

Improve Outcomes With Minimally Invasive Dentistry
Clinicians can increase long-term clinical success by incorporating the principles of minimally invasive dentistry into caries risk assessment and restorative treatment.
Clinicians can increase long-term clinical success by incorporating the principles of minimally invasive dentistry into caries risk assessment and restorative treatment.
The authors have no commercial conflicts of interest to disclose.
This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Define minimally invasive dentistry.
- Discuss the importance of effective caries risk assessment.
- Identify preventive strategies for individuals at elevated caries risk.
- Explain the minimally invasive approach to restorative treatment.

Minimally invasive (MI) dentistry focuses on preserving healthy tooth structure through prevention, remineralization and minimal intervention for the placement and replacement of restorations.1 This philosophy is not limited to restorative dentistry and, in fact, can be used across all dental platforms in order to provide patients with the most appropriate care. The core concepts of MI dentistry sometimes conflict with what dentists learned during dental school and clinical training. Dentists and clinical staff must be open to new ways of thinking, as a team effort is required to achieve success with MI dentistry. As one example of an effective team approach, dental hygienists — who typically spend 30 to 60 minutes with patients at least every six months — can play a pivotal role in educating patients about MI dentistry and the importance of an optimal self-care regimen.2
The principles of MI dentistry have evolved as our understanding of the caries process has grown. Today, more is known about the potential for remineralization and the enduring restorative cycle teeth undertake after tooth structure is removed and restored. In addition, new adhesive restorative materials have been introduced. The cornerstones of MI dentistry include risk assessment (with a focus on early disease detection and prevention); remineralization strategies; use of biocompatible dental materials that enable minimal intervention for placement of restorations; and a shift in focus (when possible) from replacement to repair.3
In order to implement an effective MI approach, the entire team needs to gain a deeper understanding of the Caries Management by Risk Assessment model, early detection methods and techniques, and management of noncavitated lesions. To provide the most appropriate intervention before dentition is irreversibly damaged, the depth and activity of caries lesions must be assessed and a caries risk assessment performed.


The International Caries Detection and Assessment System is helpful in the visual detection of early noncavitated lesions.4 This system uses visual criteria based on histologic caries depths, and is performed on clean, dry teeth. The system includes two levels to ascertain changes in noncavitated lesions: first (Code 1) and distinct (Code 2) visual changes in enamel. For smooth surfaces, if no lesion is apparent when the tooth is wet, but a noncavitated lesion appears once the tooth is adequately dried, the lesion is classified as Code 1 (Figure 1). If a noncavitated lesion is apparent both when the tooth is wet or dry, it is classified as Code 2 (Figure 2).
For pit and fissure lesions, if there is discoloration confined to the pit and fissure area once the tooth is air dried, the lesion is classified as Code 1 (Figure 3). Conversely, if the discoloration is wider than the natural fissure or fossa, it is classified as Code 2 (Figure 4).
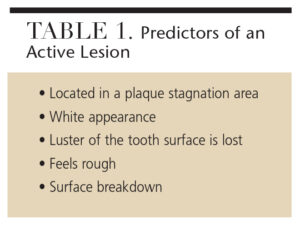
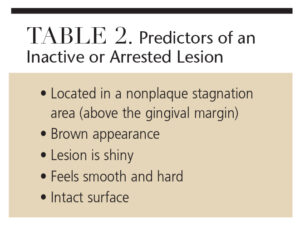
Lesion activity (active versus inactive) is assessed by a number of visual and tactile methods. Table 1 lists the signs of an active lesion, while Table 2 details the characteristics of an inactive or arrested lesion. The combination of these predictors is used to determine the overall activity of the lesion. For example, although the lesion is white (predictor of an active lesion) in Figure 5, it is above the gingival margin and is hard, shiny and intact (predictors of an inactive lesion). As such, this lesion is considered inactive.

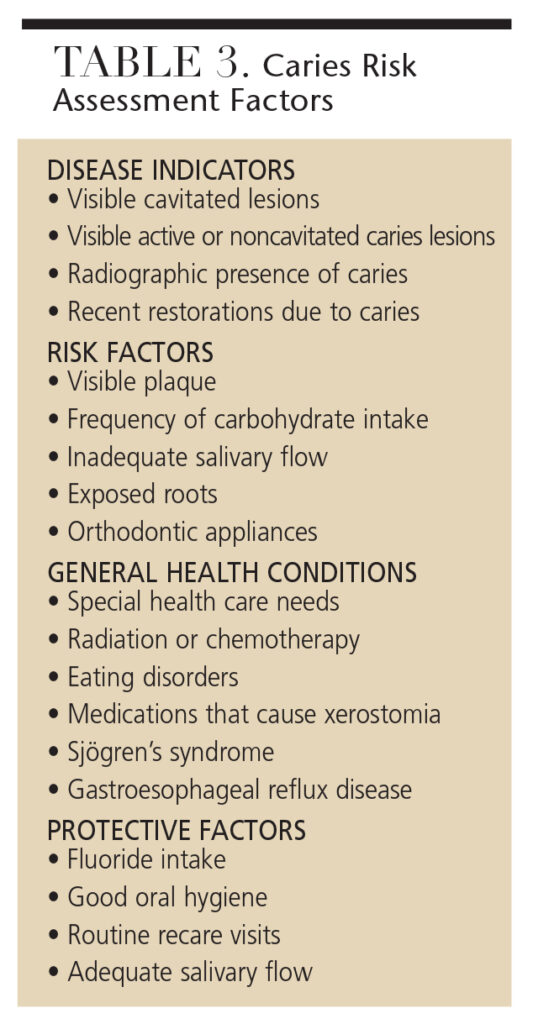
Individual caries risk assessment is determined by a number of elements, including disease indicators, risk factors, general health conditions and protective factors (Table 3). Based on the balance of these factors, the patient’s caries risk (low, moderate or high) can be determined. The American Dental Association,5 American Academy of Pediatric Dentistry,6 and the University of California, San Francisco School of Dentistry, in collaboration with the California Dental Association Foundation,7 all offer effective caries risk assessment tools. The caries risk level, along with individual lesion assessment, assist clinicians in determining appropriate prevention and remineralization strategies.
PREVENTION AND REMINERALIZATION STRATEGIES
 Once the patient’s caries risk assessment is completed and individual lesions have been assessed (based on depth and activity), the information gathered is used to manage noncavitated lesions. The caries process is a dynamic sequence of biofilm and tooth interactions that occur over time. When risk factors outweigh protective factors, there is a shift toward demineralization. Ideally, demineralization can be prevented by increasing protective factors, such as reducing the frequency of fermentable carbohydrate consumption (including acidic beverages); decreasing the number of cariogenic bacteria that produce acid (adequate oral hygiene using fluoride toothpaste); and increasing salivary flow (by using saliva replacements, sugar-free chewing gum with or without xylitol, or a calcium phosphate technology, and/or sugar-free lozenges with or without xylitol).
Once the patient’s caries risk assessment is completed and individual lesions have been assessed (based on depth and activity), the information gathered is used to manage noncavitated lesions. The caries process is a dynamic sequence of biofilm and tooth interactions that occur over time. When risk factors outweigh protective factors, there is a shift toward demineralization. Ideally, demineralization can be prevented by increasing protective factors, such as reducing the frequency of fermentable carbohydrate consumption (including acidic beverages); decreasing the number of cariogenic bacteria that produce acid (adequate oral hygiene using fluoride toothpaste); and increasing salivary flow (by using saliva replacements, sugar-free chewing gum with or without xylitol, or a calcium phosphate technology, and/or sugar-free lozenges with or without xylitol).
 The demineralization process of an active lesion can be arrested and/or reversed, allowing the enamel to strengthen through the remineralization process. For remineralization to occur, the components of saliva (fluoride and calcium phosphate) must be present. Evidence supports the application of topical fluoride as the best strategy for remineralization, based on the patient’s caries risk assessment. In high-risk patients, a prescription dentifrice containing 5000 ppm fluoride may be recommended, in addition to in-office applications of 2.26% fluoride varnish.8 Other products that contain the components of saliva (calcium and phosphate), such as amorphous calcium phosphate, casein phosphopeptide-amorphous calcium phosphate, calcium sodium phosphosilicate and tri-calcium phosphate, can be helpful. But these should not be used as the sole method for promoting remineralization.
The demineralization process of an active lesion can be arrested and/or reversed, allowing the enamel to strengthen through the remineralization process. For remineralization to occur, the components of saliva (fluoride and calcium phosphate) must be present. Evidence supports the application of topical fluoride as the best strategy for remineralization, based on the patient’s caries risk assessment. In high-risk patients, a prescription dentifrice containing 5000 ppm fluoride may be recommended, in addition to in-office applications of 2.26% fluoride varnish.8 Other products that contain the components of saliva (calcium and phosphate), such as amorphous calcium phosphate, casein phosphopeptide-amorphous calcium phosphate, calcium sodium phosphosilicate and tri-calcium phosphate, can be helpful. But these should not be used as the sole method for promoting remineralization.
High-risk patients and those with noncavitated active lesions should be managed with a three-month to four-month reevaluation of caries risk assessment, application of 2.26% fluoride varnish, brushing with 5000 ppm fluoride toothpaste at least twice daily, and the optional use of xylitol (6 g to 10 g/day) and/or calcium phosphate products.7
MINIMAL INTERVENTION FOR RESTORATIVE TREATMENT

Proper diagnosis on the activity, location and cavitation of the lesion, along with caries risk, are essential when determining a treatment plan based on noninvasive caries management. Active noncavitated proximal lesions can be successfully arrested through a combination of improved oral hygiene and repeated application of topical fluoride agents (e.g., varnishes, gels or foams) every three months until caries arrest has been confirmed.9
Depending on patients’ caries risk, proximal lesions can be treated with proximal sealants or a resin infiltration technique. The resin infiltration technique is designed to fill the intercrystalline spaces with a low-viscosity resin to arrest lesions. In contrast to sealants — where the diffusion barrier remains on the enamel surface as a resin coating — the resin infiltration creates a diffusion barrier within the enamel lesion and enables the demineralized enamel structure to strengthen with the resin matrix, preventing lesion formation.10,11 It also strengthens the demineralized enamel structure with the resin matrix, providing mechanical support for the lesion. Additionally, the infiltrated resin modifies the optical properties of early caries lesions, appearing clinically as white spot lesions to blend more with the natural tooth color.12 Occlusal sealants are indicated in active fissure caries or in high-caries-risk patients with fissures that have susceptible morphologic characteristics.9
An in vitro study compared conventional sealing to resin infiltration in occlusal fissure caries lesions. Results showed that infiltration led to deeper penetration into the noncavitated fissure lesions, and thus had greater potential to inhibit caries progression.13 More long-term clinical studies are required to support the use of resin infiltration on occlusal fissure lesions. Another important issue to address is the technique’s long-term color stability when used in proximal and smooth surface lesions.14
 According to Elderton and Mjör,15 cavitated lesions should be restored when:
According to Elderton and Mjör,15 cavitated lesions should be restored when:
- The tooth reacts to stimuli, such as hot, cold and sweetness
- Occlusal and proximal lesion depth deeply penetrates dentin
- Pulp is endangered and the lesion is progressing despite efforts to arrest it
- The patient’s self-care ability is compromised
- Clinicians note the potential for drifting through loss of proximal contact
- The appearance is unesthetic
Regardless of the extent of the cavitation, the outline of the final restoration should follow the three-dimensional shape of the lesion and preserve as much tooth structure as possible.16 This highlights the evolution from the traditional outline forms for caries preparations, which are no longer regarded as appropriate under the MI approach.17
PARADIGM SHIFT FROM REPLACEMENT TO REPAIR
The traditional approach for a failing restoration is to remove and replace it with a new restoration. This treatment modality, however, requires additional tooth structure removal, which may potentially weaken the tooth. In contemporary clinical practice, there has been a significant paradigm shift in the management of recurrent caries. Today, extension, repair or resurfacing of failing restorations is encouraged, as opposed to total restoration replacement.18 The change from replacement to repair is based on the availability of bonding systems and materials that facilitate a defect-specific approach.
The decision-making process on when to replace or repair a restoration should involve comprehensive information that includes caries risk status, professional judgment of benefits versus risks, and the conservative principles of caries preparation.19 Patients need to be informed of the risks and benefits of various treatment approaches, as cooperation is key in successful caries management.
While there are no absolute guidelines for repair, the following criteria/questions should be considered:20
- Is the restoration functionally adequate?
- Are the margins acceptable?
- How significant is the location and extent of the recurrent caries?
- If the tooth is repaired, does this put the tooth at significant risk for fracture or compromise esthetics?
- Will there be proper access and isolation for the repair treatment?
- Is there adequate tooth structure remaining to support the existing restoration and repair?
CONCLUSION
The MI approach can be effectively implemented by educating patients about the importance of recare appointments for reassessment and monitoring of their oral health status. During office visits, dental team members can evaluate caries risk, provide education on self-care techniques, detect caries in the earliest stages, and apply preventive and remineralization agents when indicated. Implementation and further evolution of MI dentistry will benefit both patients and dental professionals, and provide a solid foundation for improving the oral health of future generations.
References
- Dawson AS, Makinson OF. Dental treatment and dental health. Part 2. An alternative philosophy and some new treatment modalities in operative dentistry. Aus Dent J. 1992;37:205–210.
- Christensen GJ. Developing your staff into a patient education team. J Am Dent Assoc. 2009;140:1536–1539.
- Koirala S. Minimally invasive cosmetic dentistry: Concept and treatment protocol. Available at: dentaltribune.com/articles/specialities/cosmetic_dentistry/1749_minimally_invasive_cosmetic_dentistry_concept_and_treatment_protocol.html. Accessed January 7, 2016.
- International Caries Detection and Assessment System. Criteria Manual: ICDAS II. Available at: icdas.org/uploads/ICDAS%20Criteria%20Manual%20Revised%202009_2.pdf. Accessed January 7, 2016.
- American Dental Association. ADA Caries Risk Assessment Form Completion Instructions. Available at: http://www.ada.org/~/media/ADA/Member%20Center/FIles/topics_caries_instructions.ashx. Accessed January 7, 2016.
- American Academy of Pediatric Dentistry. Guideline on Caries-Risk Assessment and Management for Infants, Children, and Adolescent. Council on Clinical Affairs. Available at: aapd.org/media/Policies_Guidelines/G_CariesRiskAssessment.pdf. Accessed January 7, 2016.
- Young DA, Featherstone JD, Roth JR, Anderson M, Autio-Gold J, Christensen GJ. Caries management by risk assessment — implementation guidelines. J Calif Dent Assoc. 2007;35:799–805.
- Weyant RJ, Tracy SL, Anselmo TT, et al. Topical fluoride for caries prevention: executive summary of the updated clinical recommendations and supporting systematic review. J Am Dent Assoc. 2013;144:1279–1291.
- Amaechi BT, Amerongen JP, Loveren C, eds. Fundamentals of Operative Dentistry: A Contemporary Approach. 4th ed. Hanover Park, Illinois: Quintessence; 2013:121–123.
- Kugel G, Arsenault P, Papas A. Treatment modalities for caries management, including a new resin infiltration system. Compend Contin Educ Dent. 2009;30:1–17.
- Altarabulsi MB, Alkilzy M, Petrou MA, Splieth C. Clinical safety, quality and effect of resin infiltration for proximal caries. Eur J Paediatr Dent. 2014;15:39–44.
- Rocha GomesTorres C, Borges AB, Torres LM, Gomes IS, de Oliveira RS. Effect of caries infiltration technique and fluoride therapy on the color masking of white spot lesions. J Dent. 2011;39:202–207.
- Paris S, Lausch J, Selje T, Dörfer CE, Meyer-Lueckel H. Comparison of sealant and infiltrant penetration into pit and fissure caries lesions in vitro. J Dent. 2014;42:432–438.
- Borges A, Caneppele T, Luz M, Pucci C, Torres C. Color stability of resin used for caries infiltration after exposure to different staining solutions. Oper Dent. 2014;39:433–440.
- Elderton RJ, Mjör IA. Treatment planning. In: Hörsted-Bindslev P, Mjör IA, eds. Modern Concepts in Operative Dentistry. Copenhagen, Denmark: Munksgaard; 1988:59–88.
- Walsh LJ, Brostek AM. Minimum intervention dentistry principles and objectives. Aust Dent J. 2013;58:3–16.
- Ricketts DNJ, Pitts NB. Traditional operative treatment options. In: Pitts NB, ed. Detection, Assessment, Diagnosis and Monitoring of Caries, Monographs in Oral Science. Basel, Switzerland: S. Karger AG; 2009; 22:164–173.
- Peters MC, McLean ME. Minimally invasive operative care II. Contemporary techniques and materials: an overview. J Adhes Dent. 2001;3:17–31.
- Tyas MJ, Anusavice KJ, Frencken JE, Mount GJ. Minimal intervention dentistry — a review. FDI Commission Project 1-97. Int Dent J. 2000;50:1–12.
- Ettinger RL. Restoring the aging dentition: repair or replacement? Int Dent J. 1990;40:275–282.

