
 PORNPAK KHUNATORN/ISTOCK/GETTY IMAGES PLUS
PORNPAK KHUNATORN/ISTOCK/GETTY IMAGES PLUS
Dentists’ Role in Migraine Treatments With Botulinum Toxins
Treatment for migraines using botulinum toxins shows promise for successful management by dental professionals.
Ranked as the third most common disease worldwide, migraines affect 14.7% to 18.5% of the population globally.1 Classified as a neurovascular disorder and recognized as a major cause of disability,2 this condition3 affects one in seven people worldwide.4 In the United States, the prevalence of migraines may be as high as 18%, with approximately 39 million people currently affected.2 Given this prevalence, dental teams likely already provide oral care for affected individuals — and, with proper training and appropriate professional judgment, dentists can also offer migraine treatments using botulinum toxin injections.
This common disorder can be divided into two major subtypes. The first is migraine without aura, which accounts for approximately 70% of migraine attacks. The second subtype is migraine with aura, which accounts for approximately 30% of migraine events (Table 1).1 Aura is a warning sign that can have visual symptoms, such as flashing lights, fortification spectra (i.e., zigzag lines resembling forts), or blind spots in the vision.5 Migraine is a common neurological disorder with a significant economic impact. Compared to individuals without the disorder, migraines cost employers in the United States is estimated at $9.2 billion per year.2 According to a 2018 study, annual health care expenditures for an individual experiencing migraines was $8033, which, in part, can be broken down into outpatient costs ($2952), prescription drugs ($2207), and inpatient expenditures ($1784).2
General dentists screen and manage individuals who have headaches regularly stemming from many etiologies. By using a multidisciplinary approach involving the patient’s physician and medical team, dentists can play a role in treatment for migraines in the dental office. In this multidisciplinary approach, it is important for the patient to be thoroughly evaluated, with a proper diagnosis offered by a qualified and suitably trained health professional. Chronic headaches are complex and difficult to diagnose. A correct diagnosis of migraine is paramount in managing patients with chronic headaches. The diagnosis should be made by a headache neurologist and/or orofacial pain specialist. Besides specialists, treatment options might include primary care physicians, chiropractors, neurologists, physical therapists and other disciplines — including dentists with specialized training in the use of botulinum toxins.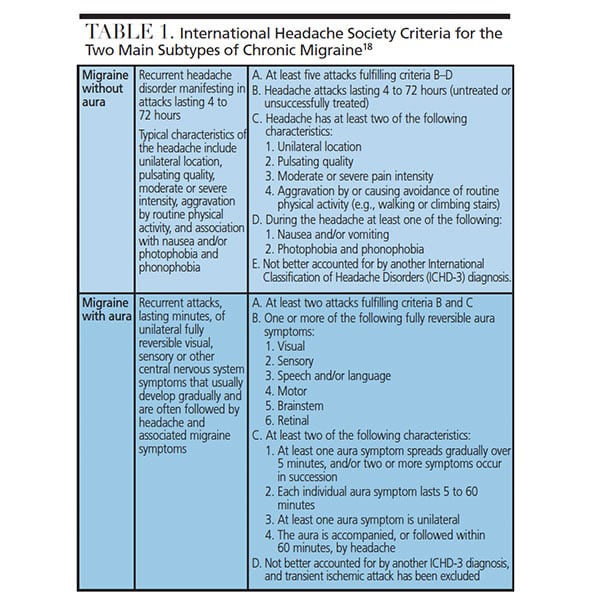
MIGRAINE HEADACHES AND PREVENTIVE THERAPIES
Migraines typically present as a severe, unilateral, throbbing headache lasting between four and 72 hours.6 Associated symptoms include nausea and emesis, accompanied with photophobia and phonophobia.7 The criteria for the classification of headaches is determined by the International Headache Society using the International Classification of Headache Disorders (ICHD-3).8 Pharmacotherapy for migraines include abortive and preventive medications. The acute therapy for migraines may include medications, such as nonsteroidal anti-inflammatory drugs, and migraine-specific agents, such as triptans.9 The success of acute therapies is guarded, as acute medication overuse can itself cause more frequent headaches (called rebound or medical overuse headache).7,9 If migraines are identified early, they can be aborted with pharmacological treatment using either nonspecific or migraine-specific medications.10 Nonspecific medications include aspirin, ibuprofen and naproxen, while migraine-specific medications include ergotamine, caffeine plus ergotamine, dihydroergotamine, sumatriptan and zolmitriptan.10
Preventive therapy can include adrenergic receptor antagonists, such as propranolol and timolol; calcium-channel antagonists, such as verapamil; tricyclic antidepressants, such as amitriptyline; and anticonvulsants, such as divalproex sodium, gabapentin and topiramate.9,11,12
A preventive therapy that has gained attention in chronic migraine treatment is use of botulinum toxin type A (BoNT-A).13 While this agent has been used for more than 25 years to treat various neurological disorders,14 the mechanism by which botulinum toxin prevents migraine attacks is not fully understood. The mechanism of action of BoNT-A inhibits the release of acetylcholine. Botulism toxins inhibit the release at the neuromuscular junction, which depolarizes the motor end plate of the muscle, which, in turn, causes muscle contraction.15 Botulinum neurotoxins cause flaccid paralysis that interferes with vesicle fusion and neurotransmitter release in neural cells.16 Produced by the anaerobic bacterium, Clostridium botulinum, BoNT-A is a natural protein.17 Botulinum toxins exert their effects through uptake by cholinergic neurons, resulting in temporary chemodenervation and a decrease in neuromuscular transmission.12
While there is no muscle component involved in migraines,18 in vitro evidence suggests BoNT-A may inhibit the release of neuropeptides involved in pain perception and inflammation.12 Botulinum toxin has become a viable and effective option in treatment for migraines.16 This treatment option also relieves the pain when there is excessive muscle contraction.18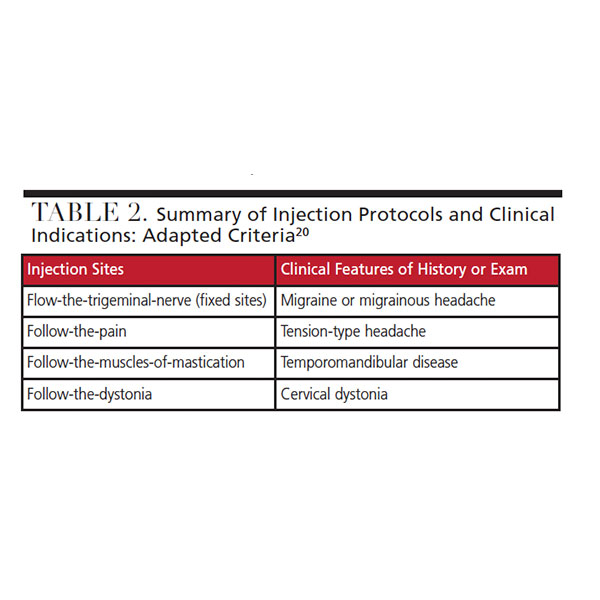
CASE REPORT
Because dentists are specially trained in the orofacial region, practitioners with the proper training and sound clinical judgment can use botulinum toxin injections to treat patients diagnosed with migraines. This case report involves a patient with a diagnosis of chronic migraines for more than 10 years who had received treatment from numerous doctors from a myriad of specialties. It is important to note this case treated a patient with a preventive therapy that is used for chronic migraines and not acute migraines.19
A 49-year-old female presented to our private dental practice. The patient had been experiencing migraine headaches for years, and in her medical history she reported seeing multiple doctors for the condition, including neurologists, pain management specialists, chiropractors, psychiatrists and several dental practitioners. Treatments included migraine prescriptions, monthly chiropractic adjustments, treatment for depression caused by the migraines, and dentist-prescribed oral appliances. The medications included 800 mg Motrin, Ergostat 2 mg, Cafergot 100 mg caffeine/1 mg ergotamine, and Imitrex 12 mg. The patient noted some, but not significant, improvement with Imitrex. The patient stated she had little success with previous treatments from various clinicians over the past decade.
The patient was diagnosed with chronic migraine headaches by a neurologist using the International Headache Society ICHD-3 diagnostic criteria (Table 1).8 She reported six attacks per month, averaging at least one to two per week. The patient said the migraines typically lasted seven to 10 hours, producing severe pain and symptoms that might include nausea, vomiting, osmophobia and photophobia.
In her history, she reported trauma to the head/neck and jaw region as a child as a result of an automobile accident. The patient stated no surgery was needed, but felt her jaw was “never right” after the accident. This also coincided with the start of sporadic headaches that increased in frequency and severity over time. She stated the headaches and migraines got worse around age 35, and progressively worsened. The patient reported the area with the highest concentration of pain was in the bilateral forehead area, and that she experienced aura symptoms.
At the initial visit, the patient was asked to use the analog pain scale to rate pain during a migraine attack. She reported the areas by pointing to the affected muscles on her face during the initial clinical evaluation. The most painful areas were in the lower medial forehead or glabella area. The patient stated on an analog pain scale of 1 to 10 her pain was “1000” in the glabellar region during a migraine. She also noted less significant pain in the frontalis muscles, including the area over the anterior temporal region; the patient reported a score of 5 on the pain scale in this area when migraines occur.

a patient with migraine disorder.
EXAMINATION AND CONSENT
On physical examination, the patient’s oral health was unremarkable, with restorations in her posterior teeth. She was asked to report on pain using a scale of 0 to 10 (0 being no pain and 10 being the worst possible pain) when palpating the muscles. The muscles of mastication and muscles of the neck and back were unremarkable when palpated, with the patient reporting 0 on the scale. She reported 5 in the procerus and bilateral corrugator muscles, and 3 on the frontalis muscle on palpation (Figure 1). From the information gathered during the medical history review and clinical examination, a migraine treatment plan was created and presented using BoNT-A as preventive therapy for managing her headaches. The plan was reviewed with the patient, who agreed to treatment and provided informed consent. The patient was told of the injection sites for treatment and that a “fixed sites” approach from Blumenfeld’s protocol (Table 2) would be used.20 This protocol was chosen because of Blumenfeld et al’s findings from 271 patients using botulism to treat chronic migraines.20,21

The patient indicated the most severe pain with her migraines was in the procerus and frontalis muscles. The dosage protocol was based on the recommended dosages (Table 3).20 The first injection site of BoNT-A was the procerus muscle at 5.0 U (Figure 2). The next injection site was the corrugator muscles, and 2.5 U was injected for each muscle, with two injection sites (one per side). The final injection site was the frontalis muscle, and 2.5 U was injected into 12 sites (six per side).
The patient was given postoperative instructions that included remaining upright for at least four hours, not wearing a headband, refraining from aerobic exercise, and not massaging the areas of injection for 24 hours. She was asked to return in four weeks for follow-up. The patient was also asked to maintain a journal of any side effects and incidences of migraine attacks. The patient was called that night and reported no side effects and that she was “doing well.” At the follow-up appointment, the patient noted no side effects from the BoNT-A treatment, and while she still experienced migraines, they were not as severe as previously, and they occurred four times instead of the previously reported six events per month.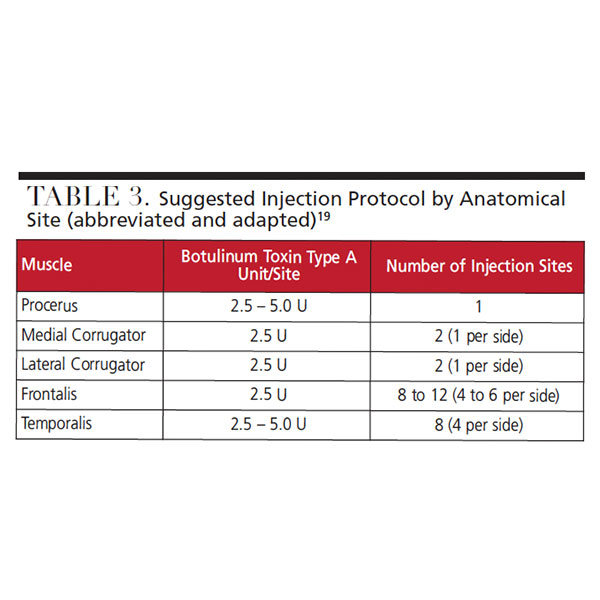
ONGOING FOLLOW-UP
The patient was asked to come in monthly to record any changes. In the ensuing visits, she noted improvements, but reported still having migraines. She said the location was the same, and while the symptoms of nausea, vomiting and photophobia were less severe, they were still present. At the six-month follow-up, the patient stated that since the initiation of BoNT-A migraine treatment, she averaged about four to five migraines a month, and two were just as severe as previously. The rest showed slight improvement, with a pain scale rating of 8 instead of 10, as reported prior to treatment.
In summary, the patient expressed satisfaction, and although the changes were not as significant as hoped for, she was appreciative of the progress made during the past six months. She indicated she would continue with botulinum toxin as treatment for migraines. The patient stated she feels better and her quality of life has improved, so she will continue to manage her headaches in this fashion.
CONCLUSION
As noted, prior to being seen in our clinic, the patient had been treated by experts from several disciplines in medicine for more than a decade. This care had resulted in minimal to no improvement of symptoms from chronic migraines, so botulinum toxin was presented as a viable treatment option. The excellent tolerability of BoNT-A makes it an effective treatment adjunct for patients who have had limited success with other treatment modalities, such as oral prophylactics.8 When indicated, botulinum toxin is a viable preventive therapy for patients experiencing migraines.22,23
As part of a multidisciplinary care team — and in consultation with the appropriate specialists and medical professionals — dentists with special training to administer botulinum toxins can use this approach as part of a preventive therapy for managing chronic migraines. Again, such treatment should not be initiated without a proper diagnosis from a headache neurologist and/or orofacial pain specialist. In addition, the dentist should thoroughly review the medical and social history at every appointment to ensure this course of therapy is both appropriate and effective in migraine treatment.
KEY TAKEAWAYS
- Ranked as the third most common disease worldwide, migraines affect 14.7% to 18.5% of the population globally.1
- By using a multidisciplinary approach with the patient’s physician and medical team, dentists with specialized training can play a role in treatment for migraines in the dental office with botulinum toxin injections.
- In this multidisciplinary approach, it is important for the patient to be thoroughly evaluated, with a proper diagnosis offered by a suitably trained health professional. A headache neurologist and/or orofacial pain specialist should make the diagnosis.
- If migraines are identified early, they can be aborted with pharmalogical treatment using either nonspecific or migraine-specific medications.10
- Preventive therapy can include adrenergic receptor antagonists, calcium-channel antagonists, tricyclic antidepressants and anticonvulsants.9,11,12
- A preventive therapy that has gained attention in chronic migraine treatment is use of botulinum toxin type A (BoNT-A).13 In vitro evidence suggests BoNT-A may inhibit the release of neuropeptides involved in pain perception and inflammation.12
- It is important to note the case report presented here treated a patient with a preventive therapy that is used for chronic migraines and not acute migraines.19
- When indicated, BoNT-A is a viable preventive therapy for patients experiencing migraines.22,23
REFERENCES
- Rhee TG, Harris IM. Reasons for and perceived benefits of utilizing complementary and alternative medicine in U.S. adults with migraines/severe headaches. Complement Ther Clin Prac. 2018;30:44–49.
- Agosti R. Migraine burden of disease: from the patient’s experience to a socio-economic view. Headache. 2018;58(Suppl 1):17–32.
- Ramage-Morin PL, Gilmour H. Prevalence of migraine in the Canadian household population. Health Reports. 2014;25:10–16.
- Gormley P, Anttila V, Winsvold BS, et al. Meta-analysis of 375,000 individuals identifies 38 susceptibility loci for migraine. Nat Genet. 2016;48:858–866.
- National Headache Foundation. Aura. Available at: headaches.org/2007/10/25/aura/. Accessed July 22, 2019.
- Feoktistov A. Headache classification and medically resistant headaches. In: Feoktistov A (ed). Interventional Management of Head and Facial Pain. New York: Springer; 2014:3–7.
- Silberstein SD, Welch KM. Painkiller headache. Neurology. 2002;59:972–974.
- Headache Classification Committee of the International Headache Society. The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38:1–211.
- Silberstein SD. Practice parameter: evidence-based guidelines for migraine headache (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2000;55:754–762.
- Aukerman G, Knutson D, Miser WF, Department of Family Medicine, Ohio State University College of Medicine and Public Health. Management of the acute migraine headache. Am Fam Physician. 2002;66:2123–2131.
- Ferrari MD. Migraine. Lancet. 1998;35:1043–1051.
- Goadsby PJ, Lipton RB, Ferrari MD. Migraine — Current understanding and treatment. N Engl J Med. 2002;346:257–270.
- Blumenfeld A, Binder WJ, Blitzer A, Katz H. The emerging role of botulinum toxin type A in headache prevention. Operat Tech Otolaryngol. 2004;15:90–96.
- Raghavan R, Shajahan PA, Ritha B. Botox and its role in prosthodontics. Available at: guident.net/articles/prosthodontics/botox-and-its-role-in-prosthodontics.html. Accessed July 22, 2019.
- Krymchantowski AV, Bigal ME, Moreira PF. New and emerging prophylactic agents for migraine. CNS Drugs. 2002;16:611–634.
- Binder WJ, Brin MF, Blitzer A. Botulinum toxin type A (BOTX) for treatment of migraine headaches: An open-label study. Dis Mon. 2002;48:323–353.
- Rao LB, Sangur R, Pradeep S. Application of botulinum toxin type A: an arsenal in dentistry. Indian J Dent Res. 2011;22:440–445.
- Chen S. Clinical uses of botulinum neurotoxins: current indications, limitations and future developments. Toxins (Basel). 2012;4:913–939.
- Capehart KL. Treating migraines with Botox: a case report. J Neurol Stroke. 2014;1:1–3.
- Blumenfeld AM, Binder W, Silberstein SD, Blitzer A. Procedures for administering botulinum toxin type A for migraine and tension-type headaches. Headache. 2003;43:884–891.
- Blumenfeld A, Evans RW. Onabotulinum toxin A for chronic migraine. Headache.2017;57:E10–E16.
- Capehart KL, Mollica AG, Young NB. Migraines and Botox. J Dent Assist. 2018;87:10–12.
- Buse DC, Loder EW, Gorman JA, et al. Sex differences in the prevalence, symptoms, and associated features of migraine, probably migraine and other severe headache: results of the American Migraine Prevalence and Prevention (AMPP) Study. Headache. 2013; 53:1278–1299.
The authors have no commercial conflicts of interest to disclose.
From Decisions in Dentistry. September 2019;5(8):44—47.
