

Surgical Risk Assessment for Dental Implants
Through use of objective criteria, clinicians can improve outcomes by effectively assessing patients and specific sites for implant placement.
Through use of objective criteria, clinicians can improve outcomes by effectively assessing patients and specific sites for implant placement
The dental implant surgeon has many factors to consider when deciding on the candidacy of a patient and particular site for implant placement. Successful outcomes depend on placement that leads to integration, restoration and function — with stable hard and soft tissue for acceptable esthetics. While numerous clinical factors are involved in this process, the aim of this article is to identify factors having the greatest impact on the surgical process, with the goal of forecasting a reasonably predictable outcome given the site’s specific characteristics.
By creating what we propose as an Implant Placement Risk Assessment Score (IPRAS), an objective set of criteria can be established to aid clinicians in appropriate surgical protocols for implant placement. The risk assessment scale is meant to prognosticate the outcomes of implant placement without adjuncts, such as hard- or soft-tissue grafts, the use of membranes, and/or ridge reconstruction. Based on the score, the provider may decide to add additional treatment modalities to ensure success in medium- and high-risk cases. In cases beyond their skill set, clinicians may also elect to refer the patient to an appropriate provider with advanced skills.
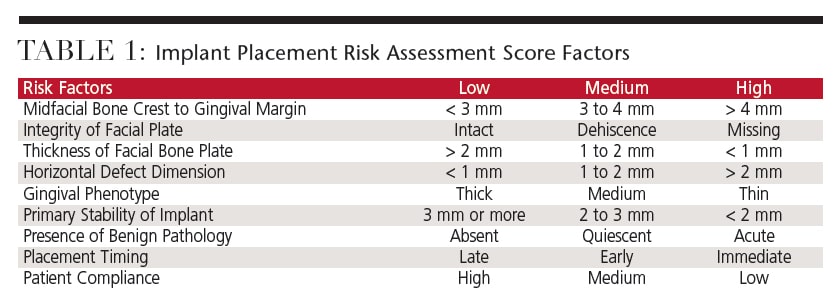 The risk factors included in the IPRAS are based on clinical experience and discussion among implant clinicians worldwide. The criteria within each category are derived from evidence in the literature and are used to create a profile for individual implant sites. Each factor is stratified into low, medium or high risk, and the individual factors are combined to provide a cumulative risk score (Table 1). Lower risk scores denote more predictable results, and higher likelihood of overall success. Conversely, higher risk scores denote less predictable results, and lower likelihood of overall success without additional interventions to the implant site.
The risk factors included in the IPRAS are based on clinical experience and discussion among implant clinicians worldwide. The criteria within each category are derived from evidence in the literature and are used to create a profile for individual implant sites. Each factor is stratified into low, medium or high risk, and the individual factors are combined to provide a cumulative risk score (Table 1). Lower risk scores denote more predictable results, and higher likelihood of overall success. Conversely, higher risk scores denote less predictable results, and lower likelihood of overall success without additional interventions to the implant site.
FACIAL BONE PLATE CHARACTERISTICS
The first three factors to consider when evaluating an implant site are all characteristics of the facial bone plate. Deficiency in any of these factors may lead to stratification into the medium- and high-risk categories. Clinically, these deficiencies indicate a lack of adequate bony housing and may lead to rapid bone loss, tissue recession, exposure of the facial surface of the implant, esthetic concerns — and even implant failure.
Midfacial Bone Crest to Gingival Margin: The depth of implant placement is important to ensuring sufficient space for the formation of adequate emergence profile and biologic width for maintenance of a healthy gingival sulcus around the implant. Crestal bone level should be examined at the time of implant placement to ensure the gingival margin will be at the desired level once implant integration and mucosal maturation are complete. Implants placed at the proper depth, and with midfacial bone crest correctly positioned in relation to the implant abutment interface, will experience less recession than if incorrectly positioned. In turn, this eliminates thread exposure and helps ensure an esthetic gingival margin and crown contour.

The implant sulcus varies with thickness of gingival tissue and is dependent on the patient’s gingival phenotype. Implant sulcus thickness is defined as ≤ 2 mm in thin-gingival biotypes, 2.1 to 3 mm in medium-tissue biotypes, and > 3.1 mm in thick-tissue phenotypes.1,2 Lee et al1 report that peri-implant mucosa typically measures < 3 mm in a thin-tissue phenotype, compared with > 4 mm in a thick-tissue phenotype. Palaska et al3 examined 105 implants placed in humans in a prospective, blind, randomized clinical trial examining placement depth and bone remodeling. While bone loss increased with sub-crestal implant placement, the connection pattern between implant/abutment proved significant: less bone loss was observed with morse taper, and more with screw channel connections. This article effectively summarized the work of multiple authors, who found that first bone to implant contact is 0.9 to 2.25 mm apical to the implant abutment interface with sub-crestal implant placement. With increased bone contact depth in relation to the abutment interface, gingival sulcus depth and marginal gingiva predictability decreases, and risk for peri-implant inflammation increases. In sites with greater facial bone crest to gingival margin depths, clinicians may decide to perform bone augmentation procedures prior to, or at time of, implant placement to reconstruct the facial bone to a more ideal position.
The findings discussed above lead to the stratification of midfacial bone crest to gingival margin as low risk if < 3 mm, medium risk if 3 to 4 mm, and high risk if > 4 mm (Figure 1).
Integrity of Facial Bone Plate: Many studies and reviews endorse that facial plate dehiscence compromises predictable bony support for the implant.1,4–8 In a 2004 literature review, Chen et al7 note that sockets with dehiscence defects may lack the potential for complete bone regeneration, and the risk of long-term complications may increase with immediate implant placement at these sites. Bone augmentation procedures may be necessary to regenerate the facial bone plate and can be expected to achieve some degree of predictability. With the introduction of additional products and predictable procedures for bone reconstruction, a more ideal ridge form can be achieved. Predictability of the reconstructed ridge form, however, is reduced compared with implant integration into healthy, native bone. Kan et al9 studied 23 implants with immediate implant placement and guided bone regeneration in sites with facial bone defects > 3 mm. It was demonstrated that larger defects resulted in more gingival recession. One year after immediate tooth replacement and guided bone regeneration, one of 12 (8.3%) V-shaped, three of seven (42.8%) U-shaped, and four of four (100%) ultra-U-shaped defects resulted in > 1.5 mm of facial gingival recession.
In a prospective study of 56 sites, Chen et al6 found that labial plate damage resulted in significant resorption, irrespective of whether a membrane and/or bone graft was used. They advocated slower resorbing adjuncts in these cases. The literature demonstrates that dehisced bone has the potential to regenerate, but also shows a propensity to bone loss. Missing facial bone presents a greater risk for failure at the time of placement. Although guided bone regeneration may help rebuild the facial plate at the time of implant placement, it was not specifically investigated in this review, and would be considered an adjunct for possible use in highrisk patients.
Bone plate integrity is stratified as low risk if the facial plate is completely intact, medium risk for dehiscence-type defects, and high risk when the facial plate is missing.
Thickness of Facial Bone Plate: In terms of predictable success, if the facial bone plate is of the proper height and integrity, the final structural consideration is the thickness of the bony wall. There is a significant volume of data on this factor. Braut et al10 performed a radiographic study using cone beam computed tomography to evaluate facial plate thickness of teeth in the anterior maxilla. Of the 125 scans performed, 90.0% of patients either had missing or thin (< 1 mm) facial bone in the crestal area of teeth in the anterior maxilla. In a study of nonsubmerged immediate implant sites, Chen et al6 note that sites that healed with complete bone fill or a residual crater-like defect had an initial thickness of the facial bone of 0.7 to 0.9 mm, and recorded vertical loss of crestal bone height of 0.3 to 0.9 mm at reentry. In contrast, sites that healed with a dehiscence defect initially had a facial bone thickness of 0.5 mm, and recorded vertical crestal bone loss of 2.1 mm at reentry. Thus, extraction sockets with thin facial bone lost more vertical height and had less bone fill than sites with thicker bone.
Examining 93 immediate implants, Ferrus et al11 note that 71% of sites with a thin (< 1 mm) buccal ridge experienced significant (> 20%) bone plate resorption during healing. Tomasi et al12 performed a randomized, controlled clinical trial of 93 implants in immediate extraction sites, and found that sites with thick (> 1 mm) bony walls showed more bone fill than sites with a thin (1 mm) alveolar crest. Buccal and palatal bone fill appear to depend on the thickness of the alveolar crest. Spray et al8 examined 3061 implants for facial plate thickness, noting the largest bone loss was evident when facial bone thickness at implant placement ranged from < 1 to 1.4 mm. Decreased bone loss was noted with plate thickness of 1.4 to 1.7 mm, and no change or bone increase was seen with facial plate thickness > 1.8 mm. The study concluded that 2 mm was the critical thickness to bone survival and increased predictability in regard to buccal plate thickness at the implant site.
Using incandescent and fluorescent light microscopy in 12 dog subjects, Qahash et al13 evaluated the strength of the association between buccal alveolar ridge width and extent of bone resorption. The investigation demonstrated mean buccal resorption was significantly greater when ridge width was < 2 mm. In a sample of 12 immediate implants with guided bone regeneration, Matarasso et al14 found the residual combined thickness of the buccal wall with the newly formed periimplant bone at sites with an initial thickness of 1 mm was statistically significantly smaller (P < 0.05) compared with sites with an initial buccal thickness of 2 mm (2.50 +/- 0.76 versus 4 +/- 0 mm).
With significant evidence behind this factor, facial bone thickness is stratified into low risk if the buccal plate thickness is > 2 mm, medium risk for plate thickness of 1 to 2 mm, and high risk if plate thickness is < 1 mm.
HORIZONTAL DEFECT DIMENSION
Horizontal defect dimension (HDD) refers to the gap between the facial implant surface and internal surface of the facial bone socket wall. The HDD is 0 for implants placed in healed sites, which generally serve as the control in most studies. Paolantonio et al15 observed 96 mini-implants for alveolar anatomy changes. Half of the implants were placed into extraction sockets with HDDs ≤ 2 mm, while the other half were placed into mature bone and served as controls. No membranes or grafts were used, and primary soft tissue closure was performed. Examination of the test implants following surgical reentry at six months showed complete bone fill of the previous defects. Based on literature reviews, Chen et al5,7 report that HDDs ≤ 2 mm will spontaneously heal, and that osseointegration will be successful. However, HDDs > 2 mm were shown to heal unpredictably, although outcomes might be enhanced with use of membranes and bone grafts.
Wilson et al16 performed a study involving histological examination of immediate implants in humans and found predictable bone fill with HDDs of < 1.5 mm without membrane placement. A case series by Wilson et al17 reporting on biopsies of seven implants with HDDs > 4 mm at time of placement, covered with connective tissue membrane and primary closure, found bone-to-implant contact (BIC) similar in the implants with > 4 mm gaps to those with gaps of 0 to 1.5 mm. The study size was small and it remains undetermined whether different types of membrane, placement of the membrane, type of implant surface, or a combination of these factors were responsible for the improved osseointegration in HDDs > 4 mm. Botticelli et al18 followed 52 sites with HDDs > 3 mm on 21 implants after immediate implant placement. Reentry surgery was performed at four months. Following flap elevation, eight defects with HDDs > 3 mm remained, 25% of the sites with initial HDDs of 2 to 3 mm healed completely, as well as 78% of the sites with initial gaps of less than 2 mm. Schropp et al19 observed that only 52% of sites with an initial HDD of 4 to 5 mm healed spontaneously in the presence of intact bone walls. While integration and bone fill can be seen in sites with larger HDDs, the bulk of evidence points to a smaller gap as yielding more predictable results.
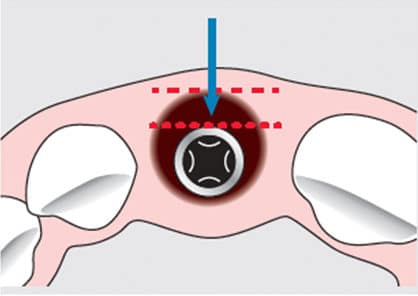
In summation, an HDD is considered low risk when < 1 mm, medium risk when 1 to 2 mm, and high risk when > 2 mm (Figure 2, page 16).
GINGIVAL PHENOTYPE
In terms of implant function, peri-implant soft tissue rivals bone because gingival health and contours around the implant are not only important for esthetics, they also contribute to long-term success. Durable, healthy tissue is necessary to resist frictional forces in the mouth and recession and, thus, preserve underlying bone around the implant. Although gingival phenotype is innate to an individual, it can be altered with grafting techniques. Linkevicius et al2 showed high correlation between crestal labial soft-tissue thickness of anterior maxillary implants and the thickness of the underlying bone. Though not found to be statistically significant, Kan et al9 reported that > 1.5 mm recession occurred in 30% of implants with a thick phenotype, and 38.5% with thin phenotypes.



Stratifying by tissue phenotype and presence of a graft, Puisys and Linkevicius20 examined 97 bone level implants for bone loss at 12 months. Significantly less bone loss (0.65 mm) was seen in sites with a thick phenotype compared to those with a thin phenotype (0.75 mm). In a literature review, Chen et al7 note that in immediate implant placement, sites with a thin-tissue phenotype had a higher incidence of recession, reportedly > 1 mm compared to sites with a thick-tissue phenotype. Jung et al21 examined pig maxillae for gingival thickness as it pertains to implant materials and their visibility through tissue. Gingival thickness of 3 mm was found to be optimal to provide coverage over the implant’s metal collar so it was indistinguishable to the eye. Chappius et al22 studied gingival alterations after tooth extraction and found that a thin-gingival phenotype in post ex traction sites showed spontaneous gingival thickening, but more bone resorption.
Considering the data, the authors of this paper stratify a thick-gingival phenotype as low risk for implant placement, medium phenotype as medium risk, and thin phenotype as high risk (Figures 3A through 3C).
NATIVE BONE FOR PRIMARY STABILITY
Primary stability is necessary to ensure the implant has a minimum amount of native bone to stabilize the implant for successful osseointegration and function. The amount of bone needed to achieve primary stability is still poorly defined, however, and most clinicians use their own visual and digital standards for determining primary stability. Quite simply, if the implant does not move when touched, it is considered to have primary stability. Although scant, there is some literature to help determine the bone requirements for primary stability. Pommer et al23 found no difference in stability between residual bone heights of 2, 4 and 6 mm. Implant diameter was also not found to be significant. Bone density was reported to be a determining factor for primary stability in maxillary molar implants placed in atrophic sinuses with simultaneous sinus augmentation. With simulated bone, Hsu et al24 found an increase in stability as the height of cortical bone and density of trabecular bone increased from 0 to 3 mm, and from 0.12 to 0.32 g/cm3, respectively. A decrease in the three-dimensional BIC ratio was associated with decreases in peri-implant bone strain and primary implant stability. In addition, there was a strong linear correlation between cortical BIC and primary implant stability (R2 > 0.8). Becker and Becker,25 along with Werbitt and Goldberg,26 cited 3 mm as the minimum bone required for primary stability in immediate extraction sites.
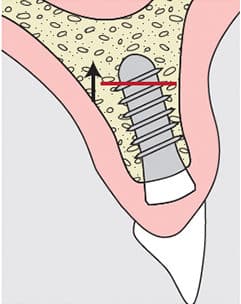
From the data, available residual bone height for primary stability is considered low risk if > 3 mm, medium risk with 2 to 3 mm residual bone height, and high risk with residual bone height < 2 mm (Figure 4).
PRESENCE OF BENIGN PATHOLOGY
Pathology around an implant site may affect apical bone for primary stability or crestal bone in the form of periodontal defects. If malignancy or an aggressive benign lesion is suspected, further investigation is needed prior to implant placement. If risk is considered, implant planning and placement can proceed in areas with the presence of benign pathology. In literature reviews by Chen et al,5,7 numerous sources attribute implant failures to periodontal disease. A higher failure rate is also reported in sites with active periodontitis, irrespective of the timing of placement after extraction. Comparing patients with periodontal disease to healthy subjects, a retrospective analysis by Evian et al27 of 149 consecutive single implants placed showed implant survival rates of 79.22% and 91.57%, respectively, over a mean observational period of 943 days. No significant difference was noted between immediate and delayed placement of the implants. The limitations of this study should be noted, however, including simultaneous periodontal procedures performed at the time of implant placement. In addition, routine follow-up and maintenance were not performed by the surgeon but, rather, by the restorative dentist.

Siegenthaler et al28 conducted a prospective, controlled clinical trial in 32 subjects that examined immediate implant placement in sites with periapical pathology. Immediate implant placement was compared in 17 sites with apical pathology, and 17 sites without apical pathology. Five sites (four with apical pathology and one without) were withdrawn due to lack of initial implant stability. After 12 months, the survival rate for both groups was 100%. In a follow-up study by the same group, after five years all implants were found to be osseointegrated, with good tissue and radiographic parameters.29 Considering the studies and sample sizes evaluating implants placed in sites with periapical pathology is limited, any conclusions should be drawn with caution.
Based on the above discussion, sites without benign pathology are stratified as low risk, sites which chronic pathology (such as periodontal disease) as medium risk, and sites with acute benign pathology as high risk for implant placement (Figure 5).
PATIENT COMPLIANCE
Causes of implant failure are both site specific and patient modified. Manor et al30 cite primary predictors of implant failure as poor bone quality, chronic periodontitis, systemic diseases, smoking, advanced age, implant location, parafunctional habits, loss of implant integration, and inappropriate prostheses. While some of these predictors are site specific, many are patient-modifiable and thus would affect any implant site in a given patient. A site deemed as low risk (according to the factors discussed above) can experience implant failure if patient compliance is poor, or by introducing patient-modifiable factors, such as smoking, bruxing or neglecting systemic health. Prior to implant placement, instructions regarding dietary restrictions, hygiene, proper prosthesis use (or restricted use), and splint therapy (if indicated) should be thoroughly discussed with patients. The clinician should ascertain patients’ likely level of cooperation and motivation to proceed through the surgical phase of implant therapy. Patients should also be counseled about maintenance of chronic health conditions, and smoking cessation, if applicable. Additionally, the postoperative observation schedule should be clearly outlined to ensure patient follow-up with the clinician. A provider may rule out a patient as a candidate if geographic and transportation factors are limiting, or if a psychological disorder may lead to sporadic compliance.
The authors stratify the compliance factor as low risk if the patient is cooperative and motivated, medium if there are minor patient compliance variables, and high risk if the patient is complacent and not motivated to follow instructions and restrictions.
RISK SCORING AND SUMMARY
After each risk factor is considered and critically assessed, an overall value can be determined for a potential implant site. If a numerical value is assigned to each category in the risk assessment scale, with one for low, two for medium, and three for high, a numerical value of overall risk can calculated. Sites with ≤ 10 points are stratified as low risk, 11 to 18 points as medium risk, and ≥ 19 points as high risk. Low-risk sites generally offer a reasonably predictable likelihood of integration, restoration, function, stable hard and soft tissue housing, and acceptable esthetics. Medium-risk sites pose challenges that may warrant modification through adjuncts, such as guided bone regeneration or soft-tissue grafting. High-risk sites may either be eliminated as potential candidates for implant placement, or considered for more advanced reconstruction planning. Risk scores in individual categories will determine the potential need for further adjunctive surgical intervention.
In conclusion, a patient’s overall IPRAS helps clinicians determine the likelihood of successful implant therapy. It may also serve as a threshold for referral to a specialist with advanced surgical skills. In addition, the IPRAS provides a powerful tool to share with the patient at the treatment plan presentation, and to help establish realistic expectations when discussing expected outcomes.
KEY TAKEAWAYS
- Successful implant outcomes depend on placement that leads to integration, restoration and function — with stable hard and soft tissue for acceptable esthetics.
- This article proposes an Implant Placement Risk Assessment Score (IPRAS) based on objective criteria that can aid clinicians in determining a patient’s suitability for implant placement.
- The criteria within each scoring category are derived from evidence in the literature and can be used to create a profile for individual implant sites.
- Besides offering a powerful treatment-planning tool, the IPRAS can be shared with patients to establish realistic expectations when discussing expected outcomes.
REFERENCES
- Lee A, Fu JH, Wang HL. Soft tissue biotype affects implant success. Implant Dent. 2011;20:e38–e47.
- Linkevicius T, Apse P, Grybauskas S, Puisys A. The influence of soft tissue thickness on crestal bone changes around implants: a 1-year prospective controlled clinical trial. Int J Oral Maxillofac Implants. 2009;24:712–719.
- Palaska I, Tsaousoglou P, Vouros I, Konstantinidis A, Menexes G. Influence of placement depth and abutment connection pattern on bone remodeling around 1-stage implants: a prospective randomized controlled clinical trial. Clin Oral Implants Res. 2016;27:e47–e56.
- Block M, Kent J. Factors associated with soft- and hard-tissue compromise of endosseous implants. J Oral Maxillofac Surg. 1990;48:1153–1160.
- Chen ST, Buser D. Clinical and esthetic outcomes of implants placed in postextraction sites. Int J Oral Maxillofac Implants. 2009;24(Suppl):186–217.
- Chen ST, Darby IB, Adams GG, Reynolds EC. A prospective clinical study of bone augmentation techniques at immediate implants. Clin Oral Implants Res. 2005;16:176–184.
- Chen ST, Wilson TG Jr, Hämmerle CH. Immediate or early placement of implants following tooth extraction: review of biologic basis, clinical procedures, and outcomes. Int J Oral Maxillofac Implants. 2004;19(Suppl):12–25.
- Spray JR, Black CG, Morris HF, Ochi S. The influence of bone thickness on facial marginal bone response: stage 1 placement through stage 2 uncovering. Ann Periodontol. 2000;5:119–128.
- Kan JY, Rungcharassaeng K, Sclar A, Lozada JL. Effects of the facial osseous defect morphology on gingival dynamics after immediate tooth replacement and guided bone regeneration: 1-year results. J Oral Maxillofacial Surg. 2007;65(Suppl 1):13–19.
- Braut V, Bornstein MM, Belser U, Buser D. Thickness of the anterior maxillary facial bone wall-a retrospective radiographic study using cone beam computed tomography. Int J Periodontics Restorative Dent. 2011;31:125–131.
- Ferrus J, Cecchinato D, Pjetursson EB, Lang NP, Sanz M, Lindhe J. Factors influencing ridge alterations following immediate implant placement into extraction sockets. Clin Oral Implants Res. 2010;21:22–29.
- Tomasi C, Sanz M, Lindhe J, et al. Bone dimensional variations at implants placed in fresh extraction sockets: a multilevel multivariate analysis. Clin Oral Implants Res. 2010;21:30–36.
- Qahash M, Susin C, Polimeni G, Hall J, Wikesjö U. Bone healing dynamics at buccal periimplant sites. Clin Oral Implants Res. 2008;19:166–172.
- Matarasso S, Salvi GE, Iorio Siciliano V, Cafiero C, Blasi A, Lang NP. Dimensional ridge alterations following immediate implant placement in molar extraction sites: a six-month prospective cohort study with surgical re-entry. Clin Oral Implants Res. 2009;20:1092–1098.
- Paolantonio M, Dolci M, Scarano A, et al. Immediate implantation in fresh extraction sockets. A controlled clinical and histological study in man. J Periodontol. 2001;72:1560–1571.
- Wilson TG Jr, Carino J, Schenk R, Cochran D. Immediate implants covered with connective tissue membranes: human biopsies. J Periodontol. 2003;74:402–409.
- Wilson TG Jr, Schenk R, Buser D, Cochran D. Implants placed in immediate extraction sites: a report of histologic and histometric analyses of human biopsies. Int J Oral Maxillofac Implants. 1998;13:333–341.
- Botticelli D, Berglundh T, Lindhe J. Hard-tissue alterations following immediate implant placement in extraction sites. J Clin Periodontol. 2004;31:820–828.
- Schropp L, Kostopoulos L, Wenzel A. Bone healing following immediate versus delayed placement of titanium implants into extraction sockets: a prospective clinical study. Int J Oral Maxillofac Implants. 2003;18:189–199.
- Puisys A, Linkevicius T. The influence of mucosal tissue thickening on crestal bone stability around bone-level implants. A prospective controlled clinical trial. Clin Oral Implants Res. 2015;26:123–129.
- Jung R, Sailer I, Hämmerle C, Attin T, Schmidlin P. In vitro color changes of soft tissues caused by restorative materials. Int J Periodontics Restorative Dent. 2007;27:251–257.
- Chappuis V, Engel O, Shahim K, Reyes M, Katsaros C, Buser D. Soft tissue alterations in esthetic postextraction sites: A 3-dimensional analysis. J Dent Res. 2015;94(Suppl):187S–193S.
- Pommer B, Hof M, Fädler A, Gahleitner A, Watzek G, Watzak G. Primary implant stability in the atrophic sinus floor of human cadaver maxillae: impact of residual ridge height, bone density, and implant diameter. Clin Oral Implants Res. 2014;25:e109–e113.
- Hsu J, Huang H, Chang C, Tsai M, Hung W, Fuh L. Relationship of three-dimensional bone-to-implant contact to primary implant stability and peri-implant bone strain in immediate loading: microcomputed tomographic and in vitro analyses. Int J Oral Maxillofac Implants. 2013;28:367–374.
- Becker W, Becker B. Guided tissue regeneration for implants placed into extraction sockets and for implant dehiscences: surgical techniques and case report. Int J Periodontics Restorative Dent. 1990;10:376–391.
- Werbitt M, Goldberg P. The immediate implant: bone preservation and bone regeneration. Int J Periodontics Restorative Dent. 1992;12:206–217.
- Evian CI, Emling R, Rosenberg ES, et al. Retrospective analysis of implant survival and the influence of periodontal disease and immediate placement on long-term results. Int J Oral Maxillofac Implants. 2004;19:393–398.
- Siegenthaler D, Jung R, Holderegger C, Roos M, Hämmerle C. Replacement of teeth exhibiting periapical pathology by immediate implants: a prospective, controlled clinical trial. Clin Oral Implants Res. 2007;18:727–737.
- Jung RE, Zaugg B, Philipp AO, Truninger TC, Siegenthaler DW, Hammerle CH. A prospective controlled clinical trial evaluating the clinical radiological and esthetic outcome after 5 years of immediately placed implants in sockets exhibiting periapical pathology. Clin Oral Implants Res. 2013;24:839–846.
- Manor Y, Oubaid S, Mardinger O, Chaushu G, Nissan J. Characteristics of early versus late implant failure: a retrospective study. J Oral Maxillofac Surg. 2009;67:2649–2652.
The authors have no commercial conflicts of interest to disclose.
Featured photo by ISTOCK.COM/LORADO
From Decisions in Dentistry. January 2017;3(1):14—16,18,21.
