that is tied to outcomes. Vujicic also suggested that to bring oral care into the realm of total health, it is essential that stakeholders also talk about tying care costs together between oral health and total health. This discussion has already taken place, for example, for conditions such as diabetes and periodontal disease.10
The Journal of the American Dental Association published an editorial in its July 2018 issue that followed on Vujicic’s piece. In the article, Glick11 discussed the relevance of oral health in achieving overall health, and suggested this may be a “linchpin for acceptance for primary health care professionals in substantiating its impact on patient care.” He states the “emphasis on the procedural aspects of dentistry as the essential element of our identity as dentists” must shift to the more important outcome of how this care effects overall health. It is the extent to which the profession adheres to this latter point that will give oral health care equal status in the perception of overall health.
This cannot be achieved without an understanding of the inextricable connection between the costs associated with oral health and overall health. Glick also discusses the “tsunami” of information coming our way, and the need to synthesize information into clinical decision-making that relates to health and disease management, as well as health maintenance. This is opposed to a historical focus primarily on treatment outcomes, without the ability to specifically manage the disease itself. Yet, the payer system compensates and rewards treating the results of disease, rather than managing the disease itself. This is not fault of providers or the health care professions, but of a system of care that must inevitably change.
REVISITING THE DEFINITION
The literature goes into further detail in elucidating the purpose of managed care beyond just globally reducing costs. It discusses the need to reduce unnecessary health costs via a variety of mechanisms, including providing economic incentives for providers and patients so less costly forms of care that achieve similar or better outcomes are chosen. In addition, there is a need to create programs reviewing the medical necessity of specific procedures by more carefully reflecting on the likely outcome of such therapy. And, finally, a higher level of management needs to be directed toward high-cost health care cases in which some form of reimbursement is in play.
In looking at this broader definition of managed care, it is apparent that dentistry is not the same as other parts of health care. The differences lie in the layering of systems in the larger health care model, particularly given the existence of large hospital organizations, provider organizations, and in the pharmacy distribution business (as well as in the pharmaceutical business as a whole). Therefore, it is not possible to equate the need for specific changes in the overall system with those in dentistry. However, it is easy to see where dental practices can learn from the global system while taking advantage of the strengths of a “flatter” health care organization structure.
IMPORTANCE OF SHIFTING COST RISKS
The ability to reduce costs as an objective of a managed care plan (and of the Triple Aim) is only achievable when one looks at who bears the cost risk in various aspects of the system.
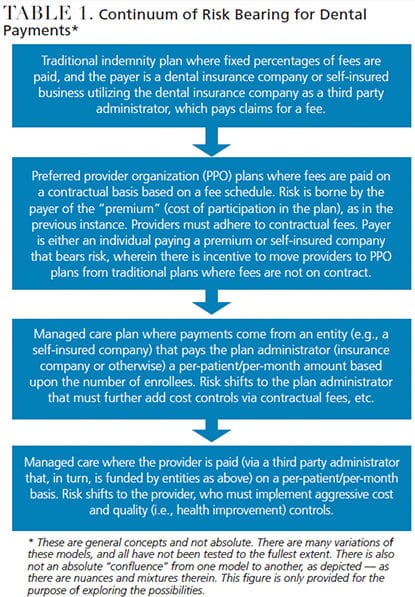 Stakeholders can look at the payer system in dentistry as a continuum (Table 1) in which on the historical side there was no dental insurance: Everything was fee-for-service based and paid out of pocket. Next, dental insurance became available (along with dental Medicaid in certain circumstances). Individual insurance plans provided compensation for most preventive dental care and some restorative care.
Stakeholders can look at the payer system in dentistry as a continuum (Table 1) in which on the historical side there was no dental insurance: Everything was fee-for-service based and paid out of pocket. Next, dental insurance became available (along with dental Medicaid in certain circumstances). Individual insurance plans provided compensation for most preventive dental care and some restorative care.
As costs have grown in the system, the reimbursement rates have gone down in actuality and, relatively speaking, this is impacted by the cost of inflation. In addition, as large corporations have become entirely self-insured for their medical and dental plans, they bear most of the cost risk (this was described by Bezos et al in the January 2018 Amazon, Berkshire Hathaway and J.P. Morgan Chase announcement). Therefore, they are the ones negotiating the fees and inexorably driving the managed care concept, including the growth of PPO organizations in dentistry. Based essentially on the principles of the Triple Aim, these large companies need to satisfy their employees by providing high-quality care, while also reducing the cost of care.
Dentistry’s needs are no different. With the growth of self-insured programs leaving the risks to those organizations, the next step would be for them to ask for stronger means to transmit risk from what are now commercial insurance entities to providers themselves. It is the shifting of risk that might create what some define as managed care in the truest sense. Ideally, if the risk is shifted in a way that compensation to providers could be earned while absorbing the risk — and thereby incentivizing clinicians to improve patients’ health through quality metrics — the ideals of managed care would be manifested in their purest form. This is not an assessment of the system, but, rather, a statement of the realities that may be in play.
DISCUSSION
The purpose of this paper is not to explore the advantages and disadvantages of a managed care plan, but, rather, to introduce the global concept and discuss the elements of risk associated with managed care. It is precisely shifting the risk for care and reimbursement — where traditional dental payment models transition to a scenario in which large corporations drive the PPO business through their self-insured perspective — that will help achieve the goals of the Triple Aim initiative.
Ultimately, just as is occurring in state organizations that are implementers of federally funded Medicaid programs (where the systems are shifting to managed care in which third-party contractees are paid on a per-patient/ per-month basis and risk is shifted from the state), the next step would be to directly compensate providers on a per-patient/ per-month basis. This would give dental practices a stronger incentive to improve patient health, as measured by the development and use of quality metrics.
Look for further studies and commentary as tests are performed on the commercial side of the business designed to evaluate health care systems managed via provider-based incentives associated with risk adoption and quality metrics.
KEY TAKEAWAYS
- The Institute for Healthcare Improvement’s Triple Aim objectives are designed to contain costs while helping health care organizations improve the health of their populations, as well as the patient’s experience in terms of quality, access and reliability.1
- The purpose of managed care is to focus attention and redirect resources to activities and treatments that have the greatest impact on health.
- Although oral health care represents less than 4% of the total cost of health care in the United States, its importance to health is undeniable, and it is thereby essential that dentistry is part of efforts to achieve the Triple Aim’s objectives.
- While managed care has many definitions, the common thread is a health care system that is managed to control costs.3–5
- There is a need to engage in what’s known as effective utilization management in order to prevent unnecessary treatment.
- In a guest editorial in the Journal of the American Dental Association, health economist Marco Vujicic discussed the need to address the dental coverage gap, the need to define and systematically measure oral health by developing quality metrics, and using these metrics to create a reimbursement system that is tied to outcomes.9
- In order to bring oral care into the realm of total health, it is essential that stakeholders begin to talk about tying care costs together between oral health and overall health.
REFERENCES
- Institute for Healthcare Improvement. Inititiaves. IHI Triple Aim Initiative. Available at: ihi.o/ g/ Engage/ Initiatives/ TripleAim/ Pages/ default.aspx. Accessed January 10, 2019.
- The Commonwealth Fund. The Triple Aim Journey: Improving Population Health and Patients’ Experience of Care, While Reducing Costs. Available at: commonwealthfund.org/ publications/ case-study/ 2010/ jul/ triple-aim-journey-improving-population-health-and-patients. Accessed January 10, 2019.
- Howard SW, Burnell SL, Yoon J, Luck J, Ranit CM. Oregon’s experiment in health care delivery and payment reform: coordinated care organizations replacing managed careJ J Health Polit Policy Law. 2015;40:245–255.
- Topaloglu-Ak A, Eden E, Frencken JE. Managing dental caries in children in Turkey — a discussion paper. BMC Oral Health. 2009;25:32.
- Fisher MA, Mascarenhas AK. A comparison of medical and dental outcomes for Medicaid-insured and uninsured Medicaid-eligible children: a U.S. population-based study. J Am Dent Assoc. 2009;140:1403–1412.
- Business Wire. Amazon, Berkshire Hathaway and JPMorgan Chase & Co. to partner on U.S. employee healthcare. Available at: businesswire.com/ news/ home/ 20180130005676/ en/ Amazon-Berkshire-Hathaway-JPMorgan-Chase-partner-U.S. Accessed January 10, 2019.
- Reuters. Amazon, Berkshire, JPMorhan name Atul Gawande CEO of healthcare venture. Available at: reuters.com/ article/ us-berkshire-buffet-healthcare/ amazon-berkshire-jpmorgan-name-ceo-for-healthcare-venture-idUSKBN1JG1WZ. Accessed January 10, 2019.
- Gawande A. Being Mortal: Medicine and What Matters in the End. New York, New York: Metropolitan Books; 2014.
- Vujicic M. Our dental care system is stuck. J Am Dent Assoc. 2018;149:167–169.
- Nasseh K, Vujicic M, Glick M. The relationship between periodontal interventions and healthcare costs and utilization. Evidence from an integrated dental, medical, and pharmacy commercial claims database. Health Econ. 2017;26:519–527.
- Glick M. Dentistry at a crossroads. J Am Dent Assoc. 2018;149:565–566.
The author discloses that he consults for MCNA Dental, DMG America and Hu-Friedy.
Featured image by PAUL BRADBURY/OJO IMAGES/GETTY IMAGES PLUS
From Decisions in Dentistry. February 2019;5(2):17—20.
