
Update on Breath Malodor
By understanding the pathogenesis of breath malodor, as well as strategies for its assessment and management, clinicians can effectively address this common condition.
By understanding the pathogenesis of breath malodor, as well as strategies for its assessment and management, clinicians can effectively address this common condition.
The author has no commercial conflicts of interest to disclose.
This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the epidemiology and pathogenesis of breath malodor.
- Identify the classifications of breath malodor.
- List the strategies for assessing this common problem.
- Explain solutions for managing breath malodor.
Halitosis, bad breath and oral malodor are terms used for breath malodor. While some may dismiss it as a matter of semantics, recognizing the difference between bad breath and oral malodor is important. The former may have origins in sites other than the mouth, while oral malodor starts in the oral cavity. Dental professionals play the greatest role in managing oral malodor, which is the primary focus of this review.
The semantic argument for use of the terms halitosis, bad breath and oral malodor is of clinical relevance because oral malodor is a restrictive term that should not be confused with odor arising from recent food ingestion, smoking, alcohol consumption, extraoral sources or psychological conditions. Oral malodor should also not be confused with morning breath malodor, as the latter arises from decreased salivary flow during sleep, and generally disappears after morning oral hygiene regimens. Oral malodor is the most common form of halitosis and is associated mainly with the presence of volatile sulfur compounds — produced by oral bacteria — that have a particularly acrid smell.1–3
Oral malodor is considered a symptom rather than the outcome of a specific pathologic process. Surprisingly, this important and often debilitating condition continues to be poorly understood, and is generally overlooked by the dental profession. Despite a large body of literature on the topic, little is known about oral malodor’s epidemiology and impact on quality of life. There are few, if any, evidence-based systematic reviews with meta-analyses on the management of oral malodor.
EPIDEMIOLOGY AND CLASSIFICATION
The incidence of chronic breath malodor is poorly understood. The incidence of halitosis ranges from 2% to 30% of the world’s population, according to a number of studies.4–7 Evidence indicates that 25% to 40% of the population of industrialized countries experience this condition.8 Nearly 90% of breath malodor cases arise from the oral cavity and are associated with poor oral hygiene, gingivitis, periodontitis, dental caries and tongue coatings.8 Of the remaining cases, sinus or gastrointestinal problems account for around 5%, with other etiologies (5%) accounting for the remainder.8
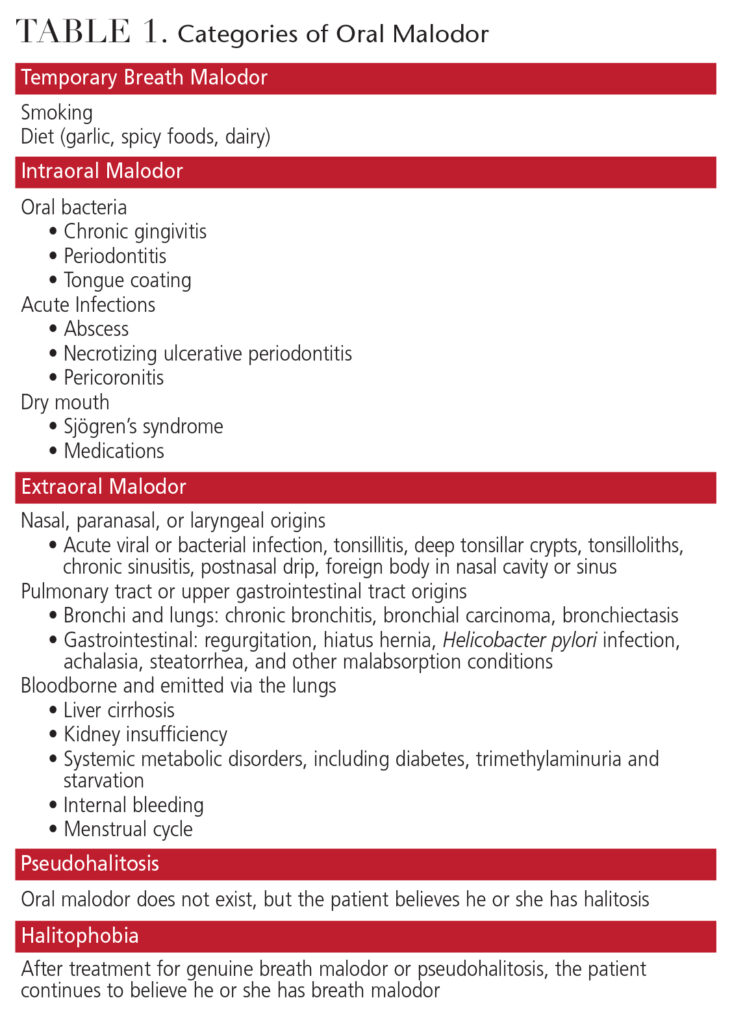 A classification for breath malodor originally described in Japan in 1999 by Miyazaki et al9 was subsequently presented in English by Yaegaki and Coil.10 This classification categorizes breath malodor as temporary, intraoral, extraoral, pseudohalitosis or halitophobia (Table 1). Such classifications support rational treatment decisions based on the overall diagnosis of the condition. Of these conditions, the most important distinction is between intraoral and extraoral breath malodor, as these represent the presence of legitimate breath malodor.
A classification for breath malodor originally described in Japan in 1999 by Miyazaki et al9 was subsequently presented in English by Yaegaki and Coil.10 This classification categorizes breath malodor as temporary, intraoral, extraoral, pseudohalitosis or halitophobia (Table 1). Such classifications support rational treatment decisions based on the overall diagnosis of the condition. Of these conditions, the most important distinction is between intraoral and extraoral breath malodor, as these represent the presence of legitimate breath malodor.
Intraoral breath malodor is used to describe cases in which the source of the problem can be found within the oral cavity, including tongue coating and pathologic conditions, such as gingivitis, periodontitis, ulcers and caries. Extraoral breath malodor is subdivided into bloodborne and nonbloodborne. The terms pseudohalitosis and halitophobia describe conditions in which patients believe they have breath malodor, but no such condition can be confirmed following clinical assessment. The condition of temporary breath malodor is generally associated with tobacco use or consuming various types of food or drink.
PATHOGENESIS AND ASSESSMENT
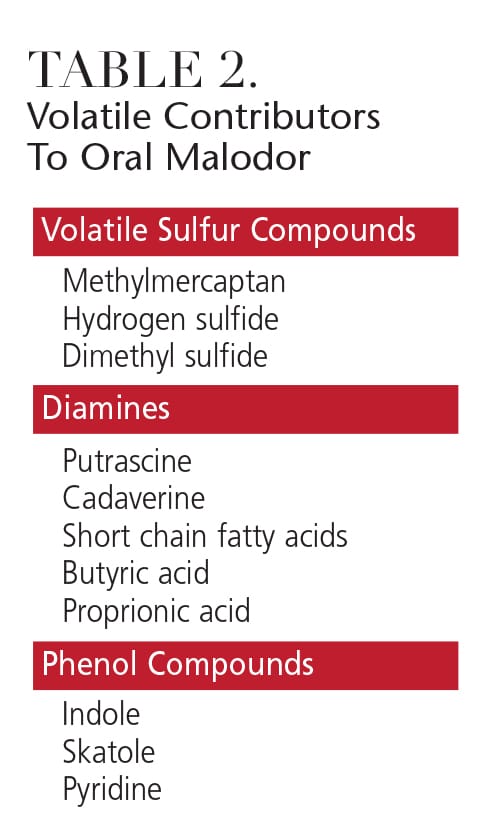
Oral malodor is caused principally by the degradation of organic material by anaerobic bacteria associated with periodontal disease.11–13 These bacteria produce the bad smell, which is composed of volatile sulfur compounds, diamines and phenyl compounds (Table 2).3,14 Of these, volatile sulfur compounds — including methylmercaptan, hydrogen sulfide and dimethyl sulfide — have been most extensively studied. Evidence suggests that oral malodor is associated with elevated levels of methylmercaptan and hydrogen sulfide, while breath malodor from nonoral sources may be associated with dimethyl sulfide.15
 The bacteria principally responsible for the production of methylmercaptan and hydrogen sulfide are associated with the subgingival biofilm present in gingivitis and periodontitis — although they are also found on the dorsum of the tongue. Some studies have suggested that, in addition to periodontal disease, oral malodor is directly related to the total bacterial load in tongue coatings and saliva.16,17
The bacteria principally responsible for the production of methylmercaptan and hydrogen sulfide are associated with the subgingival biofilm present in gingivitis and periodontitis — although they are also found on the dorsum of the tongue. Some studies have suggested that, in addition to periodontal disease, oral malodor is directly related to the total bacterial load in tongue coatings and saliva.16,17
A thorough history, both medical and dental, is an essential starting point when assessing patients for breath malodor. The medical history should include questions relating to current medications, nasal and sinus conditions, snoring and sleep apnea, mouth breathing, throat infections, tonsilloliths, and an assessment of ingestion of foods that may contribute to breath malodor.
The dental history should focus on whether general dental care has been maintained through regular dental visits and oral hygiene practices, including frequency of toothbrushing and the use of other oral hygiene aids, such as floss, interdental cleaning aids, mouthrinses and tongue cleaners/scrapers. Specific questions relating to the oral malodor must also be addressed, such as how long the problem has existed, whether it is worse at a particular time of day, and whether anyone has commented on the problem.
Following the initial interview, both an oral evaluation and breath analysis are required.18 The oral evaluation should include an assessment of the tonsils, oral debris, caries, exposed pulps, extraction wounds, interdental food impaction, gingivitis, periodontitis, necrotizing periodontal conditions, peri-implantitis, pericoronitis and recurrent oral ulcerations.
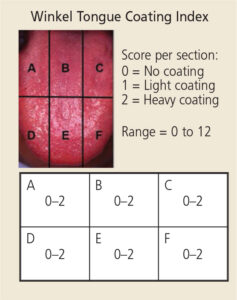
An assessment of tongue coating is also an integral part of the oral assessment for breath malodor. An index for assessing tongue coatings has been used in which the dorsum of the tongue is divided into six sections (Figure 1).19 The presence of any tongue coating is then graded and recorded for each of the sections. If no coating is present, a score of 0 is given; a light, thin coating is given a score of 1; and a heavy, thick coating is given a score of 2. The final score, ranging from 0 to 12, is calculated by adding the six section scores.
An assessment of the quantity and quality of saliva is also important. One consequence of reduced salivary flow and dry mouth is increased bacterial growth due to the absence or reduction of saliva’s antibacterial properties. With the increased bacterial load, there is an associated increase in the release of volatile sulfur compounds and, thus, an increase in oral malodor.
After the oral examination, a breath odor evaluation is conducted. There are numerous ways in which this can be done, including organoleptic testing (i.e., smelling patient’s breath) or the use of instruments.
INSTRUMENT ASSESSMENT
While there are many methods for assessing breath malodor, instrument analysis for the presence of volatile sulfur compounds is recommended because it provides a degree of objective assessment.20,21 A variety of devices is available, but one is able to distinguish the three major volatile sulfur compounds (hydrogen sulfide, methylmercaptan and dimethyl sulfide) associated with halitosis. Sample collection is achieved by placing a disposable syringe in the mouth with the lips sealed for 30 seconds, with the contents then injected into a chromatograph. Analysis takes eight minutes, after which the resulting printout depicts the levels of the three volatile sulfur compounds. This provides immediate assessment of whether the source of the oral malodor is likely due to the oral cavity or elsewhere.
MANAGEMENT STRATEGIES
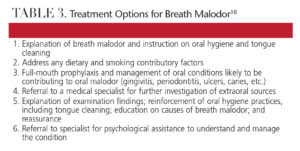
The treatment options for breath malodor can be divided into six categories (Table 3).10,18 Temporary, intraoral and pseudohalitosis can be managed by oral health care professionals — however, extraoral halitosis and halitophobia will require the assistance of physicians, psychiatrists and/or psychologists.
 Oral malodor is suspected if elevated levels of hydrogen sulfide and methylmercaptan are present. Conversely, an extraoral source of breath malodor is likely if dimethyl sulfide readings are high.15 Once a diagnosis of oral malodor (as distinct from breath malodor) is made, treatment of the oral condition can commence. Ideally, this will be cause-related and involve a multistep approach. If temporary breath malodor is suspected, assessment and management of dietary components are essential to eliminate the intake of strong-smelling foods and drinks, such as garlic, onions and alcohol. This initial aspect of management should be followed for all five breath malodor classifications. In addition, all dental diseases — including gingivitis, periodontitis, ulcers and dental caries — must be diagnosed and effectively managed.
Oral malodor is suspected if elevated levels of hydrogen sulfide and methylmercaptan are present. Conversely, an extraoral source of breath malodor is likely if dimethyl sulfide readings are high.15 Once a diagnosis of oral malodor (as distinct from breath malodor) is made, treatment of the oral condition can commence. Ideally, this will be cause-related and involve a multistep approach. If temporary breath malodor is suspected, assessment and management of dietary components are essential to eliminate the intake of strong-smelling foods and drinks, such as garlic, onions and alcohol. This initial aspect of management should be followed for all five breath malodor classifications. In addition, all dental diseases — including gingivitis, periodontitis, ulcers and dental caries — must be diagnosed and effectively managed.
The overriding principle for management of intraoral breath malodor is reducing the bacterial burden. An effective and regular oral hygiene regimen (brushing and interdental cleaning) must be implemented, and should include twice-daily tongue cleaning.20,22,23 Due to the potential damage to the tongue surface, some clinicians do not recommend tongue scraping and prefer gentle brushing with a small, soft-bristle brush.10 Use of a proven antibacterial toothpaste is recommended.
Rendering malodorous gases nonvolatile should also be an aim when managing oral malodor and can be achieved through several means. Increasing salivary flow boosts the solubility of volatile sulfur compounds and can help lessen noticeable effects of malodor. Drinking water frequently can reduce malodor for an hour. Beyond these approaches, the adjunctive use of antiseptic mouthrinses is essential to ensure a satisfactory outcome in the management of oral malodor.24,25
While chlorhexidine remains the gold standard for chemical plaque control, it is best used only in the short term for treating oral malodor. Emerging evidence suggests that formulations with cetylpyridinium chloride, zinc ions or essential oils may be helpful.19,26–28 These formulations work by reducing the overall bacterial load and also have a dilution effect on the malodor. The addition of zinc is particularly interesting because it appears to have both an antibacterial effect and the ability to neutralize volatile sulfur compounds.29 Thus, mouthrinses and toothpastes containing zinc are emerging as helpful tools in managing oral malodor.
ALTERNATIVE APPROACHES
Probiotics have been proposed as adjuncts in the management of both intraoral and extraoral breath malodor.30 The use of probiotics for oral malodor is based on the bacterial origin of this condition.31 Consequently, controlling the reappearance of odiferous bacteria following conventional mechanical cleaning by the introduction of nonodiferous, commensal bacteria to colonize the oral cavity is an attractive proposal.31 To date, studies investigating the use of probiotics as an adjunctive aid for management of oral malodor have been equivocal and are not universally accepted as a method to control oral malodor.32,33
The use of agents that merely mask the offensive smell of oral malodor is generally of limited value. These agents include mouthrinses, sprays, lozenges and chewing gum. While these will most likely have short-term effects, they are not a definitive treatment and may delay an accurate diagnosis.
An extraoral source of breath malodor is usually suspected if dimethyl sulfide readings are high.15 In these cases, additional assessment and tests are required. If deemed appropriate, referral to a physician specializing in management of nasal, throat or gastrointestinal abnormalities may be necessary. These may also be accompanied by blood tests for kidney insufficiency, liver insufficiency/dysfunction, and metabolic diseases.
While the management of oral malodor is not the most glamorous aspect of dentistry, it is a fascinating and important aspect of patient care. For many patients, oral malodor is a significant problem that affects their quality of life. Through the use of modern technology and the increased understanding of the role certain bacteria play in oral malodor, the management of this condition is becoming more predictable.
References
- Delanghe G, Ghyselen J, Feenstra L, van Steenberghe D. Experiences of a Belgian multidisciplinary breath odour clinic. Acta Otorhinolaryngol Belg. 1997;51:43–48.
- Delanghe G, Ghyselen J, van Steenberghe D, Feenstra L. Multidisciplinary breath-odour clinic. Lancet. 1997;350:187.
- Tonzetich J. Production and origin of oral malodor: a review of mechanisms and methods of analysis. J Periodontol. 1977;48:13–20.
- Söder B, Johansson B, Söder PO. The relation between foetor ex ore, oral hygiene and periodontal disease. Swed Dent J. 2000;24:73–82.
- Miyazaki H, Sakao S, Katoh Y, Takehara T. Correlation between volatile sulphur compounds and certain oral health measurements in the general population. J Periodontol. 1995;66:679–684.
- Liu XN, Shinada K, Chen XC, Zhang BX, Yaegaki K, Kawaguchi Y. Oral malodor related parameters in the Chinese general population. J Clin Periodontol. 2006;33:31–36.
- Nadanovsky P, Carvalho LB, Ponce de Leon A. Oral malodour and its association with age and sex in a general population in Brazil. Oral Dis. 2007;13:105–109.
- Zalewska A, Zatoñski M, Jabłonka-Strom A, Paradowska A, Kawala B, Litwin A. Halitosis — a common medical and social problem. A review on pathology, diagnosis and treatment. Acta Gastroenterol Belg. 2012;75:300–309.
- Miyazaki H, Arao M, Okamura K, et al. Tentative classification of halitosis and its treatment needs (Japanese). Niigata Dental Journal. 1999;32:7–11.
- Yaegaki K, Coil JM. Examination, classification, and treatment of halitosis; clinical perspectives. J Can Dent Assoc. 2000;66:257–261.
- Loesche WJ, Kazor C. Microbiology and treatment of halitosis. Periodontol 2000. 2002;28:256–279.
- Persson S, Edlund MB, Claesson R, Carlsson J. The formation of hydrogen sulfide and methyl mercaptan by oral bacteria. Oral Microbiol Immunol. 1990;5:195–201.
- McNamara TF, Alexander JF, Lee M. The role of microorganisms in the production of oral malodor. Oral Surg Oral Med Oral Pathol. 1972;34:41–48.
- Scully C, Greenman J. Halitology (breath odour: aetiopathogenesis and management). Oral Dis. 2012;18:333–345.
- Tangerman A, Winkel EG. Volatile sulfur compounds as the cause of bad breath: a review. Phosphorous, Sulfur and Silicon. 2013;188:396–402.
- Tonzetich J, Kestenbaum RC. Odour production by human salivary fractions and plaque. Arch Oral Biol. 1969;14:815–827.
- De Boever EH, Loesche WJ. Assessing the contribution of anaerobic microflora of the tongue to oral malodor. J Am Dent Assoc. 1995;126:1384–1393.
- Seemann R, Conceicao MD, Filippi A, et al. Halitosis management by the general dental practitioner — results of an international consensus workshop. J Breath Res. 2014;8:017101.
- Winkel EG, Roldán S, Van Winkelhoff AJ, Herrera D, Sanz M. Clinical effects of a new mouthrinse containing chlorhexidine, cetylpyridinium chloride and zinc-lactate on oral halitosis. A dual-center, double-blind placebo-controlled study. J Clin Periodontol. 2003;30:300–306.
- Dadamio J, Laleman I, De Geest S, et al. Usefulness of a new malodour-compound detection portable device in oral malodour diagnosis. J Breath Res. 2013;7:046005.
- Laleman I, Dadamio J, De Geest S, Dekeyser C, Quirynen M. Instrumental assessment of halitosis for the general dental practitioner. J Breath Res. 2014;8:017103.
- van den Broek AM, Feenstra L, de Baat C. A review of the current literature on management of halitosis. Oral Dis. 2008;14:30–39.
- Outhouse TL, Al-Alawi R, Fedorowicz Z, Keenan JV. Tongue scraping for treating halitosis. Cochrane Database Syst Rev. 2006;2:CD005519.
- Quirynen M, Zhao H, Soers C, et al. The impact of periodontal therapy and the adjunctive effect of antiseptics on breath odor-related outcome variables: a double-blind randomized study. J Periodontol. 2005;76:705–172.
- Quirynen M, Zhao H, van Steenberghe D. Review of the treatment strategies for oral malodour. Clin Oral Investig. 2002;6:1–10.
- Young A, Jonski G, Rölla G. Combined effect of zinc ions and cationic antibacterial agents on intraoral volatile sulphur compounds (VSC). Int Dent J. 2003;53:237–242.
- van Steenberghe D, Avontroodt P, Peeters W, et al. Effect of different mouthrinses on morning breath. J Periodontol. 2001;72:1183–1191.
- Fine DH, Furgang D, Sinatra K, Charles C, McGuire A, Kumar LD. In vivo antimicrobial effectiveness of an essential oil-containing mouth rinse 12 h after a single use and 14 days’ use. J Clin Periodontol. 2005;32:335–340.
- Dadamio J, Van Tournout M, Teughels W, Dekeyser C, Coucke W, Quirynen M. Efficacy of different mouthrinse formulations in reducing oral malodour: a randomized clinical trial. J Clin Periodontol. 2013;40:505–513.
- Burton JP, Chilcott CN, Moore CJ, Speiser G, Tagg JR. A preliminary study of the effect of probiotic Streptococcus salivarius K12 on oral malodour parameters. J Appl Microbiol. 2006;100:754–764.
- Teughels W, Van Essche M, Sliepen I, Quirynen M. Probiotics and oral healthcare. Periodontol 2000. 2008;48:111–147.
- Masdea L, Kulik EM, Hauser-Gerspach I, Ramseier AM, Filippi A, Waltimo T. Antimicrobial activity of Streptococcus salivarius K12 on bacteria involved in oral malodour. Arch Oral Biol. 2012;57:1041–1047.
- Suzuki N, Yoneda M, Tanabe K, et al. Lactobacillus salivarius WB21-containing tablets for the treatment of oral malodor: a double-blind, randomized, placebo-controlled crossover trial. Oral Surg Oral Med Oral Pathol Oral Radiol. 2014;117:462–470.

