
7 Habits of Highly Effective Implant Clinicians
Understanding the nuances of implant/abutment screw joints will help providers minimize biomechanical complications.
The majority of dental implants are two-part systems in which the endosseous and transmucosal portions combine to present a joint surface to the tissues. This is known as the implant-abutment (IA) joint.1 By far, the most commonly used connection between the implant body and abutment is the screw joint. This joint may also be used as a direct means of connecting the final prosthesis with an integral abutment to the implant.
The IA screw joint is considered a nonpermanent joint that allows retrievability. The advantages include:
- The ability to exchange components (e.g., healing abutments, impression copings or definitive abutments)
- This joint enables various abutment materials to be connected to the implant via a screw, such as titanium, zirconia or polyetheretherketone
- Screw joints do not depend on cementation agents that could introduce contaminants into the peri-implant tissues
- This connection also allows control of the joint clamping forces
Although dentists may be familiar with the screw joint in general, many fail to appreciate how errors make it susceptible to failure.2 Implant abutment screw loosening is the most common prosthetic complication, with a reported incidence of 7% to 12% over six years for single implant crowns.3–7 With the goal of improving outcomes, this is the first article in a series that explores seven successful habits to reduce the likelihood of the IA joint failing or screws loosening.
While failure to maintain the IA joint can lead to biological and mechanical issues, these can often be resolved if they are dealt with expediently. In other cases, however, screw joint failure results in bone loss, peri-implantitis or mechanical damage, such as screw breakage, material wear, or implant fracture. Fortunately, most complications can be avoided with a better understanding of how screw joints work, through correct use of calibrated torque wrenches, and by recognizing that occlusion is dynamic and requires continual assessment.
HABIT 1: UNDERSTAND THE JOINT
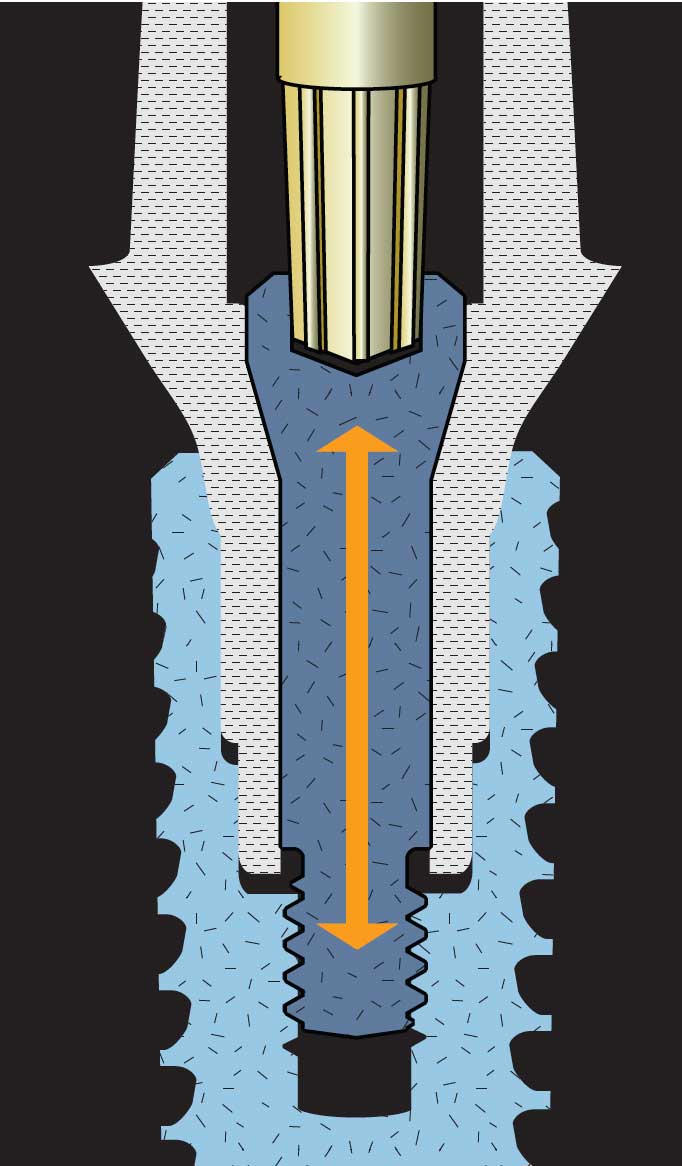
The screw joint has been utilized by engineers for hundreds of years and is effective when used correctly. When torque (a rotational force) is applied to the implant screw, it moves into or out of a reciprocating thread within the implant body. This requires energy to overcome the friction of the thread surfaces moving against each other. Preload is the name given to the tension or stretch that develops within the screw; it acts like an elastic as it pulls the joint together, producing a clamping force (Figure 1). Implant manufacturers prescribe the torque needed to produce the optimum clamping force, and these values should be strictly heeded. It is worth noting that most of the torque that tightens the screw is absorbed due to friction, and that only 10% of the input torque converts to preload. Too little torque leads to premature loosening, while too much results in deformation of the screw, reducing its ability to stretch and promoting early failure. Too much torque is especially problematic, as the weakness in a screw system occurs when the screw joint is loaded with lateral forces — such as the cyclic action of chewing, or the effects of parafunctional or cantilever forces.
HABIT 2: USE TOOLS CORRECTLY
In order to achieve the specified torque, clinicians must rely on specialized tools, such as torque wrenches. These must be both accurate and precise; otherwise, too little or too much torque will be applied — which increases the risk of screw failure.
Unfortunately, most dentists fail to routinely calibrate or check the torque wrench to ensure it meets the calibration limits required by all industries that use torque wrenches.8 The International Standards Organization recommends this be done at an absolute minimum yearly, unless the device is subject to contamination or extreme heat.9 Both of these conditions exist in dentistry — moisture and saliva cannot be avoided, and the heat of autoclaving is considered extreme. Thus, the author recommends the friction style (also known as toggle or break-neck) torque wrench be checked each time it is used. Limitations of the spring- or cantilever beam-type wrenches also exist, which will be discussed in future articles covering additional habits practiced by successful implantologists.
References
- International Congress of Oral Implantologists. Glossary of Implant Dentistry. Available at: https://www.icoi.org/wp-content/uploads/2018/08/Glossary-of-Implant-Dentistry-3.pdf. Accessed January 4, 2022.
- Huang Y, Wang J. Mechanism of and factors associated with the loosening of the implant abutment screw: A review. J Esthet Restor Dent. 2019;31:338–345.
- Katsavochristou A, Koumoulis D. Incidence of abutment screw failure of single or splinted implant prostheses: A review and update on current clinical status. J Oral Rehabil. 2019;46:776–786.
- Goodacre BJ, Goodacre SE, Goodacre CJ. Prosthetic complications with implant prostheses (2001–2017). Eur J Oral Implantol. 2018;11(Suppl 1):S27–S36.
- Jung RE, Pjetursson BE, Glauser R, et al. A systematic review of the 5-year survival and complication rates of implant-supported single crowns. Clin Oral Implants Res. 2008;19:119–130.
- Kourtis S, Damanaki M, Kaitatzidou S, Kaitatzidou A, Roussou V. Loosening of the fixing screw in single implant crowns: predisposing factors, prevention and treatment options. J Esthet Restor Dent. 2017;29:233–246.
- Bickford JH. An Introduction to the Design and Behavior of Bolted Joints. Boca Raton, Fla: CRC Press; 1995.
- Wadhwani CP, Rosen PS, Yang G, et al. Survey of dental clinicians for attitude and use of torque-limiting devices. Int J Oral Maxillofac Implants. 2021;36:538–545.
- International Standards Organization. ISO 6789-2:2017. Available at: https://www.iso.org/standard/62550.html. Accessed January 4, 2022.
From Decisions in Dentistry. February 2022;8(2):24.
