
 LukaTDB / E+
LukaTDB / E+
Risk Assessment for Immediate Implant Treatment
Four key factors help determine a patient’s presurgical risk for immediate dental implant therapy.
The primary objectives of immediate implant therapy are to decrease treatment time and the number of surgical procedures, while improving overall patient satisfaction. Lazzara1 reported the first immediate dental implant placement, and Wohrle2 first detailed immediate provisionalization of an immediate implant. In a systematic review, Lang et al3 reported an overall success rate of 98.4% for immediate implants.
It is axiomatic that thorough site evaluation and patient selection are crucial to the success of immediate implant treatment. Based on the dental implant literature, this paper proposes a risk profile that can be used to evaluate the recipient site prior to immediate implant therapy. The key elements used in the profile should be helpful when selecting cases that will mitigate the risk of immediate implant surgical complications, including failures. The main components of a risk profile can be broadly stratified into four categories: hard tissue evaluation, soft tissue evaluation, systemic factors, and compliance.
HARD TISSUE EVALUATION
Socket Bone Morphology — Intact socket walls are ideal for immediate implant treatment. Elian et al4 suggested a simple classification to categorize extraction sockets. Type I sockets present intact soft tissue and a socket morphology conducive to immediate implant care. Type II sockets show buccal dehiscence, with intact soft tissue, whereas Type III sockets reveal both buccal plate and soft tissue dehiscence. However, Chu et al5 reported successful immediate implant placement with simultaneous bone grafting and provisionalization in the maxillary premolar areas in Type II sockets. In addition, Chaar et al6 reported immediate implant placement without temporization in Type II defects with buccal osseous dehiscence, adequate interproximal bone height, and sufficient apical bone to provide primary stability. Nevertheless, it is prudent to consider a staged or delayed implant treatment approach in Type II and Type III defects, especially in maxillary anterior sites characterized by a high smile line and thin periodontal phenotype.
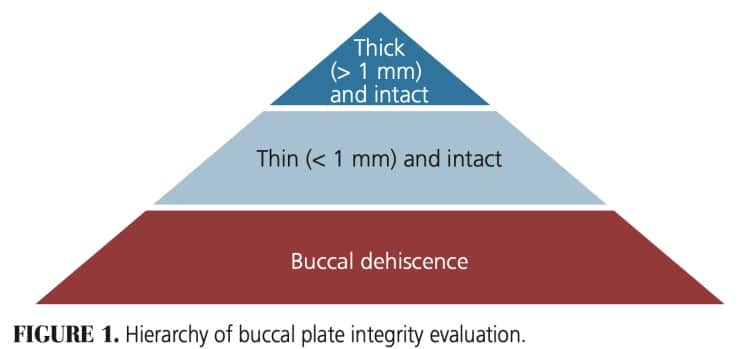
Buccal Plate Integrity — Buccal plate thickness and intactness are vital for immediate implant placement. Morton et al7 suggested that a buccal plate thickness of 1 mm is ideal for immediate implants. In this regard, Huynh-Ba et al8 noted that 87% of anterior sites have labial plate thickness less than 1 mm, and Janaurio et al9 determined the average labial plate thickness around maxillary anterior teeth to be approximately 0.6 mm. Zhang et al10 reported an interesting finding in that maxillary lateral incisors exhibit a thin labial plate and a frequent undercut close to the alveolar ridge. Additionally, Cheng et al11 determined an intact buccal plate to be a more critical feature than thickness. Based on available literature, the hierarchy of buccal plate evaluation can be summarized as thick (> 1 mm) and intact buccal plate is better than thin and intact, which, in turn, is better than buccal dehiscence socket morphology (Figure 1).
Interproximal Crestal Bone Height — The level (height) of interproximal bone crest can be measured radiographically or during clinical evaluation with a bone sounding technique. In a retrospective study, Tarnow et al12 showed the importance of maintaining an appropriate distance between the crestal bone height to the contact point for the creation of ideal interproximal papillary esthetics. The authors noted that a distance of 5 mm from the interproximal bony crest to the contact point of adjacent teeth allows for ideal gingival papillae formation, with 100% fill of the interproximal space. When the distance is increased to 6 mm, the papillary fill decreases to 56%. Salama et al13 developed a three-tier classification for “interproximal height of bone,” and stated that optimal esthetics is achievable when the interproximal height of bone is 4 to 5 mm from the interproximal contact point. In contrast, Roccuzzo et al14 asserted there is insufficient evidence regarding the influence of the space between the interproximal contact to the bony osseous crest and the degree of papillary height and/or percent of fill. The authors also noted that for single-tooth implants, interproximal papillary height is dependent upon the clinical attachment level of the adjacent tooth. Hence, lesser distance between interproximal bone height and interproximal contact is suggested to attain predictable papillary fill.
Residual Bone — The presence of apical and palatal bone is important for attaining primary stability for immediate implants. It is reported that 3 to 5 mm of native apical bone is essential for engaging the apical part of the implant and providing primary stability.15–17 Kan et al18 developed a classification system based on the sagittal root position in cone beam computed tomography that helps evaluate the available palatal bone for immediate implant placement. Class I is considered ideal, with root positioning more toward the labial cortical plate, which thus provides adequate amount of palatal (as well as the apical) bone to support the immediate implant. Class II has mid-center root position in the alveolar housing, and Class III has root positioning more toward the palatal cortical plate. Class IV, which is defined as having nearly two-thirds of the root engaging both the buccal and palatal cortical plate, is not recommend for immediate implants.
Periapical Pathology — Successful osseointegration has been reported when immediate implants are placed following extraction of teeth with chronic periapical lesions.19 However, a 2019 study revealed that residual microbes in the extraction site can lead to retrograde peri-implantitis.20 Following thorough debridement, clinicians are advised to eliminate bacterial contamination of the implant surface and consider irrigating with antimicrobials21 prior to implant placement. It is also necessary to evaluate the size and nature of the lesion (e.g., chronic versus acute). If the peri-apical lesion is large (e.g., extending to adjacent teeth) or there is a history of multiple endodontic procedures, the site needs critical evaluation for immediate versus delayed implant treatment. When evaluating patients for immediate implants, Chaar et al6 recommends selecting cases with no acute infection.
SOFT TISSUE EVALUATION
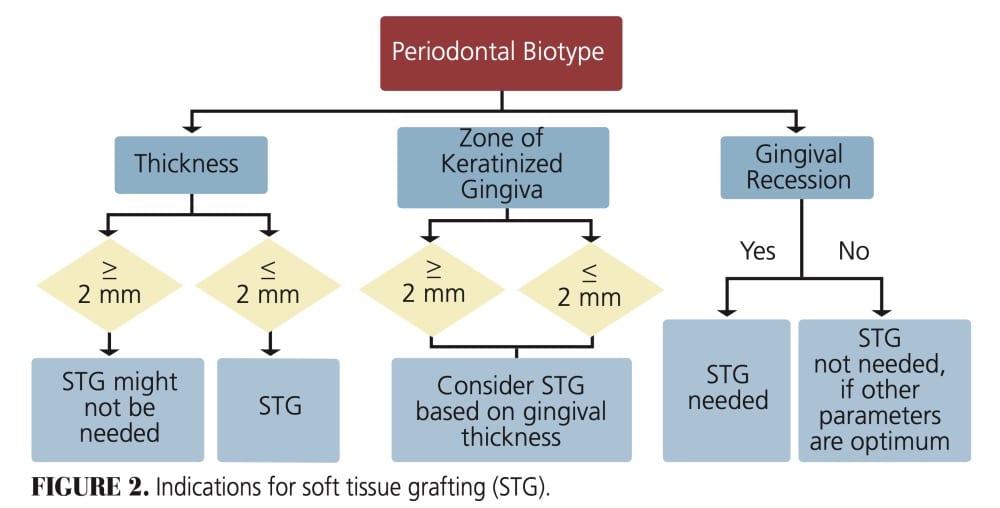
Gingival Phenotype — Periodontal phenotype (previously referred to as biotype) assessment should include both thickness, which is a horizontal measurement from buccal to palatal or lingual, and zone of keratinized gingiva, which is a vertical measurement from free gingival margin to the mucogingival junction. Based on thickness, gingiva is broadly classified into thick, average and thin phenotypes.22 Numerous studies have shown that a thick phenotype is associated with thicker labial plate22,23 and wider zone of keratinized gingiva.24 Soft tissue phenotype is an important component in maintaining optimal crestal bone level, peri-implant gingival health and restoration esthetics. It also prevents gingival recession around the implant. Immediate implant treatment can be performed even with thin periodontal phenotypes that exhibit optimal buccal plate integrity.
When faced with a thin phenotype overlying an intact buccal plate, simultaneous connective tissue or allogenic grafting can be performed to convert from a thin to thick phenotype (see “Healing Progression of the Free Gingival Graft,” page 26). Such a phenotype conversion will aid in maintaining a wider zone of keratinized gingiva and may reduce the risk of crestal bone loss.25 Esper et al26 recommend a minimum width of 2 mm of keratinized gingiva around implants to maintain good peri-implant health. In this regard, Linkevicius et al27 reported a crestal bone loss of 1.45 mm when gingival thickness is ≤ 2.5 mm. Jung et al28 notes that a gingival thickness of 2 mm is ideal to maintain esthetics. The Figure 2 flowchart provides indications for soft tissue augmentation.
Gingival Symmetry — It is important to assess gingival symmetry prior to tooth extraction. Some anterior cases might exhibit gingival asymmetry resulting from passive eruption, previous trauma, orthodontic treatment or restorative procedures. Gingival symmetry can be accomplished with soft tissue grafts, crown lengthening, forced eruption, or with localized gingivectomy procedures.
Aberrant Frenum — In their systematic review on maxillary midline frenula, Delli et al29 determined the potential role of a frenum in marginal gingival recession and peri-implant disease was inconclusive. However, a frenal attachment encroaching on the marginal gingiva should be removed to maintain good peri-implant health.

SYSTEMIC FACTORS
Systemic conditions can compromise implant treatment outcomes.30,31 Conditions such as diabetes mellitus, severe osteoporosis, cardiovascular disease, bleeding disorders and immunosuppression need thorough evaluation — and, in certain circumstances, clearance from a physician prior to implant treatment.
In patients with well-controlled diabetes (HbA1c < 7.5%), dental implant treatment — including guided bone regeneration — yielded similar results when compared to controls.32 Smoking cessation is strongly encouraged prior to initiation of implant therapy. In a systematic review of the effect of smoking on implant failure, Keenan et al33 reported increased postoperative infections, marginal bone loss, and failures in patients who smoked. Similarly, Mumcu and Beklen34 note that smokers exhibit a time-dependent and higher marginal bone loss around both fixed and removable implant prostheses than controls.
Recently, a few medications belonging to selective serotonin reuptake inhibitors (e.g., citalopram, escitalopram, fluoxetine, paroxetine, sertraline and vilazodone) and proton pump inhibitors (e.g., omeprazole, lansoprazole, dexlansoprazole, rabeprazole and pantoprazole) are reported to have a negative impact on osseointegration.31
COMPLIANCE
Patient compliance is crucial to the success of immediate implant treatment. During initial consultation, patients should be educated about their role in achieving predictable outcomes. Dietary, physical activity and hygiene restriction (at the proposed site) should be thoroughly reviewed and readdressed during postoperative appointments to minimize dental implant complications. In addition, patients will require regular periodontal maintenance after implant therapy to maintain peri-implant health.35
The four-factor, presurgical risk profile presented here allows comprehensive case evaluation for immediate implant treatment. Risk assessment helps clinicians select appropriate cases, thus minimizing complications and failures. Clinicians should perform immediate implant placement only in patients classified as optimal or low risk to maintain good surgical and esthetic outcomes. A staged approach — including bone grafting, with or without soft tissue augmentation — should be performed in cases with a high risk profile.
Among these four categories, buccal plate intactness in the hard tissue group, and periodontal phenotype in the soft tissue category are key determinants of risk. The final two parameters (systemic/host factors and compliance) must also be met before proceeding with immediate implant treatment.
During case evaluation, if the profile parameters are spread across all risk categories, greater weight should be given to hard tissue parameters (as opposed to soft tissue factors). However, within the hard tissue category, socket morphology and buccal plate intactness are critical when compared to other parameters. It would be ideal for all hard tissue parameters to be in the optimal or low risk category before proceeding with immediate implant treatment. On the other hand, even if the soft tissue parameters are not optimal, they are modifiable and can be corrected during the immediate implant procedure (as long as the site’s presenting bone morphology is adequate).
The following case reports illustrate the presurgical risk profile determination.
CLINICAL CASE 1
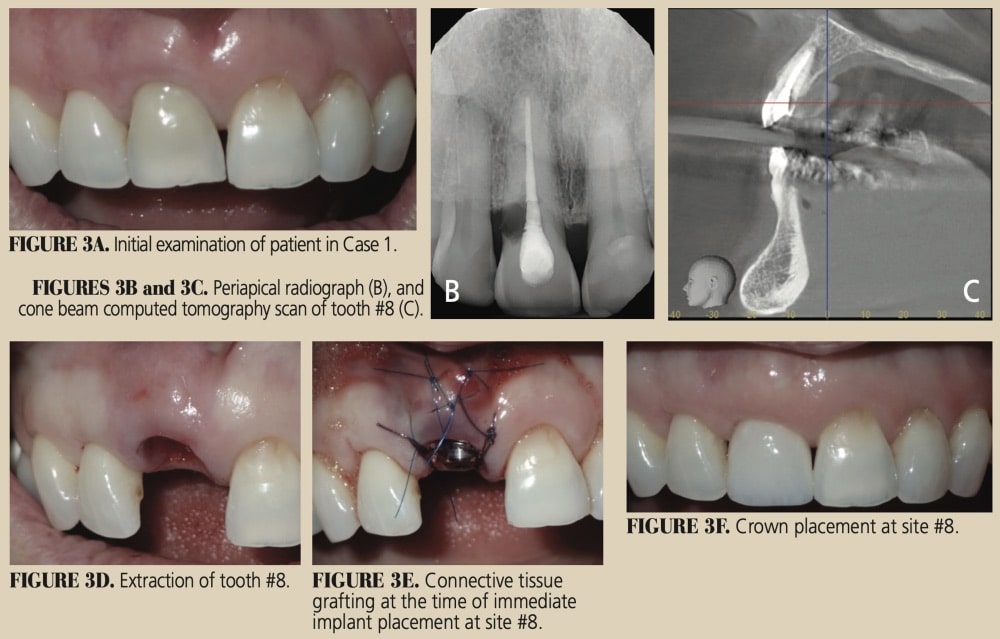
A 65-year old female was referred for implant treatment to replace tooth #8 due to internal resorption. Clinical and radiographic examination identified a high lip line, loss of the interproximal papillae around the maxillary anterior teeth, cervical abrasion on teeth #9 and 10, and uneven incisal edges between #8 and 9 (Figures 3A through 3F). Her risk profile determination is shown below (and also presented graphically in the online version of this article).
Risk Profile Analysis for Clinical Case 1
Hard tissue analysis: Risk evaluation is optimal, with Type I socket, intact buccal plate with a thickness of 0.5 mm, and interproximal bone height of 5 mm. Residual available apical and palatal bone is adequate to attain good primary stability. A chronic periapical lesion is noted on the cone beam scan and will need thorough debridement during the tooth extraction.
Soft tissue analysis: Periodontal phenotype is thin and will require soft tissue augmentation at the time of immediate implant placement. Alternately, the team can observe and evaluate implant healing for four months and treat as indicated.
Host factors: Nothing significant.
Compliance: Excellent.
This risk profile analysis determines the patient to be an optimal candidate for immediate implant treatment with simultaneous connective tissue grafting.

CLINICAL CASE 2
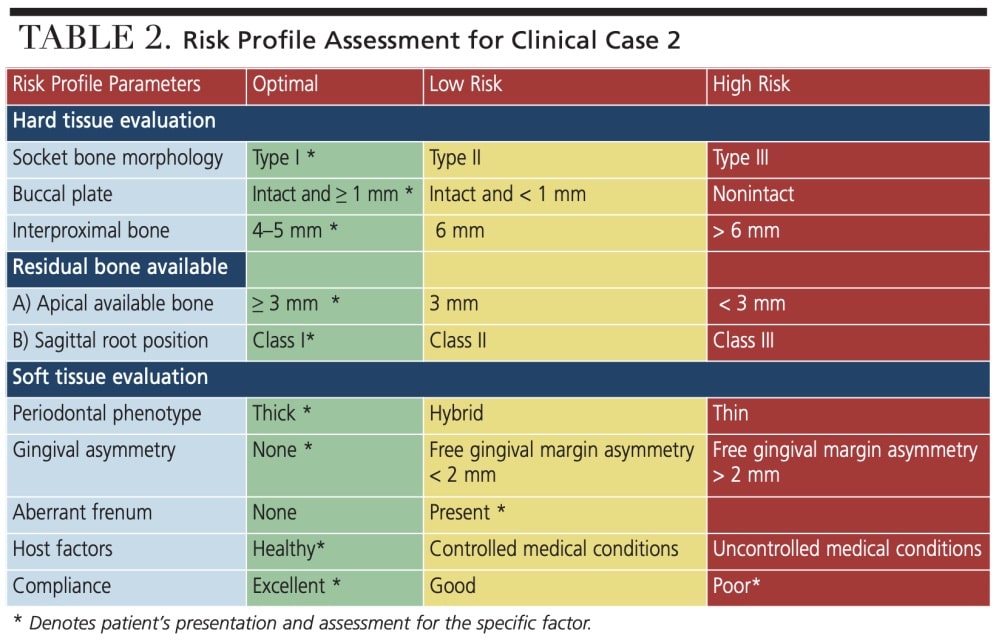
A 22-year old male was referred for implant treatment due to a nonrestorable tooth #8, which presented with cervical resorption. Clinical examination identified a thick periodontal phenotype, with slight loss of interproximal papilla between teeth #7 and 8, and a high frenal attachment. Radiographic evaluation noted an intact buccal plate, good interproximal bone, and no periapical pathology (Figures 4A through 4J).
Risk Profile Analysis for Clinical Case 2
Hard tissue analysis: Optimal.
Soft tissue analysis: Optimal. Frenum shows no pull on the marginal gingivae of teeth #8 and 9. Hence, frenectomy is not indicated.
Host factors: Optimal.
Compliance: Excellent.
Based on the risk profile determination, this patient is a good candidate for immediate implant treatment.
CONCLUSION
The risk assessment tool presented here is simple and effective. The risk profile is based on peer-reviewed literature and designed to help clinicians determine whether an immediate or delayed implant procedure should be performed following tooth extraction. With careful assessment and proper screening, immediate implant therapy is a predictable treatment approach. However, failure to follow good clinical guidelines could lead to catastrophic failures.
Key Takeaways
- Thorough site evaluation and patient selection are crucial to the success of immediate dental implant treatment.
- This paper proposes a risk profile that can be used to evaluate the recipient site prior to immediate implant therapy.
- The main components of risk can be stratified into hard tissue evaluation, soft tissue evaluation, systemic factors and compliance.
- Among these four categories, buccal plate intactness in the hard tissue group, and periodontal phenotype in the soft tissue category are key determinants of risk.
- The final two parameters — systemic factors and compliance — must also be met before proceeding with immediate implant treatment.
Acknowledgement: The author thanks Charles M. Cobb, DDS, MS, PhD, professor emeritus in the Department of Periodontics at the University of Missouri-Kansas City School of Dentistry, and Kristen Simmons, MHA, BSDH, RDH, chief operating officer of Willamette Dental Group, for their input during the preparation of this manuscript. The author also acknowledges Neha Myneni, 12th grade, Catlin Gabel School, for her help with the figures and online tables.
References
- Lazzara RJ. Immediate implant placement into extraction sites: surgical and restorative advantages. InJ J Periodontics Restorative Dent. 1989;9:332–343.
- Wöhrle PS. Single tooth replacement in the aesthetic zone with immediate provisionalization: fourteen consecutive case reports. Prac Periodontics Aesthet Dent. 1998;10:1107–1114.
- Lang NP, Pun L, Lau KY, Li KY, Wong MC. A systematic review on survival and success rates of implants placed immediately into fresh extraction sockets after at least 1 year. Clin Oral Implants Res. 2012;23(Suppl 5):39–66.
- Elian N, Cho SC, Froum S, Smith RB, Tarnow DP. A simplified socket classification and repair technique. Pract Proced Aesthet Dent. 2007;19:99–104.
- Chu SJ, Sarnachiaro GO, Hochman MN, Tarnow DP. Subclassification and clinical management of extraction sockets with labial dentoalveolar dehiscence defects. Compend Contin Educ Dent. 2015;36:516,518–520,522.
- Chaar EE, Oshman S, Abed PF. Single-rooted extraction sockets: classification and treatment Protocol. 2016. Compend Contin Educ Dent. 2016;37:537–541.
- Morton D, Chen ST, Martin WC, Levine RA, Buser D. Consensus statements and recommended clinical procedures regarding optimizing esthetic outcomes in implant dentistry. Int J Oral Maxillofac Implants. 2014;29(Suppl):216–220.
- Huynh‐Ba G, Pjetursson BE, Sanz M, et al. Analysis of the socket bone wall dimensions in the upper maxilla in relation to immediate implant placement. Clin Oral Implants Res 2010;21:37–42.
- Januário AL, Duarte WR, Barriviera M, Mesti JC, Araújo MG, Lindhe J. Dimension of the facial bone wall in the anterior maxilla: a cone-beam computed tomography study. Clin Oral Implants Res. 2011;22:1168–1171.
- Zhang W, Skrypczak A, Weltman R. Anterior maxilla alveolar ridge dimension and morphology measurement by cone beam computerized tomography (CBCT) for immediate implant treatment planning. BMC Oral Health. 2015;15:65.
- Cheng AW, Berridge JP, McGary RT, Erley KJ, Johnson TM. The extraction socket management continuum: A hierarchical approach to dental implant site development. Clin Adv Perio. 2018;9:91–104.
- Tarnow DP, Maner AW, Fletcher P. The effect of distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papillae. J Periodontol. 1992;63:995–996.
- Salama H, Salama MA, Garber D, Adar P. The interproximal height of bone: a guidepost to predictable aesthetic strategies and soft tissue contours in anterior tooth replacement. Pract Periodontics Aesthet Dent. 1998;10:1131–1141.
- Roccuzzo M, Roccuzzo A, Ramanuskaite A. Papilla height in relation to the distance between bone crest and interproximal contact point at single-tooth implants: a systematic review. Clin Oral Implants Res. 2018;29(Suppl 15):50–61.
- Kois JC. Predictable single-tooth peri-implant esthetics: Five diagnostic keys. Compend Contin Educ Dent. 2004;25:895–905.
- Resnik RR, Misch CE. Avoiding Complications in Oral Implantology. Elsevier: St. Louis; 2017.
- Werbitt M, Goldberg P. The immediate implant: bone preservation and bone regeneration. Int J Periodontics Restorative Dent. 1992;12:206–217.
- Kan JY, Roe P, Rungcharassaeng K, et al. Classification of sagittal root position in relation to the anterior maxillary osseous housing for immediate implant placement: a cone beam computed tomography study. Int J Oral Maxillofac Implants. 2011;26:873–876.
- Lee CT, Chuang SK, Stoupel J. Survival analysis and other clinical outcomes of immediate implant placement in sites with periapical lesions: systematic review. Int J Oral Maxillofac Implants. 2015;30:268–278.
- Sarmast ND, Wang HH, Sajadi AS, Munne AM, Angelov N. Nonsurgical endodontic treatment of necrotic teeth resolved apical lesions on adjacent implants with retrogra/e/apical peri-implantitis: a case series with 2-year follow-up. J Endod. 2019;45:645–650.
- Chrcanovic BR, Martins MD, Wennerberg A. Immediate placement of implants into infected sites: a systematic review. Clin Implant Dent Relat Res. 2015;17(Suppl 1):e1–e16.
- Cook DR, Mealey BL, Verrett RG, et al. Relationship between clinical periodontal biotype and labial plate thickness: an in vivo study. Int J Periodontics Restorative Dent. 2011;31:345–354.
- Zweers J, Thomas RZ, Slot DE, Weisgold AS, Van der Weijden FG. Characteristics of periodontal biotype, its dimensions, associations and prevalence: a systematic review. J Clin Periodontol. 2014;41:958–971.
- Díaz-Sánchez M, Soto-Peñaloza D, Peñarrocha-Oltra D, Peñarrocha-Diago M. Influence of supracrestal tissue attachment thickness on radiographic bone level around dental implants: a systematic review and meta-analysis. J Periodontal Res. 2019;54;573–588.
- Puisys A, Linkevicius T. The influence of mucosal tissue thickening on crestal bone stability around bone-level implants. A prospective controlled clinical trial. Clin Oral Implants Res. 2015;26:123–129.
- Esper LA, Ferreira SB Jr, de Oliveira Fortes Kaizer R, de Almeida AL. The role of keratinized mucosa in peri-implant health. Cleft Palate Craniofac J. 2012;49:167–170.
- Linkevicius T, Apse P, Grybauskas S, Puisys A. The influence of soft tissue thickness on crestal bone changes around implants: a 1-year prospective controlled clinical trial. Int J Oral Maxillofac Implants. 2009;24:712–719.
- Jung RE, Heitz-Mayfield L, Schwarz F, Groups of the 2nd Osteology Foundation Consensus Meeting. Evidence-based knowledge on the aesthetics and maintenance of peri-implant soft tissues: Osteology Foundation Consensus Report Part 3 — aesthetics of peri-implant soft tissues. Clin Oral Implants Res. 2018;29(Suppl 15):14–17.
- Delli K, Livas C, Sculean A, Katsaros C, Bornstein MM. Facts and myths regarding the maxillary midline frenum and its treatment: a systematic review of the literature. Quintessence Int. 2013;44:177–187.
- Donos N, Calciolari E. Dental implants in patients affected by systemic diseases. Br Dent J. 2014;217:425–430.
- Aghaloo T, Pi-Anfruns J, Moshaverinia A, Sim D, Grogan T, Hadaya D. The effects of systemic diseases and medications on implant osseointegration: a systematic review. Int J Oral Maxillofac Implants. 2019;34(Suppl):s35–s49.
- Erdogan Ö, Uçar Y, Tatlı U, Sert M, Benlidayı ME, Evlice B. A clinical prospective study on alveolar bone augmentation and dental implant success in patients with type 2 diabetes. Clin Oral Implants Res. 2015;26:1267–1275.
- Keenan JR, Veitz-Keenan A. The impact of smoking on failure rates, postoperative infection and marginal bone loss of dental implants. Evid Based Dent. 2016;17:4–5.
- Mumcu E, Beklen A. The effect of smoking on the marginal bone loss around implant-supported prostheses. Tob Induc Dis. 2019;20:17–43.
- Lin CY, Chen Z, Pan WL, Wang HL. The effect of supportive care in preventing peri-implant diseases and implant loss: a systematic review and meta-analysis. Clin Oral Implants Res. 2019;30:714–724.
From Decisions in Dentistry. October 2020;6(9): 14-16, 18.
