

Screwmentable Implant Crowns
When restoring dental implants, this novel hybrid design presents a viable clinical alternative to screw-retained or cement-retained crowns.
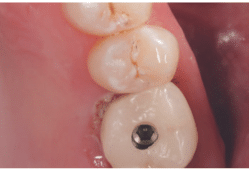
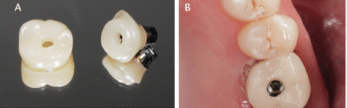
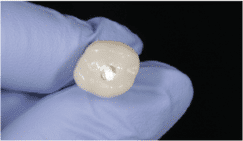
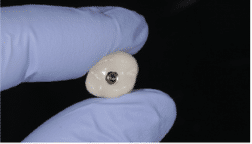
Two well-documented implant restorations are the screw-retained or cement-retained crown. However, clinicians can also choose a third type of implant restoration — the screwmentable implant crown, which offers clinical advantages unique to this novel design. As the name implies, a screw-retained crown connects directly to the endosseous dental implant. In the case of the cement-retained implant crown, the abutment connects directly to the implant, and the crown is then cemented to the abutment. The cement-retained crown has an access or “chimney” through the abutment, but there is no hole in the crown (Figure 1). The screwmentable implant crown, however, has an access channel in the abutment and a hole in the crown where the prosthesis sits directly over the access channel (Figures 2A and 2B).
The advantage of the screwmentable implant crown, unlike the screw-retained crown, is that the abutment can be screwed into place, just like a cement-retained crown. Once the abutment is positioned, the crown can be tried on and removed so contacts can be evaluated and adjusted accordingly. However, unlike a cement-retained crown, at the time of final delivery the entire prosthesis (including the titanium base, abutment and crown) can be cemented extraorally. It can then be thoroughly cleaned and polished so excess cement can be removed.
In comparison, the advantage of the screw-retained crown is that the operator does not have to be concerned with retained cement. A potential downside is that delivery can be quite arduous, as the process requires the frequent screwing and unscrewing of the prosthesis from the implant. In addition, depending on the presentation of the gingiva, the delivery process may be complicated by the collapse of the gingiva. An implant abutment may displace the gingiva to enable the ease of placement and removal of the implant crown. However, during iterations of placement and removal of a screw-retained crown, the gingiva may collapse and prevent seating of the restoration.
For screw-retained implant crowns, once the interproximal contact strength is deemed appropriate, the final crown is torqued into place for final delivery. If the contacts of the adjacent teeth are converging, the contact strength may change. This is because the implant crown will move slightly apically as it is torqued into place. This process does not always occur, particularly when the adjacent contacts are flat and broad. However, if the interproximal contacts are narrow and one (or both) of the adjacent teeth converge toward the crown, the contact may be lost as the crown is torqued down.
Clinically, the advantage of a cement-retained crown is typically its ease of deliverability. As mentioned, delivery of a screw-retained crown involves the frequent screwing and unscrewing of the prosthesis to evaluate interproximal contacts. With a cement-retained restoration, the abutment can be screwed down and kept in place while the crown itself is removed and replaced with ease as the operator evaluates and adjusts the contacts.
If there is a concern about residual cement with a cemented implant crown, the dentist always has the option to place the margins of the custom abutment supragingivally or at least equigingivally. This facilitates cement visualization and removal on the facial and lingual surfaces, but not necessarily the interproximal surface. However, the supragingival or equigingival placement of the margins of the custom abutment poses a problem for restorations in the esthetic zone. The transition between the abutment and crown may be visible and esthetically unacceptable to the patient. While cement-retained restorations have not been found to place implants at greater risk for peri-implantitis compared to screw-retained prostheses,1,2 a systematic review concluded the roughened surface caused by retained cement can facilitate biofilm formation.3
RETAINED CEMENT AND PERIODONTAL CONDITIONS
The retention of cement around the implant crown or in the surrounding soft tissue has been associated with peri-implant disease.4–6 But whether retained cement will always lead to peri-implantitis is somewhat unpredictable, as research suggests that retained cement causes disease in 9% to 81% of cases.7 Thus, not all implants with retained cement will succumb to peri-implantitis.8,9
Peri-implant disease is an inflammatory condition that can impact the hard and soft tissue around the dental implant.10 Its manifestations range from peri-implant mucositis to peri-implantitis. The former results in inflammation of the soft tissue, but there is no evidence of bone loss. This condition is considered the precursor to peri-implantitis. The progression of peri-implant mucositis to peri-implantitis mirrors the progression of gingivitis to periodontitis. If caught early, peri-implant mucositis is reversible. Peri-implantitis, however, results in deterioration of the bone adjacent to the implant.
Dental cement can retain pathogens that promote periodontal inflammation. The cement retained about the implant is rough and irregular, and thus serves as a reservoir for microorganisms. This makes the bacteria difficult to remove.
One prospective clinical trial found the signs of inflammation and peri-implant disease from retained cement can be evident as early as four months and as late as nine years after the restoration is cemented. This study demonstrated that removal of cement resulted in the resolution of the clinical signs of peri-implant disease 76% of the time.11
In some instances, a cement-retained crown may be the only treatment option. When the screw-access chamber is positioned facially or incisally in the esthetic region, a cement-retained crown may be the only viable choice. The access of the screw-retained or screwmentable implant restoration will be visible. Esthetically, the optical difference between the ceramic utilized for the restoration and composite used to cover the access may be too apparent.
FABRICATION
A screwmentable crown and abutment can be fabricated with a custom abutment. The access hole of the implant crown is the same diameter as the abutment and sits directly over the abutment. Specialized software allows the crown access hole to be designed and placed during the design and milling processes. With the growing recognition and appreciation of screwmentable implant crowns, more design programs may eventually offer the possibility of creating screwmentable prostheses.
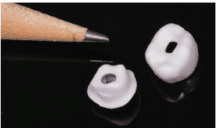
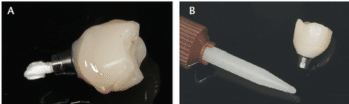
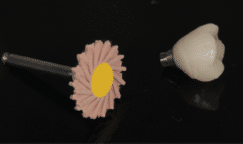
The access hole may also be created by the clinician chairside prior to the restoration being sintered (zirconia) or crystalized (lithium disilicate). In order to do this, the crown and custom abutment must first be milled out. While the abutment and crown are held together, a pencil that is sharpened thin enough to fit into the abutment chamber is used to trace the outline of the access hole onto the crown’s intaglio surface (Figure 3). From there, the outlined access hole is traced with a fine diamond bur on slow speed with ample water (Figure 4). Once the rough areas are smoothed and polished, the crown and abutment can be sintered or crystalized according to the manufacturer’s directions (Figure 5).

crown.

SCREWMENTABLE CROWN DELIVERY
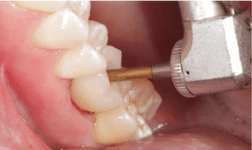
Cementation of the screwmentable crown can be completed intraorally or extraorally. Polytetrafluoroethylene tape (i.e., plumber’s tape) or cotton should be placed in the screw access chamber to prevent occlusion from cement (Figure 6). The crown is then cemented according to the manufacturer’s directions. Once the cement is placed, it must be quickly removed from the access chamber of the abutment, as should any cement occluding the hole in the crown (Figures 7A and 7B).

After the cement is cured, the plumber’s tape/cotton in the access opening (Figure 8) can be removed. The operator can now thoroughly visualize the prosthesis from 360° to verify all cement has been removed and the screw hole is not occluded (Figure 9). The ability to have unhindered complete visualization of cemented margins is perhaps the greatest benefit of the screwmentable implant crown. In the event cement remains, it can be easily cleaned off and polished (Figure 10). Careful consideration is needed during this process to ensure the abutment and crown are not scratched, as scratching the prosthesis may cause surface irregularities and subsequent plaque retention, which may lead to peri-implant disease.
The operator now has the option to place glycerin over the cement margins and cure it one more time to eliminate the oxygen inhibited layer (OIL). The OIL is a superficial layer that is formed during the polymerization of resin composite. Oxygen inhibits the polymerization reaction, which is why a superficial layer approximately 10 to 30 microns thick of uncured composite is left on the restoration.12 The OIL is prone to wear, staining and plaque retention.
Once the dentist is satisfied, the cemented screwmentable prosthesis can be replaced and torqued into place according to the manufacturer’s directions (Figure 11). Plumber’s tape is once again placed in the abutment access chamber and the hole over the crown is sealed with composite. It is imperative that a barrier is placed in the abutment chamber to facilitate future retrievability. The operator should then bond the composite being placed in the access hole rather than simply placing it without bonding. Composite shrinks once it is polymerized, and if the composite is not bonded to the ceramic in the access hole, it may result in bacterial ingress into the abutment chamber.
Bonding composite to the access hole is dependent on the restorative material selected. If the crown/abutment is fabricated from lithium disilicate, the clinician will etch the material with hydrofluoric acid according to the manufacturer’s directions and apply silane. The operator can then apply adhesive to the ceramic and restore the access with resin composite. On the other hand, if composite is being bonded to zirconia, the zirconia is roughened with 50-micron aluminum oxide before the surface is treated with a primer containing a 10-methacryloyloxydecyl dihydrogen phosphate monomer. Next, composite is applied and cured. While utilizing air particle abrasion on zirconia, the provider must be careful to ensure the rest of the implant crown is not abraded.
Interproximal contacts and occlusal contact should be verified once more, and a final bitewing radiograph should be made to confirm complete seating of the abutment and that all excess cement has been removed.
is not occluding the hole.
RETRIEVABILITY
The screwmentable implant crown, like the screw-retained crown, offers the possibility of future retrievability of the prosthesis. Over time, the crown may need to be replaced or modified despite a healthy integrated implant. A retrospective clinical study with a 10-year follow-up demonstrated the loss of at least one interproximal contact in over 50% of implants. The mesial interproximal contact was lost more frequently than the distal contact.13 Loss of the interproximal contact may lead to food impaction and plaque accumulation, and thus caries on the adjacent tooth (if the implant is next to a natural tooth).
The implant crown may also need to be replaced due to screw loosening. Abutment screw loosening is one of the most common prosthetic complications for both cement-retained and screw-retained implant restorations. It has been reported to occur as frequently as 12.7% to 43% of the time.14,15 A loose abutment is problematic because it can increase the microgap between the implant and abutment, and also lead to the ingrowth of granulation tissue and soft tissue infection.16
CONCLUSION
A host of factors contributes to the success and survivability of an implant restoration. Screw-retained and cement-retained implant crowns have a well-documented history of success and should not be discarded as treatment options. However, the screwmentable implant crown offers an additional clinical solution that may be preferred in some situations.
A chief advantage of this hybrid design is that once the abutment is positioned, the screwmentable crown can be tried on and removed for contact evaluation and adjustment. And, at the time of final delivery, the entire prosthesis (including the titanium base, abutment and crown) can be cemented extraorally. It can then be thoroughly cleaned and polished to ensure excess cement has been removed. The use of this clinical approach allows unhindered 360° visualization of the cemented margins so operators can easily check for residual cement that might otherwise lead to peri-implant disease. Equally helpful, use of a screwmentable crown allows future retrievability if the prosthesis ever needs to be adjusted or replaced.
The author has no commercial conflicts of interest to disclose.
KEY TAKEAWAYS
- As a hybrid of the traditional screw-retained and cement-retained implant restoration, the screwmentable implant crown offers unique clinical advantages.
- Unlike a screw-retained prosthesis, one benefit of a screwmentable crown is that once the abutment is positioned, the crown can easily be tried on and removed so contacts can be evaluated and adjusted.
- However, unlike a cement-retained crown, at the time of final delivery the entire prosthesis (including the titanium base, abutment and crown) can be cemented extraorally. It can then be thoroughly cleaned and polished so excess cement can be removed.
- Cementation of the screwmentable crown can also be completed intraorally.
- After the cement is cured, the operator can now thoroughly visualize the prosthesis from 360° to verify all cement has been removed and the screw hole is not occluded.
- The ability to have unhindered visualization of the cemented margins is perhaps the greatest benefit of the screwmentable implant crown.
- Once the dentist is satisfied, the cemented screwmentable prosthesis can be torqued into place.
- The screwmentable implant crown, like the screw-retained crown, offers the possibility of future retrievability of the prosthesis.
References
- Daubert DM, Weinstein BF, Bordin S, Leroux BG, Flemming TF. Prevalence and predictive factors for peri-implant disease and implant failure: a cross-sectional analysis. J Periodontol. 2015;86:337–347.
- Marrone A, Lasserre J, Bercy P, Brecx MC. Prevalence and risk factors for peri-implant disease in Belgian adults. Clin Oral Implants Res. 2013;24:934–940.
- Staubli N, Walter C, Schmidt JC, Weiger R, Zitzmann NU. Excess cement and the risk of peri-implant disease — a systematic review. Clin Oral Implants Res. 2017;28:1278–1290.
- Pauletto N, Lahiffe BJ, Walton JN. Complications associated with excess cement around crowns on osseointegrated implants: A clinical report. Int J Oral Maxillofac Implants. 1999;14:865–868.
- Gapski R, Neugeboren N, Pomeranz AZ, Reissner MW. Endosseous implant failure influenced by crown cementation: a clinical case report. Int J Oral Maxillofac Implants. 2008;23:943–946.
- Lang NP, Berglundh T, Heitz-Mayfield LJ, Pjetursson BE, Salvi GE, Sanz M. Consensus statements and recommended clinical procedures regarding implant survival and complications. Int J Oral Maxillofac Implants. 2004;19(Suppl):150–154.
- Schwarz F, Derks J, Monje A, Wang HL. Peri-implantitis. J Periodontol. 2018;89(Suppl 1):S267–S290.
- Korsch M, Obst U, Walther W. Cement-associated peri-implantitis: a retrospective clinical observational study of fixed implant-supported restorations using a methacrylate cement. Clin Oral Implants Res. 2014;25:797–802.
- Korsch M, Walther W, Bartols A. Cement-associated peri-implant mucositis. A 1-year follow-up after excess cement removal on the peri-implant tissue of dental implants. Clin Implant Dent Relat Res. 2017;19:523–529.
- Valente NA, Andreana S. Peri-implant disease: what we know and what we need to know. J Periodontal Implant Sci. 2016;46:136–151.
- Wilson TG Jr. The positive relationship between excess cement and peri-implant disease: a prospective clinical endoscopic study. J Periodontal. 2009;80:1388–1392.
- Gaviria-Martine, A, Castro-Ramirez L, Ladera-Castañeda M, et al. Surface roughness and oxygen inhibited layer control in bulk-fill and conventional nanohybrid resin composites with and without polishing: in vitro study. BMC Oral Health. 2022;22:258.
- Gasser TJW, Papageorgiou SN, Eliades T, Hämmerle CHF, Thoma DS. Interproximal contact loss at implant sites: a retrospective clinical study with a 10-year follow-up. Clin Oral Implants Res. 2022;33:482–491.
- Pjetursson BE, Bragge U, Lang NP, Zwahlen M. Comparison of survival and complication rates of tooth-supported fixed dental prostheses (FDPs) and implant-supported FDPs and single crowns (SCs). Clin Oral Implants Res. 2007:18(Suppl 3):97–113.
- Jemt T, Laney WR, Harris D, et al. Osseointegrated implants for single tooth replacement: a 1-year report from a multicenter prospective study. Int J Oral Maxillofac Implants. 1991;6:29–36.
- Goodacre CJ, Kan JYK, Rungcharassaeng K. Clinical complications of osseointegrated implants. J Prosthet Dent. 1999;81:537–552.
From Decisions in Dentistry. April 2023;9(4):16,18,20,22.

Question: what torque value is used to torque in the abutment when ‘fitting ‘ the crown? Hand torque?or full torque? And are there any studies to show best fit to interproximal contacts with either torque value?