

Proper Glove Use Prevents Spread of Infectious Diseases
As a key element of personal protective equipment, gloves provide an important barrier to contact transmission in dental settings.
As a key element of personal protective equipment, gloves provide an important barrier to contact transmission in dental settings
Oral health professionals are at daily risk of exposure to infectious diseases, and gloves provide an important barrier to contact transmission. Knowing how to perform proper hand hygiene, choosing the right gloves, and following recommended protocols for glove use will help keep clinicians and patients safe and healthy. The federal government has created regulations and recommendations to prevent disease transmission and promote safe health care. The Occupational Safety and Health Administration (OSHA) was created in 1970 to protect workers’ health and safety. In 1987, regulations for chemical safety were addressed with the addition of the Hazard Communication Standard and, in 1991, the Bloodborne Pathogens Standards — designed to protect against bloodborne pathogens — were finalized.
The U.S Centers for Disease Control and Prevention (CDC) develops guidelines and recommendations to protect clinicians and patients. Infection prevention in dentistry is largely based on the CDC’s Guidelines for Infection Control in Dental Health-Care Settings — 2003. In 2016, a companion document was released that provides a summary of the 2003 guidelines, plus new recommendations. In addition to these protocols, OSHA and the CDC continue to develop regulations and recommendations, respectively, to ensure the delivery of safe care.
EVALUATE THE RISK
In dental settings, gloves are a key element of the personal protective equipment mandated by OSHA. They are used to protect the wearer and patient from the spread of illness and infectious diseases during examinations and other procedures. Gloves provide an essential layer of barrier protection against direct contact with infectious agents that are transmitted during exposure to blood, saliva, contaminated objects and surfaces.
With more than 700 species of microbiota found in the oral cavity,1 and the ability of some pathogens — such as methicillin-resistant Staphylococcus aureus — to live on a surface for up to seven months,2 oral health professionals are well advised to adhere to the basic principles of infection prevention.
Glove quality and integrity matter; consequently, the U.S. Food and Drug Administration (FDA) regulates the manufacturing and labeling of medical devices, including gloves. It also ensures that performance criteria — such as leak resistance, tear resistance and biocompatibility — are met. While the efficacy of gloves in reducing bloodborne pathogen transmission has been well established,3 they do not provide 100% protection. When manufactured, new gloves will experience a small percentage of allowable defects, such as micro-tears, that may allow exposure to blood or saliva. As such, performing hand hygiene after glove removal is imperative. In addition, glove integrity decreases over time, with the incidence of failure increasing between 30 minutes and three hours of use.4 Changing gloves during longer procedures will reduce the risk of contact transmission. Oral health professionals may also wish to consult manufacturers’ guidelines regarding the chemical compatibility of glove material and the dental materials being used.5
In 2016, the FDA banned the use of powdered surgical and patient exam gloves after determining that powder posed risks, including possible airway inflammation, hypersensitivity reactions, granulomas, and scar tissue formation.6 No remaining glove stock with powder should be used.

GLOVE TYPES AND INDICATIONS
Most patient-care gloves are made of natural rubber latex or synthetic materials, such as nitrile or vinyl. These may either be ambidextrous (fitting both hands), or fitted, which are right- and left-hand specific. Ambidextrous gloves may contribute to repetitive stress injuries, while hand-specific gloves typically offer better fit and comfort, while reducing hand and wrist strain.7
Single-Use Disposable Patient Care Gloves: Exam gloves are used for examining patients and performing procedures that involve contact with mucous membranes. They are not intended for surgical procedures. Surgical gloves are sterile gloves that should be used for all oral surgical procedures. A surgical hand wash must be performed before donning these gloves. Individually packaged pairs are offered in hand-specific designs and sizes.
Nonpatient Care Utility Gloves: Heavy-duty utility gloves are a vital, but often underutilized, type of personal protective equipment. They are not used for direct patient care. Both OSHA and CDC indicate that chemical- and puncture-resistant utility gloves should be worn when processing contaminated instruments and performing housekeeping duties (e.g., cleaning and disinfecting) and other tasks involving chemicals.8 Heavy-duty utility gloves offer significant protection against both percutaneous injury and chemical exposure. Typically made of nitrile or neoprene, they should be washed and disinfected after use. Some types may be heat sterilized, and this would be indicated in the manufacturer’s instructions for use. Heavy-duty utility gloves are not considered a medical device; therefore the FDA does not regulate manufacturing standards. Oral health professionals should have their own pair of well-fitting utility gloves.9 Utility overgloves are similar to food-handling gloves. They may be worn over contaminated exam gloves to prevent cross-contamination when clinicians need to handle an item during patient care (such as retrieving a hand mirror from a drawer, for example).
MAKE THE BEST CHOICE
Choose the best glove for the task based on the following considerations:
- The task at hand: Gloves should be chosen based on the procedure to be performed (e.g., patient exam or surgery).
- Material: This is largely a matter of clinician preference, and both latex and nonlatex gloves are available.
- Skin sensitivity: When choosing gloves, consider latex or nitrile allergies.
- Size: Offices should have a variety of glove sizes available to their team members.
- Fit: A snug but comfortable fit is best. If too large, gloves may impede dexterity and task performance. If too small, they may cause hand discomfort.
- Ambidextrous or hand-specific gloves: This choice is based on clinician preference, while also considering the length of the procedure.
- Tactile sensation: Sensitivity should not be significantly reduced; consider grip, glove thickness, and if the material will be slippery when wet.
SAFE GLOVE USE
Hands are the main pathway of disease transmission. Hand hygiene is the most effective way to prevent the spread of infection, thus it must always be done prior to gloving.8 Routine handwashing with antiseptic hand wash, the use of antiseptic hand rub, or surgical hand antisepsis are all types of hand hygiene.10 Oral health professionals involved in patient care must be able to perform this task correctly and at the right time. The use of gloves never replaces the need for cleaning hands.
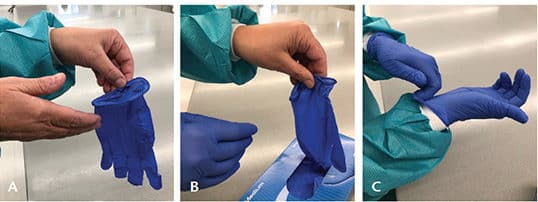
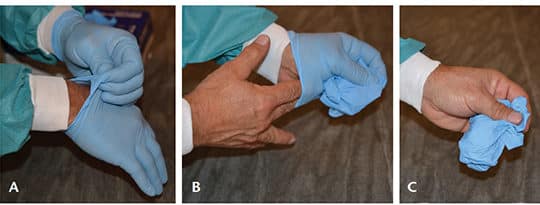
Safe glove use includes appropriate technique when donning and doffing gloves (Figure 1 and Figure 2).11 Gloves are the last item of personal protective equipment donned prior to patient treatment, and their removal follows a specific sequence. If any of these steps are not followed correctly, there is a high risk of contact transmission. Gloves must never be reused.
During treatment, a clinician must occasionally leave a patient to retrieve an instrument or device. If gloves are not removed, cross-contamination can occur when touching other surfaces or items. Removing just one glove means that pathogens on that hand could transfer to clean items. The best options are to use a cover glove, or remove both gloves, perform hand hygiene, and then retrieve the item.
Healthy, intact skin is the best defense against pathogen transmission and infectious diseases. Selection and use of appropriate medical-grade moisturizers and other hand hygiene products are warranted. In an effort to prevent dryness and contact dermatitis caused by frequent hand hygiene, clinicians often apply lotions. However, lotions with a petroleum-base can hinder the effectiveness of latex gloves.10 Therefore, oral health professionals should consider using only water-based lotions during the workday.
Adverse skin conditions can develop due to glove use, chemical exposure and repeated hand hygiene. Allergies and sensitivities related to gloves should be evaluated by an allergist or dermatologist to pinpoint the cause and direct a course of treatment.
Long nails and hand jewelry can interfere with proper glove selection, cause difficulty when donning, and are likely to create tears or punctures. Artificial nails are not recommended, as they have been linked to outbreaks of bacterial infections. Natural nail tips should be kept less than a ¼ inch long.12
While shelf life varies by glove type and manufacturer, gloves stored in areas with considerable moisture, light or heat are likely to degrade more quickly than those stored in more favorable environments.
CONCLUSION
Gloves are a critical component of personal protective equipment necessary for protection against bloodborne pathogens and exposure to other harmful microorganisms. Proper hand hygiene, along with the correct use of gloves, will dramatically reduce the likelihood of infectious transmission for both practitioners and patients. Dental team members must have a clear understanding of appropriate glove use in order to be confident they are providing safe and effective care.
KEY TAKEAWAYS
- Knowing how to perform proper hand hygiene, choosing the right gloves, and following recommended protocols for glove use will help keep clinicians and patients safe.
- Glove use is a key element of the personal protective equipment mandated by the federal Occupational Safety and Health Administration.
- While the efficacy of gloves in reducing bloodborne pathogen transmission has been well established,3 they do not provide 100% protection. Thus, performing hand hygiene after glove removal is imperative.
- Glove integrity decreases over time, with the incidence of failure increasing between 30 minutes and three hours of clinical use.4
- Changing gloves during longer procedures will reduce the risk of contact transmission.
- Gloves may either be ambidextrous (fitting both hands), or fitted, which are right- and left-hand specific.
- Hand-specific gloves typically offer better fit and comfort, while reducing hand and wrist strain.7
- Chemical- and puncture-resistant utility gloves should be worn when processing contaminated instruments and performing housekeeping duties (e.g., cleaning and disinfecting) and other tasks involving chemicals.8
REFERENCES
- Aas JA, Paster BJ, Stokes LN, Olsen I, Dewhirst FE. Defining the normal bacterial flora of the oral cavity. J Clin Microbiol. 2005;43:5721–5732.
- Kramer A, Shwebke I, Kamft G. How long do nosocomial pathogens persist on inanimate surfaces? A systematic review. BMC Infect Dis. 2006;6:130.
- Bardorf MH, Jäger B, Boeckmans E, Kramer A, Assadian O. Influence of material properties on gloves’ bacterial efficacy in the presence of microperforation. Am J Infect Control. 2016;44:1649–1649.
- Partecke LI, Goerdt AM, Langner I, et al. Incidence of micro perforation for surgical gloves depends on duration of wear. Infec Control Hosp Epidemiol. 2009;30:409–414.
- Kohn WG, Collins AS, Cleveland JL, et al. Guidelines for Infection Control in Dental Health-Care Settings — 2003. MMWR Recomm Rep. 2003;52(RR-17):1–76.
- U.S. Food and Drug Administration. Medical Device Bans. Available at: fda.gov/medicaldevices/safety/medicaldevicebans/default.htm. Accessed January 10, 2019.
- Organization for Safety, Asepsis and Prevention (OSAP). OSHA and CDC Guidelines: OSAP Interact Training System Workbook. Atlanta: OSAP; 2017.
- Summary of Infection Prevention Practices in Dental Settings: Basic Expectations for Safe Care. Atlanta: U.S. Centers for Disease Control and Prevention; 2016.
- Miller CH, Palenik CJ. Infection Control and Management of Hazardous Materials for the Dental Team. 6th ed. St. Louis: Elsevier; 2018.
- U.S. Centers for Disease Control and Prevention. Frequently Asked Questions — Hand Hygiene. Available at: cdc.gov/OralHealth/infectioncontrol/faq/hand.htm. Accessed January 10, 2019.
- World Health Organization. Glove Use Information Leaflet. Available at: who.int/gpsc/5may/Glove_Use_Information_Leaflet.pdf. Accessed January 10, 2019.
- Boyce JM, Pittet D, Healthcare Infection Control Practices Advisory Committee. Society for Healthcare Epidemiology of America. Association for Professionals in Infection Control. Infectious Diseases Society of America. Hand Hygiene Task Force. Guideline for hand hygiene in health-care settings: recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Infect Control Hosp Epidemiol. 2002;23(Suppl 12):S3–S40.
Featured image by DEMAERRE/ISTOCK/GETTY IMAGES PLUS
The author has no commercial conflicts of interest to disclose.
From Decisions in Dentistry. February 2019;5(2):21—24.
