
 FRANCKREPORTER/E+/GETTY IMAGES PLUS
FRANCKREPORTER/E+/GETTY IMAGES PLUS
Three-Dimensional Imaging in Periodontal Diagnosis, Treatment Planning and Implant Therapy
Bryan J. Frantz, DMD, MS, offers perspective on the use of cone beam computed tomography in dental implant treatment, as well as periodontal diagnosis and care.
Cone beam computed tomography (CBCT) offers three-dimensional (3D) imaging with broad indications for periodontal diagnosis and treatment, as well as all phases of dental implant planning, placement and follow-up. Yet for all of its advantages, cone beam imaging should not be used indiscriminately; rather, it should be considered as a helpful adjunct to traditional examinations, diagnosis, treatment planning and delivery. For insights into this imaging modality, we asked American Academy of Periodontology President-Elect Bryan J. Frantz, DMD, MS, to share his perspective on use of CBCT in periodontal therapy and implant dentistry.
What are the upsides — and limitations — of diagnosing various stages of periodontal disease with CBCT imaging?
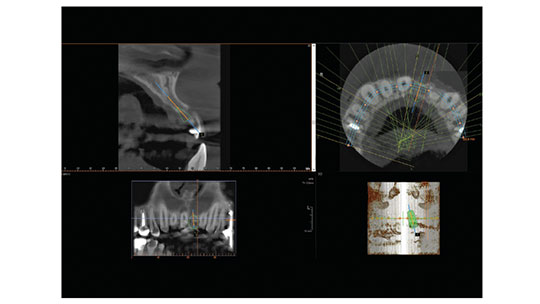
The 3D images provided by CBCT offer useful information that can guide clinical decision-making, periodontal diagnosis, treatment planning and surgical execution (Figure 1). When it comes to diagnosing and managing periodontal diseases, CBCT may be a useful adjunct in certain cases to two-dimensional imaging and clinical probing. Additional periodontal benefits may involve assessing furcation areas or intrabony lesions to help determine treatment potential and prognosis. It is also a useful adjunct in patients requiring orthodontic-periodontic interdisciplinary care.
That said, this imaging modality should be considered an adjunctive diagnostic method after a comprehensive periodontal examination is performed. Limitations to the technology include equipment and software variations that impede the standardization of outcome measures. As indicated by the American Academy of Periodontology’s Best Evidence Consensus panel on CBCT, areas for investigation include accurately quantifying bone density and changes in linear remodeling, minimizing radiation exposure, and optimizing the image resolution through the reduction of radiation artifacts, beam hardening and scatter. As is the case with most emerging technologies, the body of knowledge is evolving, and solutions are likely on the horizon.
Has CBCT become today’s standard of care in implant dentistry? And what are the potential ramifications of not using 3D imaging in implant therapy?
Yes, CBCT imaging improves the current standard of care by providing key information, such as measurement of the density, height and buccolingual width of the alveolar bone at any jaw location, as well as visualization of the pathology, inclination of the bone, and vital anatomic structures. It also aids evaluation of root morphology and pathology at extraction sites.
Using special software, data generated with CBCT imaging during implant planning can be used to fabricate 3D surgical guides. Implants are placed with higher accuracy using these 3D surgical guides. The guides can also be used to generate retro-engineered casts that enable the prefabrication of restorations prior to implant surgery. These restorations can be precisely engineered to improve prosthetic outcomes and delivered to the patient on the day of the operation. Using all available virtual tools, true restoratively driven implant dentistry can be accomplished via image-guided surgery, benefiting both the patient and dental surgeon. The success and survival of dental implants and implant restorations depend on a thorough diagnosis and careful treatment planning. Not using this imaging modality may increase surgical and prosthetic complications.
Please discuss field of view (FOV), and which practice settings would most benefit from regional versus full-scan machines.
Large FOV images are needed by periodontists, orthodontists, oral and maxillofacial surgeons, and prosthodontists for advanced reconstruction with dental implants. However, for most other situations, especially endodontics, a more restricted FOV is suitable. Smaller FOV images are more affordable and decrease the patient’s radiation exposure. In addition, small FOV images preclude the need for an expert opinion when the tissues imaged are restricted to dental structures.
What is scatter, and what are its clinical implications?
Considered one of the key limitations of CBCT image quality, scatter is the phenomenon whereby photons are diverted from their original path by interaction with matter. The clinical implications are that it results in increased measured intensities on CBCT radiographs; it also causes streaks and other artifacts that can reduce soft tissue contrast and affect the appearance of the general density of tissues.1
The literature has offered many correction algorithms for scatter, but there is not yet a practical standard approach to reducing this phenomenon.
Please explain “stitching” and its advantages in periodontal diagnosis and treatment planning.
Three-dimensional stitching is a new 3D acquisition mode that automatically combines two or three small FOV volumes to construct a larger, composite 3D image that is needed for a wider region of examination (e.g., 80×37 mm). The benefits of the 3D stitching mode include a broader range of applications, affordability, flexibility, optimizing the radiation dose for patient safety, and improved workflow. Based on current evidence, stitched composite 3D imaging appears to be accurate and reliable for diagnostic purposes.
In periodontal and implantology settings, who reviews the CBCT scan? Is this best done by a radiologist? What are the medicolegal issues in reading the scan?
Clinically, it is at the clinician’s discretion to determine if he or she is comfortable reading CBCT scans. The scan needs a formal radiographic interpretation of all areas scanned — including any abnormalities seen — and many clinicians are trained to interpret the scans successfully. However, dental radiologists and CBCT specialists are comprehensively trained to administer and interpret the scans. When it comes to mitigating legal risks, it may be advisable in certain cases for a dental radiologist to read and report on the scan.
From a practice management standpoint, what are the practical considerations in terms of training?
Unit manufacturers provide training and support. In addition, a number of continuing education courses offer training in this imaging modality and cover the basic functions of CBCT, its risks and benefits, the appearance of disease and anatomic variations, and interpretation — as well as legal and ethical issues. Time commitments and costs vary based on the nature of the course. While these types of courses may not provide the level of competency achieved by a radiologist or CBCT specialist, they offer guidance to all practitioners in the safe use of 3D imaging.
Any final thoughts?
In the last two decades, CBCT has proven a beneficial tool in diagnosis and successful treatment of various stages of periodontal disease. With proper use and application, 3D imaging can lead to predictable outcomes in particularly complex cases. It also fosters collaboration, as it provides a detailed communication tool for use with patients and dental/medical colleagues. Further research will help solidify its position in the future of periodontal care and implant dentistry.
KEY TAKEAWAYS
- In periodontal therapy and implant treatment, the three-dimensional (3D) images provided by cone beam computed tomography (CBCT) can guide clinical decision-making, diagnosis, case planning and surgical execution.
- For implant cases, CBCT imaging improves the current standard of care by providing key information, such as measurement of the density, height and buccolingual width of the alveolar bone at any jaw location, as well as visualization of the pathology, inclination of the bone, and vital anatomic structures.
- This imaging modality should be considered an adjunctive diagnostic method after a comprehensive examination is performed.
- In CBCT imaging, the scatter phenomenon results in increased measured intensities on the scans; it also causes streaks and other artifacts that can reduce soft tissue contrast and affect the appearance of the general density of tissues.1
- It is at the clinician’s discretion to determine if he or she is comfortable reading CBCT scans. The scan needs a formal radiographic interpretation of all areas scanned — including any abnormalities seen.
REFERENCE
- Schulze R, Heil U, Gross D, et al. Artefacts in CBCT: a review. Dentomaxillofac Radiol. 2011;40:265–273.
The author has no commercial conflicts of interest to disclose.
From Decisions in Dentistry. September 2019;5(8):48—50.
