

Shaping, Disinfecting and Obturating Root Canals
An examination of contemporary methods for instrumentation and cleaning during endodontic procedures, and the importance of an effective coronal seal in ensuring successful outcomes.
An examination of contemporary methods for instrumentation and cleaning during endodontic procedures, and the importance of an effective coronal seal in ensuring successful outcomes.
SECOND IN A TWO-PART SERIES
Appearing in the June 2016 issue, Part 1 discussed contemporary standards in endodontics, and best practices for providing effective care. It is available at decisionsindentistry.com.
With increasing numbers of general dentists performing root canal therapy, it is important for these clinicians to recognize they are held to the same standards as endodontic specialists. With this in mind, dental professionals should exercise prudence when determining which cases to treat — and which to refer. Available through the American Association of Endodontists (AAE), the Endodontic Case Difficulty Assessment Form and Guidelines provide a roadmap for when general practitioners should treat or refer to an endodontist.1 Designed to assist clinicians with this decision, the form is also useful for treatment planning and record keeping.
Appearing in the June 2016 issue, the first installment of this series details the standards of contemporary endodontic practice, and covers topics such as case assessment, treatment records, and the need for proper magnification and imaging. This concluding installment will examine the instrumentation, cleaning/disinfection and obturation phases of root canal therapy — as well as the critical role that a proper coronal seal plays in ensuring treatment success. In addition, it will discuss common mishaps — and appropriate responses — during endodontic therapy.
INSTRUMENTATION

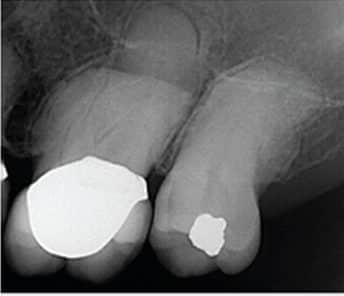
Root canals are often depicted as smooth, hollow tubes that are more or less tapered in shape. These misleading images do not reflect the intricate anatomical structure and complexity of root canal systems. They are regularly asymmetrical or oval in cross section; in addition, they branch, dilacerate and divide, and the canal walls show concavities and convexities.2 Complex root canal anatomy should be considered one of the most significant challenges in debriding the canal system and creating root canal shapes that will support successful obturation outcomes — while still leaving sufficient root strength (Figure 1).
Ultrasonic systems, in conjunction with magnification, improve vision by eliminating the bulky head of the conventional handpiece, which frequently obstructs vision when instrumenting difficult-to-access canals. The working ends of specific ultrasonic instruments are five to 10 times smaller than the smallest round burs, and their abrasive coatings allow them to precisely excavate dentin when exploring for mineralized canals or removing mineralized obstructions.3 By comparison, a rotating bur in a dental handpiece is often difficult to see, because even a small handpiece head may block the line of sight.
After biomechanical instrumentation, the completed root canal shapes need to withstand the internal compressive forces of obturation, provide sufficient resistance form to contain softened and compressible filling materials, and retain enough strength for mastication and parafunction.
Transportation, ledging, apical perforation and loss of the original canal position are all well-recognized shaping errors that often lead to loss of working length and damage to the apical terminus, followed by a weakening of the root structure at its most fragile levels.4
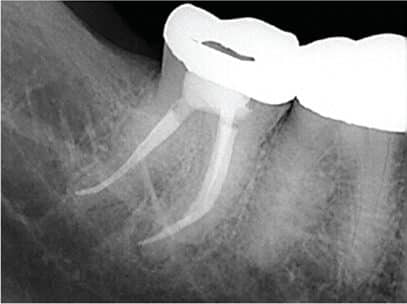
There is now a large body of conclusive research quantifying the use of nickel-titanium (NiTi) rotary and hand instruments. Compared to traditional stainless steel instruments, the literature indicates that use of these super-elastic metal alloy instruments minimizes issues with straightening, and facilitates better centered preparations across a wide range of anatomical variability5 (Figures 2A through 2C). These studies have focused on the shape geometry produced by NiTi instruments alone, or in com bination with stainless steel instruments — including taper, flow and maintenance of the original canal position. Collectively, these studies suggest that NiTi technology, in combination with the conservative use of stainless steel instruments, provides shapes that maintain the original canal positions with greater conservation of dentin, while also offering safer radicular preparations.5

Additionally, the use of electronic measuring devices, such as electronic apex locators, is standard technology for accuracy when shaping and cleaning deep within the root canal system. Combined with diagnostic-quality radiographs, an apex locator helps provide accurate length readings and corroboration with radiographs. Both are indispensable to rendering safe and accurate preparations.

DISINFECTING CANALS
In order to address the microbiologic etiology of endodontic disease, disinfection is — and will always remain — a key part of the treatment strategy. Current cleaning and shaping methods appear unlikely, however, to predictably remove all bioburden from the root canal system. Two of the most common reasons for persistent infection are resistant organism populations protected in a biofilm, and canal complexities that harbor infected necrotic tissues — even after thorough instrumentation. This speaks to the fact that it is difficult to reach the most complex irregularities within the canal, and why thorough and copious irrigation with effective an – timicrobials remains a critical component of therapy. The use of antimicrobial irrigants during root canal treatment — whether they are delivered by passive irrigation, positive-pressure irrigation (via a side-vented needle), sonic or ultrasonic agitation, or negative pressure evacuation — meets the prevailing standard of practice for endodontic irrigation.6 The key to adequate disinfection is the volume of solution that is used throughout the shaping process. Canal cleanliness is directly related to our ability to maintain a constant volume of fresh solution in the canals, both as shaping takes place, and as debris is evacuated. Sonic or ultrasonic agitation of the irrigant further enhances the ability to remove the bioburden of the infected canal.
CONSIDERATIONS FOR OBTURATION
Gutta-Percha:The most common endodontic core material is gutta-percha. It has more than 100 years of history in dental treatment. In its clinical formulations, gutta-percha comprises approximately 20% of total volume, with the remainder mostly zinc oxide and proprietary additives. Compared to other components used in endodontic obturation, gutta-percha has a low degree of toxicity, and has withstood the test of time in clinical use.
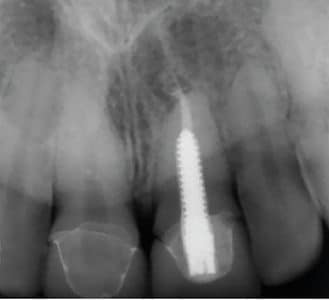
Obturation of root canal systems with this “medical-grade” rubber is possible with a host of potential applications. From lateral condensation with spreaders to warm, vertical technologies using heat-generating devices, and from custom, single-cone techniques that fit a rotary file preparation to gutta-percha carriers heated in an oven, all meet the standard of practice when utilized appropriately7(Figures 3A and 3B, page 28).
Silver Points: Based on scholarly evidence, using silver points in lieu of gutta percha or other conventional endodontic filling materials is not the current standard of practice.8 This is because silver points corrode in time, and a well-fitting apical seal is difficult to achieve during initial placement — and is eventually lost through corrosion. The 2013 AAE Position Statement on the Use of Silver Points does not recommend the prophylactic retreatment of silver point obturation unless there is clear evidence of endodontic pathosis, or if the silver points complicate proper restoration of the tooth.
N2 (Sargenti Paste): Research has found that permanent neurologic injury can occur with overfilling using paraformaldehyde sealant (N2), as N2 is cytotoxically unsafe and should be avoided.9Accordingly, the use of such materials is below the standard of practice for endodontic treatment.
ROLE OF THE CORONAL SEAL
Even the most meticulous endodontic treatment will become reinfected if microorganisms from the oral cavity contaminate the root canal system. Long-term seal of the canal system is determined apically by the solid core and sealer, and coronally by the final restoration. Coronal leakage has been shown to be responsible for a constant source of microorganisms and nutrients that can initiate and maintain periradicular inflammation.

does not meet the standards of
contemporary endodontic practice.
Because varying canal shapes (from round to oval) preclude a perfect, impenetrable seal, root-filled teeth should be permanently re – stored without undue delay to prevent contamination of the previously obturated canal system.10 Leaking coronal restorations and their relation to root canal failure rates have been corroborated by investigations into the time needed for salivary microorganisms to contaminate the entire length of sealed root canals exposed to the oral environment. Observed results showed that all root canals were recontaminated, on average, in less than 30 days.11 Until a permanent restoration is cemented, bonded barriers (e.g., orifice plugs) covering the canal openings may be used to control any leakage following compaction.

distal root perforation led to a devastating
overfill in the mandibular canal.
A leaking temporary or defective restoration will lead to contamination of an obturated root canal system over time, so the importance of keeping the temporary phase as short as possible, and restoring the root-filled tooth, cannot be overemphasized.12 The endodontic goal is to prevent bacterial contamination of the periradicular tissues by providing adequately cleaned, shaped and filled canal systems that are competently restored.13
MISHAPS
Separated Instruments: Clinical risk reduction for separated files can be accomplished if all handheld stainless steel and rotary NiTi shaping files are discarded after single-patient use. Separation incidents increase sharply when hand or rotary shaping files are reused. Chairtime and staff efficiency — along with improved patient safety — dictate the use of single-visit files.
Today, separated instruments can often be removed thanks to technological advances in vision, ultrasonic instrumentation and microtube delivery methods.14 Specifically, the increasing integration of the dental operating microscope into clinical practice allows clinicians to visualize the coronal portion of most fractured instruments. Once a separated instrument is located visually, a strategy for removal is often possible.


Perforations: If perforation occurs, early diagnosis and treatment are crucial, as belated intervention substantially increases the risk of chronic infection and failure. If a perforation is relatively small and diagnosed at the time of the occurrence, immediate sealing of the perforation with intracanal sealants, such as mineral trioxide aggregate or bioceramic repair materials, has a high success rate if placed properly under magnification and good illumination. A delayed diagnosis and treatment (beyond 24 to 72 hours), however, will result in bacterial contamination of the area surrounding the perforation. Delayed repair can lead to periodontal or endodontic lesions, as well as lateral periodontal breakdown — making healing and a favorable prognosis less likely.
Overfilling Into Neurovascular Anatomy: A clinician initiating root canal treatment on a mandibular posterior tooth should always be mindful of the vital neurovascular bundle containing the inferior alveolar nerve or mental nerve, which commonly approximates the ends of these roots. In the interest of patient safety, it is vitally important to procure a diagnosticquality image that accurately demonstrates the crestal borders of the inferior alveolar nerve canal (IANC). The use of three-dimensional cone beam computed tomography aids in assessing the IANC location for planning apical surgery or obturation in dangerous proximity of neurovascular anatomy. If endodontic treatment is performed without adequate diagnostic radiographs, the patient is at risk if there is anatomic variation, or if vital neural bundles lie in close proximity to these roots.15
Overfilling and/or overinstrumentation of the root ends can cause traumatic and/or chemical injury to the vital neural bundle, resulting in potentially permanent alteration, or total loss of sensation from paresthesia (partial numbness), anesthesia and/or dysesthesia (burning pain). The eugenol or resin components of root canal sealers are known to be cytotoxic in their 28 freshly mixed state. Consequently, endodontic overfill of the root apex into the IANC is capable of producing not only mechanical and compression damage, but also chemical injury16 (Figure 4, page 28). Accordingly, if the patient demonstrates neuropathic symptoms in the first 24 hours, or in days subsequent to a sealer entering the IANC, an expedient microsurgery referral to remove the injurious materials from the nerve space is warranted as a neurologic emergency.17 Referral to a microsurgeon, whether an oral surgeon or endodontist, is time sensitive.
Ultrasonic Burns: Ultrasonic instrumentation has become an indispensable technology for removal of metallic obstructions within the root canal space, such as post removal for retreatment and retrieval of separated instruments. Vibratory energy will loosen the cementation materials around posts, but the clinician must take precaution in such circumstances, as large amounts of heat are generated deep within the root canal space. The clinician can avoid overheating a post and surrounding tissues by proceeding slowly with a concentrated water coolant, periodically stopping to allow cool down, and checking the post temperature periodically, so as to be reasonably certain overheating is not occurring.18 Figures 5A through 5C illustrate a patient burn injury from an overheated tooth during a post removal attempt, resulting in tissue necrosis, bone loss and a poor prognosis for long-term retention.

Bleach Injuries: Sodium hypochlorite remains the endodontist’s first choice as a disinfection solution. Prevention of sodium hypochlorite extrusion is accomplished by using syringes with side-venting needles, and by constantly moving the syringe in small, vertical amplitudes to prevent hydrostatic buildup. Sodium hypochlorite can be extruded into the periapical tissues during treatment if excessive pressure is placed on the irrigating syringe, resulting in an expression of sodium hypochlorite beyond the apex. Immediate, extreme pain and swelling results from the solution diffusing into the surrounding bone and soft tissues, causing tissue necrosis from the irrigant’s high alkalinity.
Palliative treatment, such as cold compresses, accompanied by reassurance that most symptoms will dissipate, is usually adequate. Occasionally, antibiotics are prescribed. Some patients experience several days of increasing edema and ecchymosis, accompanied by tissue necrosis, paresthesia and secondary infection. Although most patients recover within one to two weeks, hospitalization, long-term paresthesia, chronic pain and surgical intervention have been reported19,20 (Figure 6).
KEY TAKEAWAYS
- General dentists who perform root canal procedures should recognize they are held to the same standards as endodontists, and should carefully consider which cases to treat or refer.
- Ultrasonic technology eliminates the bulky head of the conventional dental handpiece, which can obstruct vision when accessing canals.
- An apex locator helps provide accurate length readings and corroboration with radiographs; both are indispensable to rendering safe and accurate preparations.
- Canal cleanliness is directly related to the ability to maintain a constant volume of fresh irrigant in the canals — both as shaping takes place, and as debris is evacuated.
- Long-term seal of the root canal system is determined apically by the solid core and sealer, and coronally by the final restoration.
- Root-filled teeth should be permanently restored without undue delay to prevent leakage contamination of the previously obturated canal system.10
FINAL CONSIDERATIONS
Given that the number of patients needing root canal therapy far exceeds the capacity of endodontists to treat each of these cases, the trend of general dentists performing root canal procedures is likely to continue. From a clinical standpoint, the key considerations are that providers carefully consider treating or referring these cases, and that they take steps to ensure that any treatment rendered meets contemporary standards of endodontic practice.
As with all forms of treatment, earning patient trust and providing predictable outcomes can only come from a practitioner operating within the bounds of his or her armamentarium and level of training and expertise
A version of this article originally appeared in ENDODONTICS: Colleagues for Excellence, Fall 2014. Reused with permission from the American Association of Endodontists, ©2014. The AAE clinical newsletter is available at aae.org/colleagues.
REFERENCES
- American Association of Endodontists. Endodontic Case Difficultly Assessment Form and Guidelines. Available at: http://www.aae.org/caseassessment. Accessed May 2, 2016.
- Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics. 2005;10:3–29.
- Park E. Ultrasonics in endodontics. Endod Topics. 2013;29:125–159.
- Bürklein S, Schäfer E. Critical evaluation of root canal transportation by instrumentation. Endod Topics. 2013;29:110–124.
- Hülsmann M, Peters OA, Dummer PMH. Mechanical preparation of root canals: shaping goals, techniques and means. Endod Topics. 2005;10:30–76.
- Basrani B, Haapasalo M. Update on endodontic irrigating solutions. Endod Topics. 2012;27:74–102.
- Whitworth, J. Methods of filling root canals: principles and practices. Endod Topics. 2005;12:2–24.
- Use of Silver Points. Position Statement of the American Association of Endodontists 2013. Available at: https://www.aae.org/uploadedfiles/publications_and_research/guidelines_and_position_statements/silverpointsstatement.pdf. Accessed May 2, 2016.
- Concerning Paraformaldehyde-Containing Endodontic Filling Materials and Sealers. Position Statement of the American Association of Endodontists 2013. Available at: https://www.aae.org/uploadedfiles/publications_and_research/guidelines_and_position_statements/paraformaldehydefillingmaterials.pdf. Accessed May 2, 2016.
- Ray HA, Trope M. Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. Int Endod J. 1995;28:12–18.
- Torabinejad M, Ung B, Kettering JD. In vitro bacterial penetration of coronally unsealed endodontically treated teeth. J Endod. 1990;16:566–569.
- Gillen BM, Looney SW, Gu L-S, Loushine BA, Weller RN, Loushine RJ, Pashley DH, Tay FR. Impact of the quality of coronal restoration versus the quality of root canal fillings on success of root canal treatment: a systematic review and meta-analysis. J Endod. 2011;37:895–902.
- Salehrabi R, Rotstein I. Endodontic treatment outcomes in a large patient population in the USA: an epidemiological study. J Endod. 2004;30:846–850.
- Suter B, Lussi A, Sequeira P. Probability of removing fractured instruments from root canals. Int Endod J. 2005;38:112–123.
- Gluskin AH. Mishaps and serious complications in endodontic obturation. Endod Topics. 2005;12:52–70.
- Gluskin AH. Anatomy of an overfill: a reflection on the process. Endod Topics. 2009;16:64–81.
- Pogrel MA. Damage to the inferior alveolar nerve as the result of root canal therapy. J Am Dent Assoc. 2007;138:65–69.
- Gluskin AH, Ruddle CJ, Zinman EJ. Thermal injury through intraradicular heat transfer using ultrasonic devices: precautions and practical preventive strategies. J Am Dent Assoc. 2005;136:1286–1293.
- Witton R, Henthorn K, Ethunandan M, et al. Neurological complications following extrusion of sodium hypochlorite solution during root canal treatment. Int Endod J. 2005;38:843–848.
- Matthews J, Merrill RL. Sodium hypochlorite-related injury with chronic pain sequelae. J Am Dent Assoc. 2014;145:553–555.
Featured photo courtesy of COSMIN4000/ISTOCK/ THINKSTOCK
From Decisions in Dentistry. November 2016;2(11):26–28, 30.
