
 PEOPLEIMAGES/ISTOCK/GETTY IMAGES PLUS
PEOPLEIMAGES/ISTOCK/GETTY IMAGES PLUS
Enhance Restorative Results With Crown Lengthening
Inadvertently placing crown margins too close to the bone and impinging on the soft tissues of the biologic width can cause complications, but clinicians can avoid such sequelae with crown lengthening.
It is common for dentists to become frustrated when recently placed crowns or bridges develop red and/or sore tissues at the margins. In a similar vein, patients may report sensitivity, or present with open crown margins for which the dentist has no clear explanation. In other cases, a tooth may look so badly broken down that a dental implant seems obvious, which may dissuade the clinician from considering treatments that not only could save the tooth, but also render it restorable. Giannobile and Lang1 state in a 2016 editorial in the Journal of Dental Research the “… erroneous belief of implants yielding a better longterm prognosis has now clearly been rejected in several studies and reviews.” They go on to say that “teeth even compromised because of periodontal disease or endodontic problems may have a longevity that surpasses by far that of the average implant,” and they offer 16 citations to support their statement. Indeed, diligent practitioners will find solutions to these everyday frustrations and challenges — toward that goal, many problematic teeth can be restored predictably with the help of crown lengthening procedures.
It is worth noting Giannobile’s and Lang’s1 premise and keeping in mind that compromised teeth do not automatically have to become implant cases. Sometimes overlooked by clinicians, crown lengthening is technically a periodontal therapy, but the goal is clearly intended as a restorative procedure.

Essentially unchanged over the past 30-plus years, crown lengthening remains as useful as ever. It has applications in all parts of the oral cavity. In posterior teeth, for example, there may not be enough tooth structure for retention, or even for a predictable impression (Figure 1 and Figure 2). The clinical situation in Figure 2 illustrates a case in which clinicians might be tempted to reach subgingivally for more retention, only to result in crown margin impingement on soft tissues. This can occur as a result of excessive gingiva (as in this case), or caries or fractures. In the esthetic zone, errors of margin placement can be even more noticeable when inflammation occurs. Learning the concepts of crown lengthening and proper margin location can help avoid inflammatory complications (Figure 3).
When restorative margins are carried subgingivally, problems can occur, such as red, sore tissues or failed impressions from margins too deep to properly impress. While crown lengthening can help create an abutment tooth with better retention, creating more available supragingival tooth structure will also allow safe placement of the restorative margin away from the soft tissue attachment. Consequently, the crown margin placement will not impinge on the soft tissues — or, even better, the margin can be located supragingivally.
GOALS OF CROWN LENGTHENING
According to the CDT codes provided by the American Dental Association, the goals for crown lengthening in a restorative application are to: Expose enough sound tooth structure to allow placement of a restorative margin onto that sound tooth structure; have adequate mechanical retention; and, at the same time, avoid disrupting or impinging on any of the gingival fiber attachments to the tooth.
In the desire to use the latest materials and techniques, such as implants or lasers, the benefits and applications of crown lengthening are often overlooked. In truth, this procedure should be part of every clinician’s armamentarium.

Placing crown margins too close to the bone and impinging on the soft tissues of the biologic width have long been known to cause inflammatory complications.2 Crown lengthening can create an environment that allows restorations to be placed safely to avoid such complications. This article will make a case for learning to manage the distance from the bone to the restorative margin interface, which is key to successful crown margin placement. Mastering this concept will help clinicians avoid many impingement scenarios.
Another benefit of crown lengthening is that once enough tooth structure is exposed, the opportunity for supragingival margins is created — and this allows clean, predictable impressions and the certainty of not impinging on the soft tissues.
Of course, each tooth with restorative/soft tissue problems is not automatically indicated for crown lengthening. Extraction leading to an implant, or use of a fixed or removable appliance should always be in the differential diagnosis. Orthodontic extrusion could also be considered, as it is sometimes a viable option — but this is a topic for another paper, and has been covered by others.3>/sup>

CONVEY THE BENEFITS
Patients referred to a specialist for crown lengthening are often unclear of what the procedure entails; in turn, this can lead to frustration among clinicians when the patient refuses treatment. Why are some referrals successful and others not? Dentists and specialists might gain greater acceptance of their referrals if patients understood the benefit of the procedure and if they could actually picture those benefits. For starters, consider using the term gum shortening instead of crown lengthening, as this might be more easily understood and visualized. In an effort to use nondental terms, a useful tool could be to describe it as the “shortening” of gum tissue, and to refer to the excess gingiva as a “turtleneck.” This could apply whether the gingival margin is apically positioned or actually removed.

While patients demand ever-greater esthetics and predictability, it remains the clinician’s responsibility to provide evidence-based, scientifically sound care. While implants and bridges have that evidence, so does crown lengthening. There are also many resources covering the biologic characteristics of human gingival tissues.4–8 The work on cadavers by Gargiulo et al5 found the dimensions of human gingiva averaged 3.06 mm from the tip of the gingiva to the crest of bone. These averages did come from a range of recession and age-related changes, and included an average of 0.69 mm for the sulcus, 0.97 mm for the epithelial attachment, and 1.07 mm for the connective tissue. As noted by Kois6 and others, the distance from the tip of the gingival margin to the tip of the bone crest is most always 3 mm,6 which very much approximates those measurements. Kois6 points out these measurements help in the crucial decision of where to place a crown margin. In addition, if a subgingival margin location is desirable for esthetic reasons, it is important to know the dimension of the soft tissue attachment to allow the margin location to remain within the sulcus and avoid soft tissue impingement.
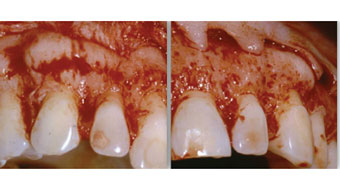
Figure 10, showing typical pattern of thick bone under these types of tissue appearances.
Despite the availability of this information, patients still have crowns placed that impinge on the gingival tissues in an apparent effort to obtain mechanical retention where there was insufficient sound clinical tooth structure, or deep caries and/or fractures. Crown lengthening is a way to avoid these challenges by creating sound tooth structure for safe placement of a restorative margin, and managing the key relationship of bone to restorative margin interface. This procedure also creates the opportunity for supragingival margins, as mentioned above. While crown lengthening can be performed after an impingement has occurred and correct the resulting sore or red tissues, offering the procedure before a crown is placed can result in better control of the esthetic result.
IMPORTANCE OF BIOLOGIC WIDTH

after a decade of no opposing teeth.
Besides impingement issues, there are instances in which dentists overlook basic biology when they perform a gingivectomy to remove excess or uneven tissues, and then place restorations into the space formerly occupied by the soft tissues. For instance, Figure 4 shows an example of excess tissue on the bicuspids. Whether the tissue is removed with a laser, blade or electrosurgery unit, this can be risky.7 It is not the choice of instrument that causes problems, it is technique that fails to respect the relationship of the gingival soft tissue to bone (namely, the biologic width). Without removing the same amount of bone as soft tissue, a violation of the biologic width will be created when restorative margins are placed where soft tissues were and the soft tissue regrows. Published reports show the gingiva will grow back to its original dimension (while this process sometimes takes up to 12 months, the tissues will regrow).9
This resulting violation of the biologic width often leads to red, sore or edematous tissues that occur as the tissue heals while reestablishing the original dimensions of the gingiva. This reestablished tissue bumps into the restoration, causing impingement. Figure 3 illustrates the resulting redness when the restorative margins are too close to the bone after a gingivectomy and the soft tissues grow back to reestablish the normal dimensions of the gingival complex, as occurred here. While some would refer to that phenomenon of regrowth as “rebound,” many reports explain the phenomenon as normal redevelopment of biologic width.9–11
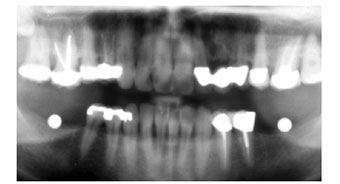
Figure 5 through Figure 9 depict how using this information allows clinicians to avoid the issue of regrowth and resulting impingement. In this case, the decision was made to eliminate the patient’s gummy smile and close the diastemas with restorations. After gingivectomy to elongate the clinical crown, the resulting provisional crown margin is very close to the bone. If the bone is not altered (Figure 8 and Figure 9), the gingiva will grow back, resulting in an impingement, as in Figure 3. Instead, the removal of bone to allow 2.5 mm of tooth-to-crown margin distance will allow for a 0.5-mm subgingival margin location and no impingement.
Thick ledges of bone, resulting in excess gingival height and small clinical crowns, leave potentially limited retention, as is often seen around second molars, and the excess tissue that results is illustrated in Figure 1 and Figure 2. This thick bone is common in maxillary and mandibular posteriors, but also occurs in the anterior, so knowing where the bone is located is key to avoiding the embarrassing red gingiva seen in Figure 3. When this thick soft tissue is observed, the question becomes, what makes it so thick? Typically, it is because the bone is thick under the soft tissue, and treating this situation requires removal of bone and not just soft tissue.
The thick tissue biotype associated with thickness in the bone is illustrated in Figure 10 and Figure 11. Predictable healing only happens when the bone is properly managed.6,9–11 When healing and maturation of the soft tissues is complete, predictable results will be achieved only by having removed enough bone and locating it 2.5 to 4.0 mm from the expected restorative margin — and not just from apically positioning the soft tissue or by doing a soft tissue gingivectomy.9,10 For subgingival margins, the distance is 2.5 to 3.0 mm, and for supragingival margins, it would be 3.5 to 4.0 mm.

improved esthetics facilitated by crown
lengthening of the molars.
Bone remains the key parameter. While some concern for the crown-to-root ratio must be acknowledged, with a periodontally sound tooth, it is unlikely that bone removal as described would result in mobility issues as so little supporting bone is removed.
Where, then, is a gingivectomy indicated? Only in cases in which there are dimensions of soft tissue exceeding the 3.0 mm of biologic width dimension beyond the bone crest. It is almost always necessary to remove bone, not just soft tissue, to create the needed tooth structure for restorative purposes.12
ADJUNCTIVE USE AND SUMMARY
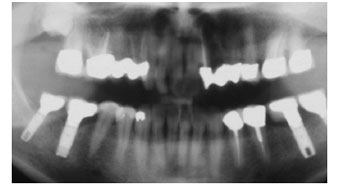
Another excellent application for crown lengthening is as an adjunct to implant procedures, as it can help provide a better long-term prognosis by establishing enough space for proper occlusal planes. Where overeruption has occurred due to teeth being missing for an extended period, it is difficult or impossible to establish proper occlusal planes (such as Curve of Spee and Curve of Wilson). By creating more exposed tooth structure, the erupted teeth can be shortened while still leaving enough structure for safe placement of margins, adequate retention and proper occlusal planes — as illustrated with the maxillary left molars in Figure 12 through Figure 15.
So, in summary, indications for crown lengthening include:
- Excessive gingival display in the anterior (often associated with thick bone)
- Short posterior teeth (usually associated with excess gingiva and thick bone)
- Uneven gingival levels
- Subgingival fractures
- Subgingival caries
- Previous crowns and finish lines too close to the soft tissue attachment and bone
- As an adjunct to implant treatment, where supraeruption has occurred
The goal of this article is to demonstrate the potential for esthetic results and predictable restorations by respecting basic tissue biology. This approach will help avoid complications, such as impinging on soft tissues and invading the biologic width. It is generally sound advice to avoid removal of soft tissue without removing a commensurate amount of matching bone, as well.
Clinicians who follow this approach will be one step closer to achieving predictable and esthetic results, both in anterior and posterior cases. These guidelines will allow operators to obtain accurate impressions and place restorations that remain safely within the sulcus — without impinging on soft tissues.
KEY TAKEAWAYS
- Compromised teeth can often be restored predictably with the help of crown lengthening, so this technique should be part of every clinician’s armamentarium.
- Placing crown margins too close to the bone and impinging on the soft tissues of the biologic width are known to cause inflammatory complications.2
- Crown lengthening can create an environment that allows restorations to be placed safely to avoid such complications.
- Learning to manage the distance from the bone to the restorative margin interface is key to successful crown margin placement, and mastering this concept will help clinicians avoid many impingement scenarios.
- While crown lengthening can be performed after an impingement has occurred and correct the resulting sore or red tissues, offering the procedure before a crown is placed can result in better control of the esthetic result.
- Another excellent application for crown lengthening is as an adjunct to implant procedures, as it can help provide a better long-term prognosis by establishing enough space for proper occlusal planes.
- In crown lengthening procedures, it is generally sound advice to avoid removal of soft tissue without removing a commensurate amount of matching bone, as well.
REFERENCES
- Giannobile WV, Lang NP. Are dental implants a panacea or should we better strive to save teeth? J Dental Res. 2016;95:5–6.
- Newcomb GM. The relationship between the location of subgingival crown margins and inflammation. J Periodontol. 1974;45:151–154.
- Durham TM, Goddard T, Morrison S. Rapid forced eruption: A case report and review of forced eruption techniques. Gen Dent. 2004;52:167–175.
- Coslet J, Ingber J, Rose L. The “biologic width” — A concept in periodontics and restorative dentistry. Alpha Omegan. 1977;70:24–28.
- Gargiulo A, Wentz F, Orban B,. Dimensions and relations of the dentogingival junction in humans. J Periodontol. 1961;32:261–267.
- Kois J. Altering gingival levels: the restorative connection, Part 1: biological variables. J Esthetic Restorative Dent. 1994;6:3–9.
- Nevins M, Mellonig J. Periodontal Therapy: Clinical Approaches and Evidence of Success. Hanover Park, Ill: Quintessence Books; 1998.
- Oh SL. Biologic width and crown lengthening: case reports and review. Gen Dent. 2010;58:e200–e205.
- Pontoriero R, Carnevale G. Surgical crown lengthening: A 12-month clinical wound healing study. J Periodontol. 2001;72:841–848.
- Deas DE, Moritz AJ, McDonnell HT, Powell CA, Mealey BL. Osseous surgery for crown lengthening: A 6-month clinical study. J Periodontol. 2004;75:1288–1294.
- Arora R, Narula SC, Sharma RK, Tewari S. Evaluation of supracrestal gingival tissue after surgical crown lengthening: a 6-month clinical study. J Periodontol. 2013;84:934–940.
- Padbury A, Eber R, Wang HL. Interactions between the gingiva and the margin of restorations. J Clin Periodontol. 2003;30:379–385.
From Decisions in Dentistry. July/August 2019;5(7):16,18,21–22.
