
Maintaining Implant Supported Hybrid Prostheses
A discussion of clinical considerations for maintaining implant supported hybrid prostheses and managing potential complications.
PART 2 of a two-part series This is the concluding installment of a two-part series. Appearing in June 2020, the first installment, “Implant Treatment Planning for Hybrid Prostheses,” explored planning, placement and restoration of implant supported hybrid prostheses. Part 2 will focus on maintaining these prostheses and managing complications.
Since Brånemark’s discovery of osseointegration, full-arch fixed implant prostheses have ranked among the best treatment options to restore function, esthetics and phonetics for patients affected by edentulism of at least one complete arch. Adequate diagnosis and treatment planning are quintessential to ensure predictable surgical and restorative outcomes when using this treatment modality. The planning, placement and restorative phases for hybrid prostheses are discussed in the first article of this two-part series, “Implant Treatment Planning for Hybrid Prostheses,” available at decisionsindentistry.com.1
Due to the complex nature of full-arch, implant supported fixed prostheses — also known as hybrid prostheses — it is crucial for the patient and treating clinician to engage in a strict, long-term maintenance plan that allows adequate follow-up and early detection of possible complications. This concluding installment in the series will explore clinical considerations for maintaining these restorations and managing any complications that arise.

CUSTOMIZE PLANS FOR EACH PATIENT
The long-term maintenance plan should be customized to meet each patient’s specific needs. This plan consists of in-office maintenance visits and adequate self-care.2 Factors to consider when developing a long-term maintenance plan include (but are not limited to) clinical findings, such as bleeding on probing (BOP), periodontal probing depth (PD), and clinical attachment loss; response to past therapies; behavioral factors, such as oral hygiene practices, smoking and nutrition; and environmental factors, such as socioeconomic status.
Etiology of Tooth Loss — Patients who lost their teeth due to periodontal disease might have a higher risk of developing peri-implant complications than patients who lost their teeth to extensive caries, defective restorations or trauma.2 The frequency of follow-up appointments should be adjusted for patients at higher risk, at least for the first year postdelivery of the final prosthesis, after which maintenance frequency should be reevaluated.
Patient Self-Care — Proper patient hygiene instruction is essential upon delivery of the provisional and final prostheses. The use of a suitable self-care armamentarium should also be discussed. Options include electric toothbrushes, water flossers, implant brushes, interproximal brushes, floss threaders and other flossing products.3 The frequency of in-office maintenance visits must be increased for individuals who struggle to maintain satisfactory self-care.4
Prosthetic Design and Restorative Material — Adequate design of the prosthetic appliance plays a major role in long-term maintenance and proper cleansability. The intaglio surface of the prosthesis must be highly polished and free of concavities, thus providing a convex surface in light contact with the soft tissue (Figures 1A and 1B). This light pressure creates a seal to prevent food accumulation and airflow between the prosthesis and residual ridge that could lead to speech difficulties. Such contact should allow adequate access of hygiene appliances.
Regardless of the material chosen — for example, titanium/poly(methyl) methacrylate (PMMA) or zirconia — the final prosthesis must be highly polished to minimize plaque adhesion and calculus formation. Ceramic restorative materials, such as monolithic zirconia, maintain surface properties over time when compared to PMMA resin. Such material selection has an impact on maintenance appointments and calculus accumulation, as patients are typically better able to maintain zirconia surfaces with self-care compared to acrylic.5,6
Prostheses should be retrievable by providing access to the prosthetic screws, allowing the clinician to remove the appliance when necessary for maintenance appointments. Screw access channels can be covered with polytetrafluoroethylene tape and composite resin to prevent food impaction into the channel.7
In-Office Maintenance Appointments — These visits are a pillar that supports the long-term success of implant treatment. In addition to completing hygiene procedures, they provide the opportunity to identify and solve potential complications in their earliest stages.
During hygiene visits, the clinician can evaluate the patient’s proficiency at self-care and determine if the frequency of maintenance visits should be increased. While scheduling maintenance appointments every six months is recommended, patients with poor self-care should be seen more often.2

During maintenance visits, clinicians should conduct a clinical and radiographic examination of the implants, prosthetic appliances, and condition of the soft tissues. Implant probing should be completed during maintenance appointments, recording PD and BOP. This exam will help detect peri-implant mucositis or early signs of peri-implantitis, and provide an opportunity for prompt treatment — thus increasing the probability of long-term implant success.8
Removal of the implant fixed prostheses during maintenance appointments is contingent upon the patient’s plaque control. The presence of plaque or calculus on the surface of the prosthesis or prosthetic abutments is an indicator for the need to remove the appliance. When removed, the prosthesis must be mechanically cleaned to remove plaque, placed in an ultrasonic bath (tartar and stain remover solution might be used), resurfaced if any concavities or inadequate contours are present, and polished to achieve a high-shine surface and prevent further plaque accumulation.9
When reinstalling the prosthesis, clinicians should consider utilizing new prosthetic screws (following manufacturer instructions) to maintain adequate torque and prevent screw fractures.
MANAGING COMPLICATIONS
The etiology of complications occurring to implant fixed full-arch prostheses varies. In general terms, complications could be mechanical, biologic, or a combination of both.
Mechanical and Prosthetic Complications — Mechanical complications affecting hybrid prostheses include screw loosening, screw fractures, implant fractures, framework/resin/veneering material fractures, tooth wear, implant prosthesis fractures, opposing prosthesis fractures, and metal framework fractures.10–14
Metal framework fracture has been attributed to inadequate metal thickness, excessive cantilever length, poor selection of dental alloys, parafunctional habits, and improper framework design.10,12,15–17 Fracture of the metal framework is a catastrophic failure that requires remaking the prosthesis. Framework design, material selection and thickness must be reassessed when dealing with this complication.
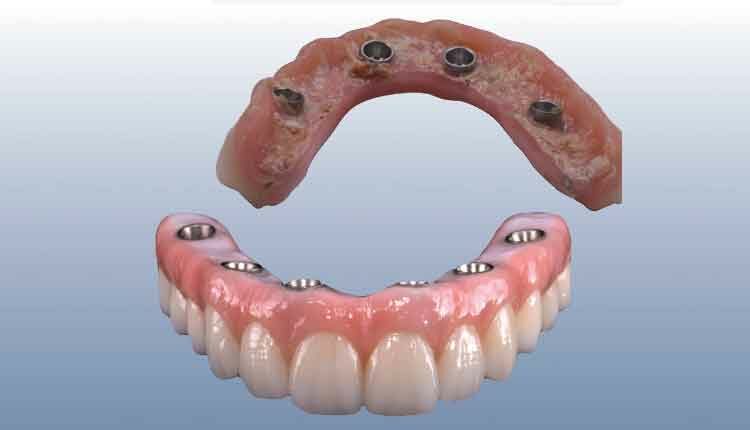
Hybrid prostheses’ most common complications involve the interface between the prosthetic teeth, acrylic resin and metal framework. These complications include acrylic resin and tooth wear, prosthetic teeth debonding and fracture, and delamination of the veneering material (Figure 2).10,12,15,16
Tooth fracture and debonding could be strongly related to an inadequate occlusal scheme or working interferences. This is especially true when fracture happens shortly after prosthetic installation. Occlusion should be reevaluated and adjusted if necessary. Prosthetic tooth wear occurs over time (an average of five years),15 and is influenced by opposing arch occlusion, as well as the patient’s habits and possible parafunctions. When teeth need replacement, the metal framework is maintained, worn prosthetic teeth are removed, and a new set of teeth is processed.
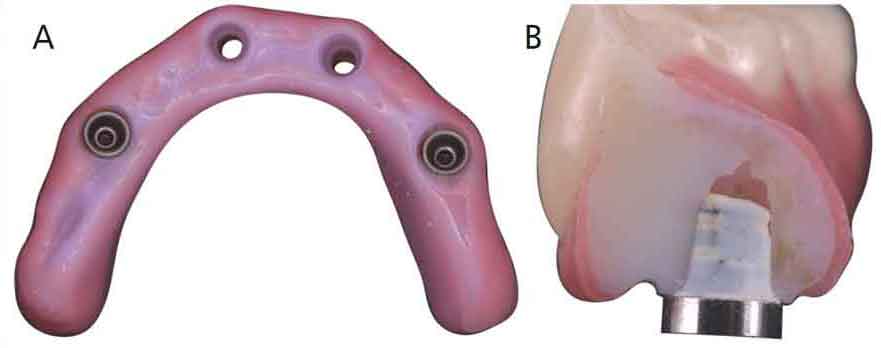
Some of the complications observed in zirconia prostheses include porcelain delamination (when nonfunctional porcelain layering is done), opposing denture teeth debonding or fracture, titanium abutment debonding, and prosthetic fracture (Figures 3A and 3B).18–25 Porcelain delamination can be solved by removing the prosthesis and returning it to the laboratory for porcelain relayering. Abutment debonding can be solved by re-bonding either intraorally, or on the model (which is the preferred method to ensure adequate control of excess cement).

A fracture of a zirconia prosthesis supposes a catastrophic failure and the only solution is to remake the prosthesis. Possible causes include lack of passive fit, poor prosthetic design, insufficient material volume, insufficient prosthetic height, excessive cantilever, and uncontrolled parafunction. Such causes must be taken in consideration when remaking the prosthesis to prevent subsequent failure.
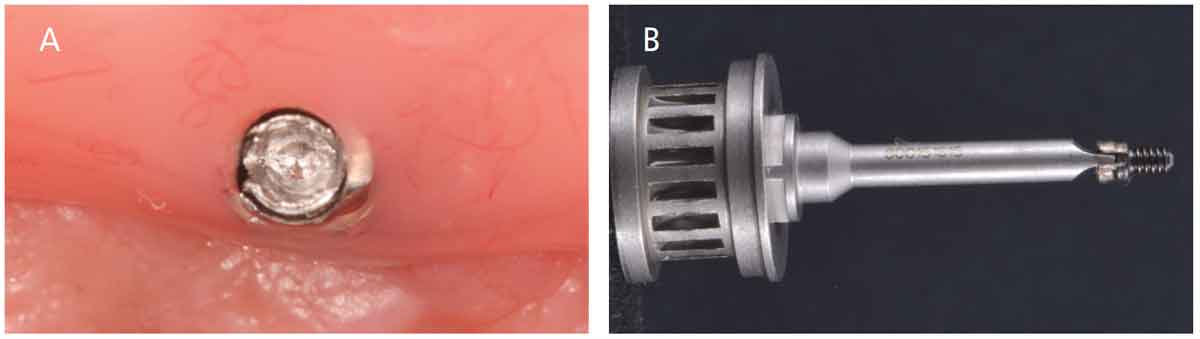
Another possible mechanical complication is screw stripping or fracture, which could be discovered when removing the prosthesis during a maintenance visit. When the prosthetic screwhead is stripped, the screwdriver will not engage. Reverse-torque kits designed to remove stripped screws are available; alternately, a fine fissure bur mounted on a high-speed handpiece can be used to carefully create a slot and utilize a flat screwdriver to remove the screw (Figures 4A and 4B). Fractured screws are generally easier to remove because the torque has been lost; they can be reversed with an explorer, wooden tip, or an instrument provided in the above-mentioned retrieval kits (Figure 5).
Phonetic and esthetic complications could be observed, and are more frequently encountered on maxillary (rather than mandibular) prostheses. Patients who have undergone excessive resorption of the anterior maxilla and those who have improper prosthesis-tissue contact could have air escape during speech, in which case the tissue contact should be adjusted. Most patients fully adapt to the shape and position of the prosthesis and have no speech impediments within three to six months after installing the prosthetic appliance.10,26

Biologic Complications — Implants can be affected by peri-implant disease, such as peri-implant mucositis and peri-implantitis.
Peri-implant mucositis is defined as “an inflammatory lesion of the soft tissues surrounding an endosseous implant in the absence of loss of supporting bone or continuing marginal bone loss.”27 Diagnosis of peri-implant mucositis comprises BOP without bone loss. This condition is caused by accumulation of biofilm and/or calculus around the implants. It is a reversible condition that can be treated during maintenance appointments by removing biofilm and calculus. Hygiene measures should be reinforced at this time, and use of adjuncts (such as chlorhexidine mouthrinse) could be indicated. If left untreated, peri-implant mucositis could evolve to peri-implantitis once there is bone loss around the implants; hence the importance of maintenance appointments to provide early treatment and prevent further damage to the peri-implant supporting tissues.
Peri-implantitis is defined as “a pathological condition occurring in tissues around dental implants, characterized by inflammation in the peri-implant connective tissue and progressive loss of supporting bone.”28 Patients affected by peri-implantitis should be evaluated for possible treatment, which might include open debridement, implant decontamination, implantoplasty, regeneration, or a combination of these procedures (Figures 6A through 6C). Accurate, timely and recurrent PD and BOP records will help the provider diagnose, treat, and follow-up on implants affected by peri-implant disease.8
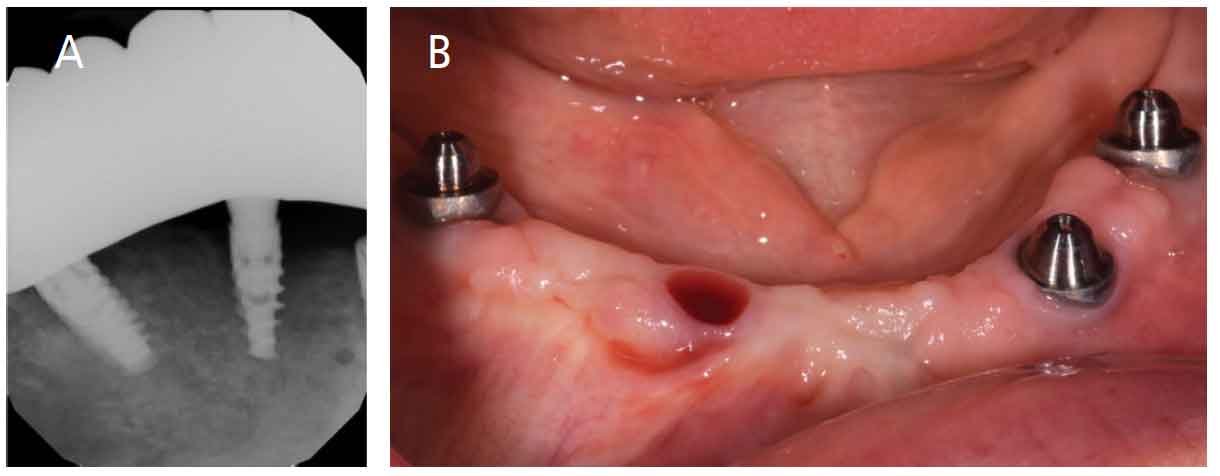
When bone loss continues around implants to the point where peri-implantitis treatment is not predictable and/or osseointegration is lost, implants should be removed (Figures 7A and 7B). New implant placement could be considered and discussed with the patient. Depending on the etiology of implant failure, healing time or regenerative procedures could be deemed necessary prior to implant placement. After failed implants are replaced, a new prosthesis must be made to accommodate the new implants.
SUMMARY
The utilization of implant supported hybrid prostheses is a remarkable treatment option to restore function and esthetics for edentulous patients. Care must be exercised during every step of treatment to provide the best possible restorative outcome. Exceptional planning and execution of each phase of therapy, patient education, and recurring maintenance are the keys to treatment success.
KEY TAKEAWAYS
- Due to the complex nature of full-arch, implant supported fixed prostheses — also known as hybrid prostheses — it is crucial for the patient and provider to engage in a long-term maintenance plan that allows adequate follow-up.
- Maintenance appointments are the pillar that supports successful outcomes in implant treatment. They also facilitate early detection of possible complications.
- Long-term maintenance plans — which should be customized to meet each patient’s specific needs — consist of in-office maintenance visits and adequate self-care.2
- Careful design of the prosthetic appliance plays a major role in long-term maintenance and proper cleansability.
- Clinicians are advised to conduct a clinical and radiographic examination of the implants, prosthetic appliances, and condition of the soft tissues at each maintenance appointment.
- This examination will help detect peri-implant mucositis or early signs of peri-implantitis, and provide an opportunity for prompt treatment — thus supporting long-term implant success.8
REFERENCES
- Curiel Aguilera F. Implant treatment planning for hybrid prostheses. Decisions in Dentistry. 2020;6(6):36–39.
- Bidra AS, Daubert DM, Garcia LT, et al. Clinical practice guidelines for recall and maintenance of patients with tooth-borne and implant-borne dental restorations. J Prosthodont. 2016;25(Suppl 1):S32–S40.
- Ioannidis A, Thurnheer T, Hofer D, et al. Mechanical and hydrodynamic homecare devices to clean rough implant surfaces — an in vitro polyspecies biofilm study. Clin Oral Implants Res. 2015;26:523–528.
- Bidra AS, Daubert DM, Garcia LT, et al. A systematic review of recall regimen and maintenance regimen of patients with dental restorations. Part 2: Implant-borne restorations. J Prosthodont. 2016;25(Suppl 1):S16–S31.
- Kanao M, Nakamoto T, Kajiwara N, Kondo Y, Masaki C, Hosokawa R. Comparison of plaque accumulation and soft-tissue blood flow with the use of full-arch implant-supported fixed prostheses with mucosal surfaces of different materials: A randomized clinical study. Clin Oral Implants Res. 2013;24:1137–1143.
- Bremer F, Grade S, Kohorst P, Stiesch M. In vivo biofilm formation on different dental ceramics. Quintessence Int. 2011;42:565–574.
- Moráguez OD, Belser UC. The use of polytetrafluoroethylene tape for the management of screw access channels in implant-supported prostheses. J Prosthet Dent. 2010;103:189–191.
- Renvert S, Persson GR, Pirih FQ, Camargo PM. Peri-implant health, peri-implant mucositis, and peri-implantitis: Case definitions and diagnostic considerations. J Periodontol. 2018;89(Suppl 1):S304–S312.
- Drago C, Gurney L. Maintenance of implant hybrid prostheses: Clinical and laboratory procedures. J Prosthodont. 2013;22:28–35.
- Goodacre CJ, Kan JY, Rungcharassaeng K. Clinical complications of osseointegrated implants. J Prosthet Dent. 1999;81:537–552.
- Cercadillo-Ibarguren I, Sanchez-Torres A, Figueiredo R, Valmaseda-Castellon E. Early complications of immediate loading in edentulous full-arch restorations: A retrospective analysis of 88 cases. Int J Oral Maxillofac Implants. 2017;32:1116–1122.
- Papaspyridakos P, Chen CJ, Chuang SK, Weber HP, Gallucci GO. A systematic review of biologic and technical complications with fixed implant rehabilitations for edentulous patients. Int J Oral Maxillofac Implants. 2012;27:102–110.
- Ventura J, Jimenez-Castellanos E, Romero J, Enrile F. Tooth fractures in fixed full-arch implant-supported acrylic resin prostheses: A retrospective clinical study. Int J Prosthodont. 2016;29:161–165.
- Zarb GA, Schmitt A. The longitudinal clinical effectiveness of osseointegrated dental implants: the Toronto study. Part III: Problems and complications encountered. J Prosthet Dent. 1990;64:185–194.
- Purcell BA, McGlumphy EA, Holloway JA, Beck FM. Prosthetic complications in mandibular metal-resin implant-fixed complete dental prostheses: a 5- to 9-year analysis. Int J Oral Maxillofac Implants. 2008;23:847–857.
- Priest G, Smith J, Wilson MG. Implant survival and prosthetic complications of mandibular metal-acrylic resin implant complete fixed dental prostheses. J Prosthet Dent. 2014;111:466–475.
- Drago C. Ratios of cantilever lengths and anterior-posterior spreads of definitive hybrid full-arch, screw-retained prostheses: Results of a clinical study. J Prosthodont. 2018;27:402–408.
- Carames J, Suinaga LT, Yu YC, Perez A, Kang M. Clinical advantages and limitations of monolithic zirconia restorations full arch implant supported reconstruction: Case series. Int J Dent. 2015;2015:392496.
- Larsson C, Vult Von Steyern P. Implant-supported full-arch zirconia-based mandibular fixed dental prostheses. Eight-year results from a clinical pilot study. Acta Odontol Scand. 2013;71:1118–1122.
- Moscovitch M. Consecutive case series of monolithic and minimally veneered zirconia restorations on teeth and implants: up to 68 months. Int J Periodontics Restorative Dent. 2015;35:315–323.
- Poggio CE, Ercoli C, Rispoli L, Maiorana C, Esposito M. Metal-free materials for fixed prosthodontic restorations. Cochrane Database Syst Rev. 2017;12:CD009606.
- Rojas Vizcaya F. Retrospective 2- to 7-year follow-up study of 20 double full-arch implant-supported monolithic zirconia fixed prostheses: Measurements and recommendations for optimal design. J Prosthodont. 2018;27:501–508.
- Gonzalez J, Triplett RG. Complications and clinical considerations of the implant-retained zirconia complete-arch prosthesis with various opposing dentitions. Int J Oral Maxillofac Implants. 2017;32:864–869.
- Limmer B, Sanders AE, Reside G, Cooper LF. Complications and patient-centered outcomes with an implant-supported monolithic zirconia fixed dental prosthesis: 1 year results. J Prosthodont. 2014;23:267–275.
- Worni A, Kolgeci L, Rentsch-Kollar A, Katsoulis J, Mericske-Stern R. Zirconia-based screw-retained prostheses supported by implants: A retrospective study on technical complications and failures. Clin Implant Dent Relat Res. 2015;17:1073–1081.
- Molly L, Nackaerts O, Vandewiele K, Manders E, Van Steenberghe D, Jacobs R. Speech adaptation after treatment of full edentulism through immediate-loaded implant protocols. Clin Oral Implants Res. 2008;19:86–90.
- Heitz-Mayfield LJ, Salvi GE. Peri-implant mucositis. J Periodontol. 2018;89(Suppl 1):S257–S266.
- Schwarz F, Derks J, Monje A, Wang HL. Peri-implantitis. J Periodontol. 2018;89(Suppl 1):S267–S290.
The author has no commercial conflicts of interest to disclose.
From Decisions in Dentistry. July 2021;7(7)8-11.
