

Recognize the Signs Of Domestic Violence
Oral health professionals need to be aware of the symptoms of domestic violence and how to assist victims.
Oral health professionals need to be aware of the symptoms of domestic violence and how to assist victims.
The authors have no commercial conflicts of interest to disclose.
This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Define the “ask, validate, document, and refer/report if required by law” model for inquiring about domestic violence.
- Identify common signs of overall abuse and abuse specific to the head and neck region.
- Discuss the role of the dentist in ensuring dental exams are as stress-free as possible.
Domestic violence is defined by the U.S. Centers for Disease Control and Prevention as “physical, sexual or psychological harm by a current or former partner or spouse which can occur among heterosexual or same-sex couples and does not require sexual intimacy.”1 Domestic violence, also known as intimate partner violence, is a serious yet preventable public health issue.
As such, it is important for dental professionals to understand the dynamics of abuse and the purposeful tactics that abusers use to gain power and control over their partners. Power is not inherently evil, and many forms of power imbalance exist in society for legitimate purposes. For example, teachers have power over students, parents over children, and police over the general public. Some people, however, try to gain power over others they have no right to claim, and some individuals in positions of power choose to abuse it by means of violence, threats or coercion. Table 1 lists examples of tactics that abusers use to exert control over their partners.2
While there are many definitions of abuse, its dynamics are complex. Context is key to understanding the full story, and while the dentist can never know everything about a patient’s history and circumstances, asking relevant background questions is important when performing assessments. Just as a diagnosis would not be made in the dental operatory without a full medical, social and physical history, conclusions cannot be drawn from a fraction of the picture while assessing a patient who may be a victim of domestic violence.
Many public health initiatives aim to educate patients and lessen the prevalence of obesity, smoking and other preventable issues, yet domestic violence can also be considered a public health issue. Preventing and easing the burden of domestic violence begins with creating awareness among health care providers. At least one in three American women has been physically or sexually assaulted by a boyfriend, husband or partner at some point.3 Domestic violence is also an important dental health issue, as 75% of injuries from family violence are sustained in the head, face and/or mouth.4
The lack of response in the face of this prevalent health issue is alarming. In a survey of 407 dentists, only 7% reported having suspected a case of elder abuse and only 1% filed a report.5 A second survey of 321 dentists found that 87% reported never having screened for any kind of domestic violence.5 The dental health care team is in a unique position to recognize domestic violence and offer support to victims to attain an improved quality of life and overall health. In four studies of survivors of abuse, 70% to 81% of respondents reported that they would like their health care providers to ask them privately about intimate partner violence.6–10
![0216_violence-1]() IMPLEMENT THE AVDR MODEL
IMPLEMENT THE AVDR MODEL
 IMPLEMENT THE AVDR MODEL
IMPLEMENT THE AVDR MODELThe “ask, validate, document, and refer/report if required by law” (AVDR) model can be used by dental health care providers to effectively inquire about, and respond to, domestic violence. Barbara Gerbert, PhD, director of the Center for Health Improvement and Prevention Studies, along with colleagues at the University of California, San Francisco School of Dentistry, developed a brief tutorial with case studies to demonstrate this intervention in action;11 it’s available at futureswithoutviolence.org.
Dental health care providers should aim to practice from a trauma-informed perspective.12 This includes recognizing that any patient who walks into the operatory may have a current or past history of abuse or trauma, regardless of whether it is disclosed or he or she appears like a victim or an abuser.12 This assumption enables clinicians to treat patients with sensitivity and reduces the potential for retraumatization. During verbal, extraoral and intraoral screenings, clinicians may detect subtle warning signs.
All patients should be screened for domestic violence. And in order to prevent the feeling of being singled out, each patient should be informed that all patients are asked about domestic violence as a part of routine screening.
Prior to inquiring about domestic violence, the following precautions must be taken: the patient is alone; an appropriate interpreter is present, if needed; the patient is aware of limits to confidentiality; and the clinician knows how to respond if abuse is disclosed.11 For this reason, it is critical that dentists and others planning to begin routinely assessing for domestic violence be properly trained by, and have a relationship with, an appropriate domestic violence program/provider.
![0216_violence-2]() VALIDATE AND DOCUMENT
VALIDATE AND DOCUMENT
 VALIDATE AND DOCUMENT
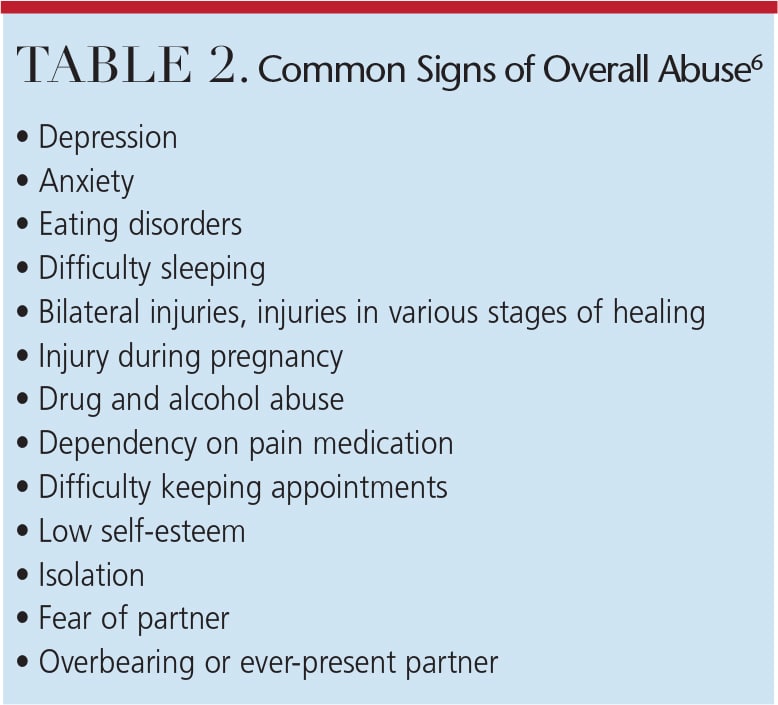
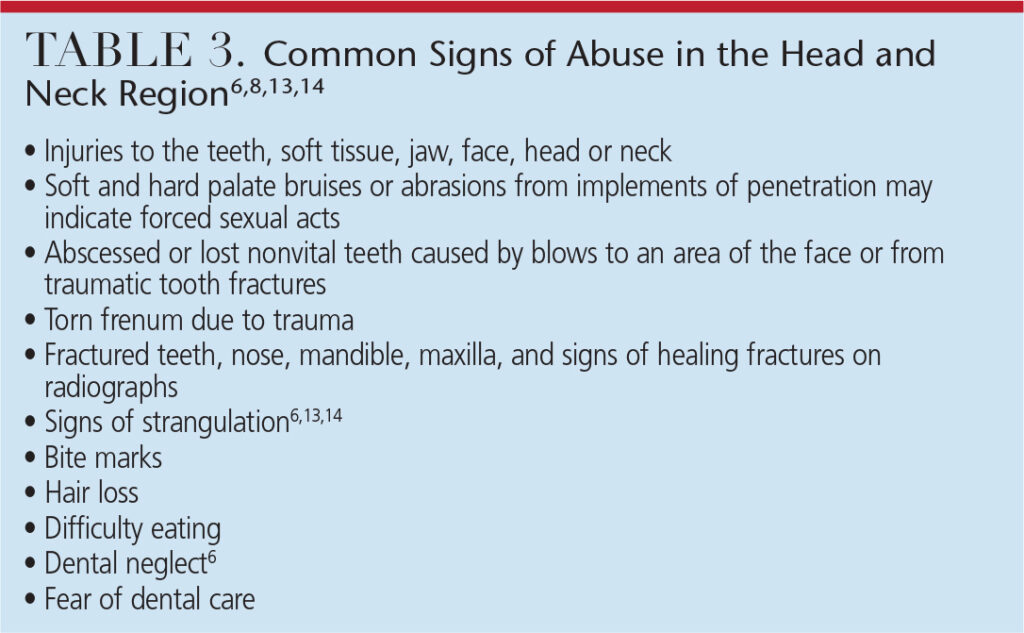
VALIDATE AND DOCUMENTIn addition to asking patients about domestic violence, clinicians should look for signs of abuse. Table 2 and Table 3 provide a list of the manifestations of abuse.6,8,13,14 Often, the signs are subtle, so it is important to listen carefully and be observant while performing extraoral and intraoral exams.
When asking direct questions about abuse, using “framing statements” may make clinicians and patients feel more comfortable. For example:
- The clinician notes an injury and suspects it may be due to domestic violence. The clinician says, “This type of bruising often occurs when someone grabs your face really hard. Was the injury to your face accidental or did someone do this to you?”
- If the clinician wishes to convey concern about an observed behavior and create an opening for the patient to share more, he or she might comment, “Your partner seemed really angry when we asked him (or her) to step out. Are you afraid of him or do you ever feel unsafe? Will you feel safe leaving with him today?”
- Oral health professionals can ask inquiry questions as part of routine screening. For example, the clinician might say, “We know that some of our patients are unsafe in their relationships, which can lead to health problems. Is anyone hurting you, controlling you, or making you afraid?”
 Validating statements can facilitate conversations between clinicians and patients. This approach will help prevent patients from feeling like they are being judged or that clinicians are jumping to conclusions. Practitioners must be careful to avoid victim blaming or extreme statements if abuse is disclosed. As an outsider, it may be difficult to understand why some victims stay with an abusive partner, or appear to deny or minimize the abuse. Whatever the case, clinicians do not comprehend the full picture of patients’ experiences or their reasons behind their decision making. It is not clinicians’ place to judge, but rather to respect patients’ autonomy and support them in an appropriate and individualized manner.11
Validating statements can facilitate conversations between clinicians and patients. This approach will help prevent patients from feeling like they are being judged or that clinicians are jumping to conclusions. Practitioners must be careful to avoid victim blaming or extreme statements if abuse is disclosed. As an outsider, it may be difficult to understand why some victims stay with an abusive partner, or appear to deny or minimize the abuse. Whatever the case, clinicians do not comprehend the full picture of patients’ experiences or their reasons behind their decision making. It is not clinicians’ place to judge, but rather to respect patients’ autonomy and support them in an appropriate and individualized manner.11
Documenting the interaction with the patient and the signs/symptoms observed is crucial for the patient’s health, as well as legal purposes. The following tips should be considered during the documentation process: use the patient’s words and/or describe the patient’s demeanor; record objective clinical findings; describe (or photograph) the location, size, shape, color, nature of injuries, or other conditions in detail; and record the treatment plan, follow-up instructions, referrals and reports made.11 Again, training is important prior to beginning routine documentation of domestic violence disclosures in the medical record so that dental providers will know how to maintain appropriate patient confidentiality and legal protection.
Upon asking the initial questions, if no abuse is reported, accept the patient’s response and respect the individual’s right to self-determination. If abuse is suspected due to injuries or other behaviors despite the lack of disclosure, concern for the patient’s safety and health should be expressed without conveying judgment of the victim or partner. The clinician should let the patient know that he or she is always welcome to seek help through the dental practice. The steps taken during the appointment should be documented in the patient’s record.11
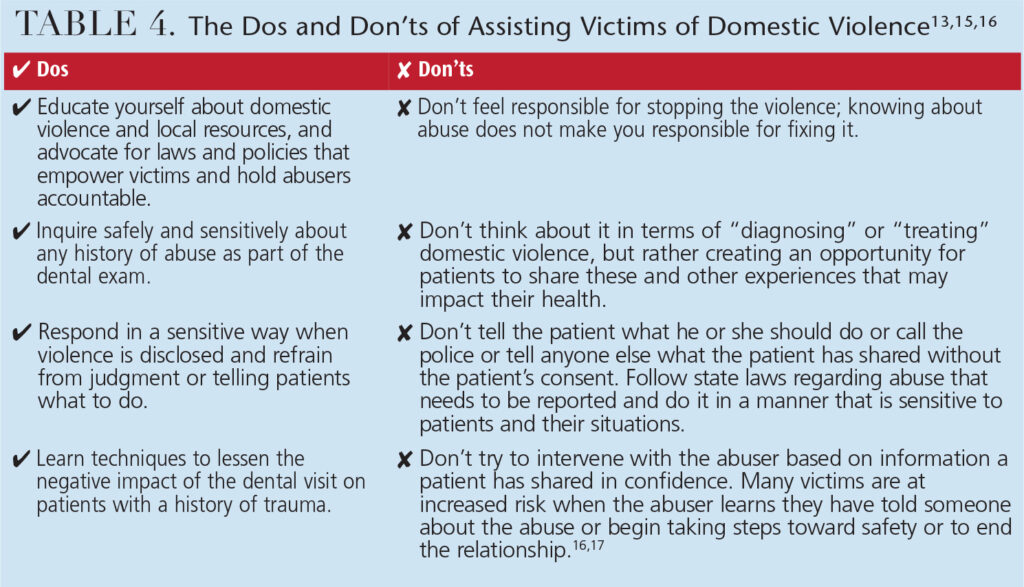
If a patient discloses past or current abuse, the clinician should listen, acknowledge and validate the patient’s concerns. Clinicians should explore how the abuse is impacting the patient’s dental situation and how he or she has coped thus far. The patient can be asked if he or she has someone to talk to and whether he or she has any concerns about safety. Only those elements of the discussion that are directly related to patient care should be documented in the patient’s record. Table 4 includes additional tips for assisting victims of domestic violence.13,15,16
![0216_violence-8]() DEVELOP A PLAN
DEVELOP A PLAN
 DEVELOP A PLAN
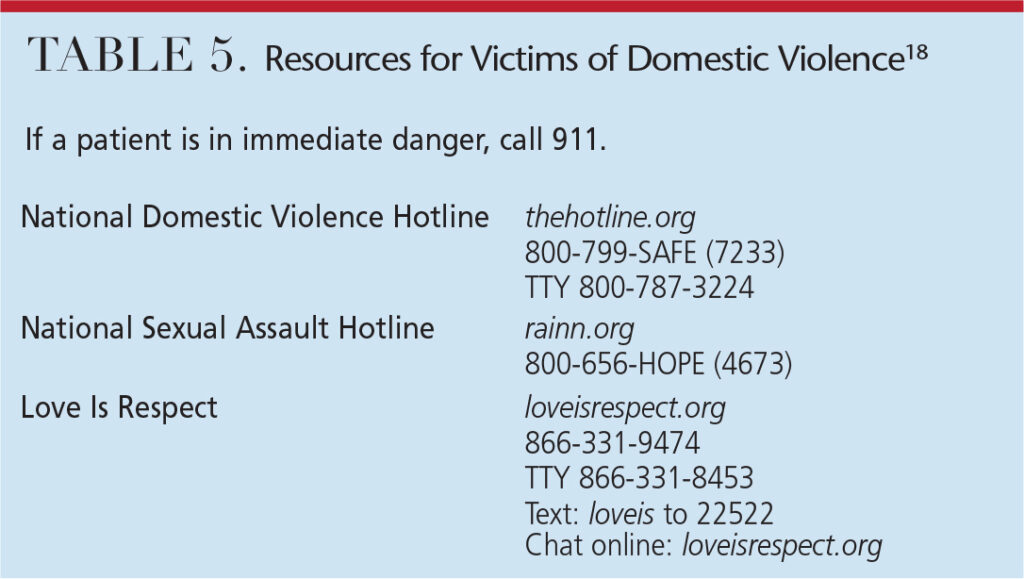
DEVELOP A PLANDental practices should have a plan of action in case patients disclose abuse. First and foremost, safety concerns should be addressed immediately. Concern should be expressed and assistance offered with contacting authorities or an abuse hotline. Laws vary from state to state regarding what types of abuse and what indicators are reportable to law enforcement and/or protective services, so dental providers should receive training about the laws in their state prior to implementing screening for any type of abuse.17 But regardless of legal mandates, national and local resources are available to help victims (Table 5).18
Appropriate referral information should be provided in writing — or verbally, if it is unsafe for the patient to take or write down numbers. Keep in mind that risks are complex and vary for each victim. If an abuser perceives a loss of control, which often happens if he/she learns that the victim is seeking help, the victim’s risk may increase. Clinicians should ask patients directly if it is safe to take the information they are offering, and be creative about giving information discretely, such as providing a generic business card or resource list that includes hotline numbers.
Patients who have been victims of domestic violence can find dental appointments stressful. From their point of view, it is a situation in which they feel they have no control, and they may feel frightened, helpless, or as if they are experiencing a past incident of abuse. Before the exam begins, patients should be asked about their anxiety level and what can be done to make them more comfortable. Clinicians should explain procedures and apprise patients of what’s to come. Keeping patients informed can help make dental appointments less traumatic.
![0216_violence-9]() CURRICULUM IN ACTION
CURRICULUM IN ACTION
 CURRICULUM IN ACTION
CURRICULUM IN ACTIONTufts University School of Dental Medicine in Boston provides its students with a four-year comprehensive curriculum that includes both didactic and clinical aspects of domestic violence education. During years 1, 2 and 3, lectures on domestic violence given by local experts are integrated into the coursework. During years 3 and 4, students treat patients who are or have been victims of domestic violence through the Dental Outreach to Survivors (DOTS) program. When the students receive their patients in the clinic, they conduct a domestic violence assessment. This helps regulate the screening process and creates a trauma-informed practice; it also assists future dental providers in becoming more comfortable assessing domestic violence. The AVDR model is followed under the supervision of faculty and staff.
The DOTS program was founded in 2003 to provide safe and confidential care to victims of violence by giving them free dental care and de-identifying the patients in the electronic medical/dental record system to keep them anonymous from their perpetrators. This umbrella of care is open to any victim, regardless of gender or sexual orientation.
The best way for oral health care providers to eliminate domestic violence is to become educated about this public health issue. It is crucial to understand what domestic violence is, how it manifests, and how to recognize and help its victims.
References
- Centers for Disease Control and Prevention. Intimate Partner Violence: Definitions. Available at: http://www.cdc.gov/violenceprevention/intimatepartnerviolence/definitions.html. Accessed January 11, 2016.
- Domestic Abuse Intervention Programs. Wheel Gallery. Available at: theduluthmodel.org/training/wheels.html. Accessed January 11, 2016.
- Collins KS, Schoen C, Joseph S, Duchon L, Simantov E, Yellowitz M. Health Concerns Across a Woman’s Lifespan: The Commonwealth Fund 1998 Survey of Women’s Health. Available at: http://www.commonwealthfund.org/publications/fund-reports/1999/may/health-concerns-across-a-womans-lifespan–the-commonwealth-fund-1998-survey-of-womens-health. Accessed January 11, 2016.
- Sweet D. Recognizing and intervening in domestic violence: proactive role for dentistry. Medscape Womens Health. 1996;1:3.
- Gironda M, Lefever K, Anderson E. Dental students’ knowledge about elder abuse and neglect and the reporting responsibilities of dentists. J Dent Educ. 2010;74:824–829.
- Futures Without Violence. Enhancing Dental Professionals’ Response to Domestic Violence. Available at: futureswithoutviolence.org/userfiles/file/HealthCare/dental.pdf. Accessed January 11, 2016.
- Caralis PV, Musialowski R. Women’s experiences with domestic violence and their attitudes and expectations regarding medical care of abuse victims. South Med J. 1997;90:1075–1080.
- McCauley J, Yurk R, Jenckes M, Ford D. Inside “Pandora’s Box:” abused women’s experiences with clinicians and health services. J Gen Intern Med. 1998;13:549–555.
- Friedman L, Samet J, Roberts M, Hudlin M, Hans P. Inquiry about victimization experiences: a survey of patient preferences and physician practices. Arch Intern Med. 1992;152:1186–1190.
- Rodriguez M, Quiroga SS, Bauer H. Breaking the silence: battered women’s perspectives on medical care. Arch Fam Med. 1996;5:153–158.
- Futures Without Violence. The Ask, Validate, Document, Refer (AVDR) Tutorial for Dentists. Available at: http://www.futureswithoutviolence.org/?s=The+Ask%2C+Validate%2C+Document%2C+Refer+%28AVDR%29+Tutorial+for+Dentists. Accessed January 11, 2016.
- National Association of State Mental Health Program Directors. The National Center for Trauma Informed Care. Available at: http://www.nasmhpd.org/content/national-center-trauma-informed-care-nctic-0. Accessed January 11, 2016.
- McClane GE, Shanel-Hogan KA, Strack GB. Never Let a Victim Die in Vain. San Diego City Attorney’s Office. 2001.
- Gwinn C, McClane GE, Shanel-Hogan KA, Strack GB. Domestic violence: No place for a smile. J Calif Dent Assoc. 2004;32:399–409.
- Browne A. When Battered Women Kill. New York: The Free Press; 1987.
- Sonkin D, Martin D, Walker LEA. The Male Batterer: A Treatment Approach. New York: Springer; 1985.
- Family Violence Prevention Fund. Compendium of State Statutes and Policies on Domestic Violence and Health Care. Available at: futureswithoutviolence.org/usefiles/file/HealthCare/Compendium%20Final.pdf. Accessed January 11, 2016.
- Futures Without Violence. Get Help. Available at: futureswithoutviolence.org/resources-events/get-help. Accessed January 11, 2016.

