
 THELINKE / ISTOCK / GETTY IMAGES PLUS
THELINKE / ISTOCK / GETTY IMAGES PLUS
Three-Dimensional Imaging in Periodontal and Implant Therapy
Douglas W. Beals, DDS, MS, of Midwestern University College of Dental Medicine in Glendale, Arizona, presents an overview of the utility of cone beam computed tomography in periodontal treatment and dental implant therapy.
Dental applications for three-dimensional (3D) cone beam computed tomography (CBCT) are numerous and include periodontal care and implant therapy, where 3D scans can serve as adjuncts that support successful long-term outcomes. But, like any imaging modality, CBCT is not indicated for every patient and case. For perspective on how cone beam scanning fits into periodontics and implantology, we asked oral and maxillofacial surgeon Douglas W. Beals, DDS, MS, of Midwestern University College of Dental Medicine in Glendale, Arizona, for his views on this versatile and popular imaging technology.
When should CBCT be utilized for diagnosing periodontal disease?
The American Academy of Periodontology (AAP) published a best evidence consensus on CBCT in 2017. This was an effort to seek out the best available publications and expert commentaries on the use of CBCT in periodontics. The consensus stated, “For patients with periodontitis, two-dimensional (2D) full-mouth radiographs combined with clinical probing remain the gold standard; however, CBCT may be beneficial in certain advanced cases.” The AAP recognized that cone beam imaging has a limited role in diagnosing periodontal disease, but should be reserved for advanced cases where traditional 2D films and clinical probing will not suffice.
Does CBCT represent today’s standard of care when planning and placing dental implants? What are the advantages of using this imaging modality in treatment planning?
Without doubt, CBCT is the most state-of-the-art modality available to treatment plan for dental implants. The question is whether it is required to properly plan implant placement. The answer is equivocal — and so opinions vary. In 2000, the American Association of Oral and Maxillofacial Radiology (AAOMR) published a position paper regarding the role of radiographic imaging in the treatment planning phase of dental implant surgery. The paper stated, “After reviewing the current literature, the AAOMR recommends that some form of cross-sectional imaging be used for implant cases, and that conventional cross-sectional tomography is the method of choice for gaining this information for most patients receiving implants.”
Since the AAOMR paper was published before cone beam imaging was in widespread use, medical-grade tomography was recommended. In today’s practice, the relative cost to purchase a CBCT unit — as well as the lower dose of radiation compared to medical-grade computed tomography — has made the use of CBCT attractive for implant planning. Utilizing CBCT cross sectional images allows practitioners to evaluate the potential implant site in three dimensions. Such 3D imaging provides the opportunity to evaluate the quality, quantity and morphology of the bone making up the residual ridge.
Applying the philosophy of “restoratively driven implant planning” is the recommended approach to this initial phase of therapy. The utilization of CBCT in conjunction with specialized software is the most reliable and predictable way to plan treatment. The need for lateral or vertical ridge augmentation to facilitate proper implant placement can be diagnosed and planned most accurately using this modality. Practitioners will more easily and accurately identify important anatomical structures in and around potential implant sites and therefore avoid iatrogenic events.
In short, while the advantages are clear, organizations to this point have not yet claimed CBCT as the standard of care for dental implant planning.
When considering the purchase of a CBCT unit, how does a dentist decide on the appropriate machine?
There are many variables to consider when evaluating the purchase of a CBCT unit. For starters, clinicians should consider their primary planned use. Applications for cone beam scanning are numerous, and key examples include:
- Implant planning
- Diagnosing and treating pathology
- Endodontics
- Extractions
- Precisely locating impacted teeth
- Identifying vital structures
- Temporomandibular joint disease diagnosis and treatment
- Managing bone defects
- Peri-implant disease diagnosis and management
- Evaluating the airway for potential sleep apnea patients
Each of these uses may require a different field of view (FOV).
Because of this, practitioners should strongly consider units that will best serve their purposes. For example, in endodontics, a limited FOV should suffice, while in oral surgery or implantology a large FOV may be necessary. There are many versions of CBCT machines and the footprints vary; thus, the size of the footprint must be considered based on the space it will occupy in the office. Also, the larger the FOV, the more expensive the machine. When a practitioner is planning any type of surgery, whether it involves implants, periodontal bone regeneration, or extraction of impacted teeth, more information is always better. Cross-sectional 3D imaging simply provides more information — depending on the individual office, the investment may be worth it.
What are some additional considerations for CBCT use in implantology?
Often, CBCT machines are offered with proprietary implant planning software that is included or available for purchase. Obviously, each company would like dentists to purchase this proprietary software, but that’s a decision the clinician will have to make. For example, providers should consider if they will design and fabricate surgical guides as part of the implant planning process. If so, third-party software may be required to facilitate the design and/or fabrication of surgical guides in-house or by a laboratory.
Would any of these parameters change if the machine was intended only for periodontal care (meaning, therapy not involving implant placement)?
Many of these same considerations apply for strictly periodontal care. For example, most clinicians continue to rely on 2D films for diagnosing and treating periodontal disease. While the use of cone beam imaging to evaluate the need for periodontal grafting — and in planning for grafting procedures — is certainly useful, it is not absolutely necessary.

When should CBCT be used in planning and executing tooth extractions?
The use of cone beam imaging to plan and execute tooth removal has become popular among exodontists. The 3D assessment of the tooth in question is invaluable, as it is often positioned adjacent to vital structures. Typical scenarios include impacted third molars adjacent to the inferior alveolar nerve, an impacted maxillary canine against an adjacent tooth root, or a diseased maxillary molar that involves the maxillary sinus. There are other indications, of course, but these are perhaps the most common. By analyzing the information provided via 3D imaging, the practitioner can determine the most predictable course of treatment. In clinical terms, this helps minimize complications and supports better outcomes.
Please discuss the issue of artifacts.
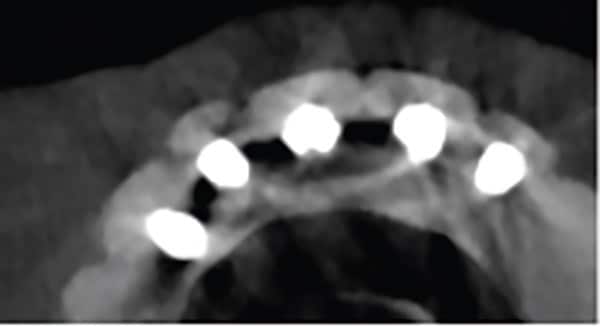
Three types of artifacts are commonly encountered in cone beam imaging. These are beam hardening, motion-related, and streak (or scatter) artifacts. Beam hardening occurs in two forms: dark bands or cupping. This phenomenon stems from the difference in density of bone and metal, which results in varying absorption of low and high-energy photons. In turn, this compromises image quality and creates difficulty in evaluating peri-implant bone levels and health due to the opaque nature of this artifact (Figure 1). For this reason, conventional 2D imaging, such as a vertical bitewing, may more accurately depict peri-implant bone.
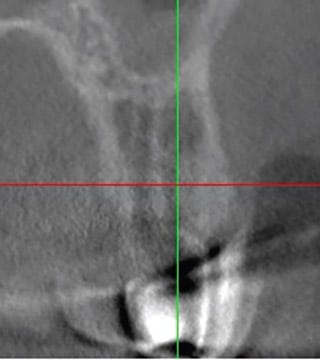
Motion-related artifacts are caused by patient movement. The resulting image appears blurred, or with lines doubled (Figure 2). This yields nondiagnostic images that can render inaccurate depiction of implants, teeth, local anatomy, or clinical measurements. If the treating doctor is not aware of this artifact and the ramifications, it can lead to surgical mistakes resulting in damage to adjacent structures or inaccurately placed implants. Sit-down machines may decrease the incidence of this artifact.
Streak or scatter artifacts (Figure 3) are a result of X-rays encountering a metallic object. When the X-rays strike the metal object, they are deflected away from it. This artifact appears as dark or light lines emanating from the metallic object. These lines produce an image of poor quality and may also obscure structures. Because this artifact cannot always be avoided, traditional 2D films may be considered as an adjunct when indicated.
How do CBCT calibration issues affect clinical practice for periodontists and implantologists?
All CBCT machines require regular maintenance, including calibration. Lack of regular calibration or technical errors that prevent correct calibration will lead to inaccurate imaging. This may result in errors in either implant planning parameters, measurements of vital structures, or identifying local anatomy. Practitioners should adhere to all manufacturer recommendations regarding calibration.
Who reviews the CBCT scan? In periodontal and implantology settings, is this best done by a radiologist? Are there medicolegal issues to consider?
When a dentist makes the decision to purchase a CBCT machine and acquire images in-house, this automatically raises medicolegal considerations. The provider who acquires the imaging is responsible for reading (interpreting) that imaging. This liability can be shared to an extent if the imaging is read by an oral and maxillofacial radiologist. The radiologist should generate a report chronicling his or her findings and recommendations.
Any practitioner who utilizes CBCT in conjunction with specialized software to plan implant surgery should be knowledgeable in reading the acquired images. Incidental findings are common in CBCT scans that are obtained for implant planning. Reducing the size of the FOV does not diminish the need to identify incidental findings during review of the imaging. A recent paper showed that of 474 limited FOV scans obtained for the purpose of implant planning, 51.5% had at least one incidental finding. Most of these findings (70.5%) were referred for evaluation and/or treatment.1
Incidental findings vary in number and type based on the size of the FOV. Practitioners should not make the mistake of thinking that a limited (i.e., small) FOV translates into less medicolegal risk.1 Practitioners should strongly consider having an oral and maxillofacial radiologist read and report on cone beam imaging acquired with in-office equipment. They should also check with their malpractice carriers, as some require a rider to cover the potential liability of acquiring CBCT images in-house.
Before purchasing a CBCT unit, clinician can utilize 3D radiography via imaging centers or by partnering with offices that have the equipment. Briefly, what are the advantages and disadvantages of this approach?
The most cost-effective way to obtain CBCT scans is to send patients to an imaging center or another practitioner who will acquire the imaging. The referring practitioner does not have to invest in costly equipment or be concerned about additional liability or billing for the service. The disadvantages of outsourcing are delays in diagnosis and treatment, constraints during implant planning, and limitations in viewing the scan.
Most oral health professionals who have CBCT machines and acquire scans daily or weekly are accustomed to reviewing them in real time. This allows for more immediate feedback to the patient and facilitates more efficient diagnosis and treatment. Similarly, using integrated in-office software allows providers to plan implant treatment for any case supported by the unit’s FOV. In turn, this contributes to the quality of care and leads to better outcomes.
In all, clinicians have multiple options for evaluating the utility of cone beam imaging in their practice before committing to a major purchase. Ultimately, this assessment may be the difference-maker when considering the addition of in-house CBCT technology.
Reference
- Johnson S, Fluckiger J, Parashar V, Beals D, Agostini G. Frequency and types of incidental findings on limited field of view CBCT scans. Gen Dent. 2021;69:42–45.
From Decisions in Dentistry. September 2022;8(9)17-19.
