
 Mykola Pokhodzhay / istock / Getty Images Plus
Mykola Pokhodzhay / istock / Getty Images Plus
Reducing the Risk of Implant-Abutment Screw Loosening
Dentists can minimize the risk of this common complication by understanding how the screw joint works — and ways to control the forces working against it.
This article was developed as a more in-depth version of the three-part “7 Habits of Highly Effective Implant Clinicians” series published by Decisions in Dentistry in 2022. The original series was intended to help reduce the issue of abutment screw loosening, which is a significant complication in implant dentistry. This extended paper will further address the causes of screw loosening, and offer strategies to minimize the risk.
Considered a “system,” screw joints have been relied on for joining materials together for hundreds of years.1,2 This system is totally dependent on the screw and confluence of the component parts — all are equally important for a stable and optimally functioning joint. Failure is problematic, and the solution may involve a straightforward fix, such as retightening the screw, to addressing catastrophic failure and breakage of the joint components.
Implant abutment (IA) screw-joint loosening affects 5% to 12% of all single implant crowns within the first five to six years following placement and use.3–7 The risk of screw loosening can be greatly reduced by understanding how the screw system works, using appropriate materials (i.e., components) and tools, and regularly monitoring the implant restoration so clinicians can mitigate the negative forces that act upon it.
This paper will focus on controlling the factors that contribute to IA screw-joint failure, such as operator error (the most common factor),1 mechanical misfit, and biological changes within the patient’s stomatological system. First, an understanding of the objectives, materials, and tools used in the IA joint is required.
HOW THE IMPLANT ABUTMENT SCREW JOINT WORKS
As operators controlling the screw joint, dentists can reduce the risk of failure by understanding how the joint works — and ways to control the forces working both with it, and against it.
The first force to consider is torque, which is a rotational force on the screw.1,2 The screw contains a helical thread that, when rotated, drives it up or down vertically within the implant, corresponding to the direction of rotation. In implant dentistry, the screw is usually made from titanium, titanium alloy, or a material similar to that of the implant body, so as not to cause frictional wear or damage to either part during use. Friction opposes the movement of the screw threads as they engage the implant threads during tightening. As an example, titanium and its alloys have a very high coefficient of kinetic friction of approximately 0.8 to 0.9; by comparison, ice on ice is approximately 0.03.8 High friction requires a high amount of energy when tightening the screw.
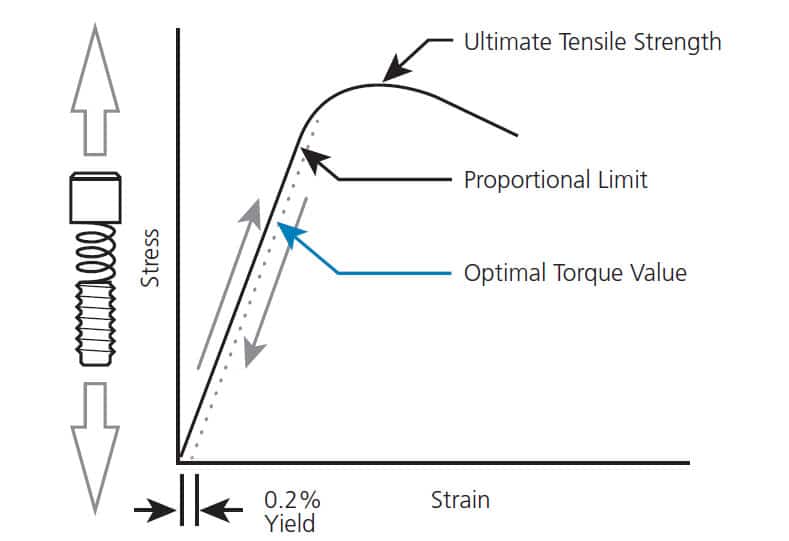
Paradoxically, even though friction makes it more difficult to tighten the screw, friction not only prevents the screw from loosening,1,2,9 it also enables optimization of the screw joint by maintaining the screw position as the joint is placed under tension. Simply put, friction holds the screw as it is being put under tension and stretched in an elastic spring-like action, drawing the joint components together (Figure 1). Known as clamping force, this is the mechanism that ultimately holds the screw joint and provides stability.10,11
Preload is the measure of the stretch in the screw, and it is important to realize this force has an optimal value.10,11 Just like any elastic material, if the preload is insufficient, the clamping force is too low; conversely, if the preload is too high, the screw is stretched too far, and it can deform and fail. The preload value is calculated by the implant manufacturer at a point that achieves optimum torque and efficiency (Figure 1).1,10 This specified tightening torque value must be strictly adhered to, as this is a fundamental rule of implant dentistry.1,2,9
Non-axial occlusal forces are the greatest challenge for IA screw joint stability. Even an optimally tightened, “perfect” implant screw joint can fail as a result of off-axial forces. It is critical to recognize this issue and the role that lateral forces from the chewing cycle and bruxing exert on a screw joint.1,2
Another important issue affecting IA screw joints is how well the abutment fits into the implant. Congruence is essential, and, just like a jigsaw puzzle piece, the abutment should perfectly match where it is designed to seat.10
Component tolerance and design are tightly controlled by the manufacturer (the reason being that if the fit is not optimal, the IA joint is more likely to fail). Today’s clinicians have multiple options when choosing abutments, but, when making the choice (or leaving the decision to the dental laboratory), the use of original equipment manufacturer (or OEM) components is encouraged, as these have been shown in multiple studies to be superior in preventing abutment screw loosening.10–13

(bottom) cantilever spring type.
PROVIDING OPTIMUM TIGHTENING TORQUE
Target torque value is the term used to describe how tight the screw should be. This can only be achieved if special torque-limiting devices are used. Torque values for hand-tightened IA screws in a simulated oral environment have been shown to vary between 4 and 21 Ncm.14 Abutment screws are small and commonly made of titanium alloy that requires a final abutment screw torque of approximately 20 to 35 Ncm. As noted, torque-limiting devices (commonly known as torque wrenches) are essential tools in producing IA screw preload. Electronic devices have been shown to be less accurate than manual devices, of which there are two basic designs: the friction (or toggle) wrench and cantilever beam wrench (Figure 2).15 Both can provide accurate and precise torque; however, both have limitations.
TOGGLE WRENCHES
The toggle wrench works by friction, commonly via an internal or external spring mechanism that pushes a ball bearing or similar device against the head of the wrench (Figure 3). When the wrench is used and the applied force (i.e., torque) exceeds the friction of the ball bearing, the head releases and a toggle effect results. The mechanisms contained within the wrench are affected by inertia as this tool is used; meaning, it must be activated slowly. This is because if the wrench is turned too quickly, it will under-deliver torque. The ideal activation time is around two to four seconds, depending on the toggle device.16
A second — and potentially more important — consideration is maintenance. When used in the oral environment, moisture will penetrate the internal spring/bearing system, which, if not cleaned and oiled after every use, can result in corrosion and malfunction (Figure 3). Research by Gutierrez et al17 has shown the potential for an under-maintained wrench to produce torque values up to 400% in error, which would definitely deform the IA screw.
This underscores the need for calibration and confirmation the torque wrench is reading correctly. A recent survey suggested 94% of implant dentists never calibrate their torque-limiting device,18 even though this is recommended by the International Organization for Standardization under its ISO 6789 standard. It is recommended that workers in all industries who use these tools check and calibrate the device at a minimum annually.

CANTILEVER BEAM WRENCHES
The cantilever beam torque wrench overcomes some of the issues presented by toggle friction-type wrenches. It has no moving parts, so it requires minimal maintenance. In addition, it is not affected by speed of activation and has lower calibration requirements compared to other types of torque wrenches.
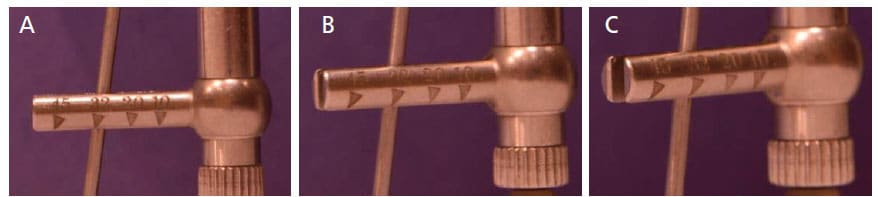
However, accuracy relies heavily on the operator being in the correct viewing position. The device is subject to parallax and torque measurement read error (MRE) — again, something accounted for in the ISO 6789 standard in the engineering world, but rarely considered in dentistry.19 An incorrect viewing position may cause MREs resulting in torque being up to 20% to 30% off the target value. This can cause clinicians to either under-torque or over-torque IA screws. To counter this, the operator must assume a viewing position that is as close to 90 degrees to both the reader arm and cantilever beam as possible (Figures 4A through 4C).
SCREW TIGHTENING TECHNIQUE
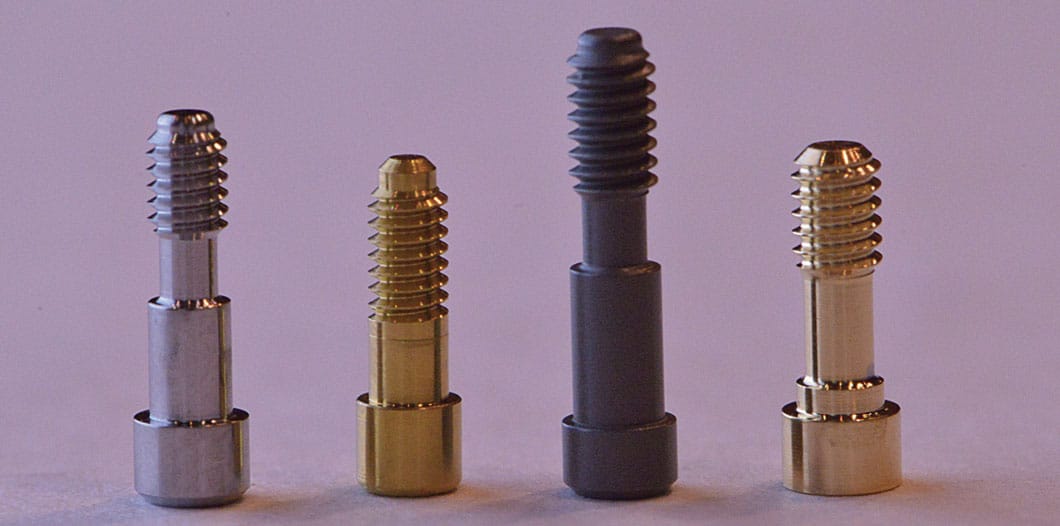
Many different techniques for screw tightening have been advocated and published in the dental literature; unfortunately, some have little merit from a scientific perspective. The concept that repeated tightening of a screw to overcome friction and improve preload relates to some screw types and is heavily dependent on the surface coating (Figure 5).
For example, 23 Kt gold-coated screws are optimally tightened by tightening to the preload target, untightening, retightening to target torque, untightening, and, finally, retightening to target torque.20 What this does is increase preload as a result of the dry-lubrication effect of the gold coating that smears off into the implant screw threads. This helps hold the screw in place. Other types of screws need only be tightened one time, and still others more than once — however, there is no need to wait five or 10 minutes between tightening events, as static friction is not governed by time.21 What is important is to confirm the abutment is correctly seated and there is no impingement of the soft tissues. Once verified, tighten the screw to the target torque. A well-made orthogonal radiograph of the IA site is essential to confirm the abutment is correctly seated within the implant at the end of the tightening procedure.22
Reuse of screws that have not failed can be considered;23 however, this is only true if the integrity of the screw is intact. Clinicians should carefully check that the surface has not been altered and the screw is not plastically deformed. Therefore, gold screws cannot be reused, as the gold wears. Additionally, screws that have loosened under load should always be replaced with new screws.
BIOLOGICAL CONSIDERATIONS
Although many IA joints fail early, often as a result of operator error,1 it is also known that the forces acting on the implant restoration change within a few weeks after placement.24 Implant restorative occlusal surfaces, especially single restorations — where bracing from other connected implants does not exist — should be designed with the aim of transmitting force through the long axis of the screw wherever possible. Shifting occlusal forces result from the cyclic function of chewing, as well as wear, erosion and attrition. Facial dento-alveolar growth and mesial drift also lead to occlusal force alterations. Thus, occlusion is dynamic — and while teeth have some ability to move and accommodate minor changes, dental implants are not capable of such compensatory movement; meaning, these alterations result in direct changes to the linearity of forces placed upon them.
These changes are noted in the literature, with up to 50% of implants adjacent to natural teeth becoming infraocclusal within five years and interocclusal contacts become lighter in as little as three months, many resulting in open contacts. Bruxing, cantilevers and cyclic loading can also lead to premature screw loosening events, especially in single-unit restorations.25
It is interesting to note, however, that IA joints can also fail after many years, which is somewhat perplexing from an engineering perspective. Although screws can develop creep, where the metal suffers plastic deformation over time, it is more likely the forces that act on the implant restoration have changed from when it was originally seated.
Research suggests continuous dentoalveolar growth development occurs throughout life. Although it is commonly reported that females stop growing after puberty around age 15 or so, and males around 21 years of age, this is incorrect. Studies evaluating tooth movement adjacent to implants have shown that adults ages 40 to 55 have similar changes compared to youths ages 15 to 21.26 These changes in occlusion will have an effect on the occlusal force placed on the implant, often increasing the lateral loading that can work to overcome the clamping forces present. It is also known that human head shape relates to anticipated growth, with brachycephalic individuals tending to grow laterally, while dolichocephalic patients experience a more anterior downward growth pattern.27
Another naturally occurring biological event is mesial drift, which is related to growth, as well as interproximal wear. As teeth have a tendency to drift forward, gaps develop adjacent to implants, resulting in lighter and sometimes open contacts in approximately 50% of cases.28 Again, with such tooth movement, the forces placed on the implant restoration will change, which can lead to failure of the IA screw joint.25
To minimize tooth movement — and thus reduce the risk of IA screw loosening — clinicians may choose to provide patients with a nighttime wear retainer (in the same manner that orthodontists stabilize the occlusion and tooth position when cases are completed). The occlusion should be regularly monitored and adjusted, as required. Should an open contact develop, it should be addressed early to prevent further biological issues, such as peri-implant disease or caries on an adjacent tooth that may occur as a result.25,28–30
CONCLUSION
Ultimately, it is likely that IA screw loosening will continue to be an issue in implant dentistry, chiefly due to the inability to control all the natural forces within an individual’s stomatological system. However, with sufficient knowledge and prudent clinical practice, the risks can be reduced. Adopting this approach will help produce healthier implants sites, minimize complications, prevent material fracture and wear, and contribute to successful long-term outcomes.
Key Takeaways
- Loosening of the implant/abutment (IA) screw is a common complication in implant dentistry, and these issues can range from a straightforward fix, such as retightening the screw, to catastrophic failure and breakage of the joint components.
- The risk of screw loosening can be greatly reduced by understanding how the screw system works, using appropriate materials (i.e., components) and tools, and regularly monitoring the implant restoration so clinicians can mitigate the forces that act upon it.
- Three common reasons for screw loosening involve operator error,1 mechanical misfit, and biological changes within the patient’s stomatological system.
- When tightening screws, torque-limiting devices are essential to achieving the manufacturer-specified torque value.
- Torque wrenches must be used and maintained correctly to ensure correct screw torque. Additionally, the screw’s surface coating dictates the proper screw tightening protocol.
- As a means of mitigating IA screw loosening, implant restorative occlusal surfaces should be designed with the aim of transmitting force through the long axis of the screw wherever possible.
- To minimize tooth movement — and thus reduce the risk of screw loosening — clinicians may wish to provide patients with a nightguard.
- With sufficient knowledge and prudent clinical practice, the risk of IA screw loosening can be minimized.
REFERENCES
- Bickford JH. An Introduction to the Design and Behavior of Bolted Joints. Boca Raton, Fla: CRC Press; 1995.
- Rybczynski W. One Good Turn. A Natural History of the Screwdriver and the Screw. New York, NY: Scribner; 2005.
- Katsavochristou A, Koumoulis D. Incidence of abutment screw failure of single or splinted implant prostheses: A review and update on current clinical status. J Oral Rehabil. 2019;46:776–786.
- Goodacre BJ, Goodacre SE, Goodacre CJ. Prosthetic complications with implant prostheses (2001–2017). Eur J Oral Implantol. 2018;11(Suppl 1):S27–S36.
- Jung RE, Pjetursson BE, Glauser R, et al. A systematic review of the 5-year survival and complication rates of implant-supported single crowns. Clin Oral Implants Res. 2008;19:119–130.
- Kourtis S, Damanaki M, Kaitatzidou S, Kaitatzidou A, Roussou V. Loosening of the fixing screw in single implant crowns: predisposing factors, prevention and treatment options. J Esthet Restor Dent. 2017;29:233–246.
- Huang Y, Wang J. Mechanism of and factors associated with the loosening of the implant abutment screw: A review. J Esthet Restor Dent. 2019;31:338–345.
- Coefficient of Friction. Available at: http/://www.vedantu.com/physics/coefficient-of-friction. Accessed December 8, 2022.
- Pia NG, Hess DP. Dynamic loosening of threaded fastners. Noise and Vibration Worldwide. 2004;35:13–19.
- Hurson S. Use of authentic, integrated dental implant components vital to predictability and successful long-term clinical outcomes. Compend Contin Educ Dent. 2016;37:450–455.
- Karl M, Irastorza-Landa A. In vitro characterization of original and nonoriginal implant abutments. Int J Oral Maxillofac Implants. 2018;33:1229–1239.
- Berberi A, Maroun D, KanJ W, Amine EZ, Philippe P. Micromovement evaluation of original and compatible abutments at the implant-abutment interface. J Contemp Dent Pract. 2016;17:907–913.
- Tallarico M, Fiorellini J, Nakajima Y, Omori Y, Takahisa L, Canullo L. Mechanical outcomes, microleakage, and marginal accuracy at the implant-abutment interface of original versus nonoriginal implant abutments: A systematic review of in vitro studies. Biomed Res Int. 2018;2018:2958982.
- Hill EE, Phillips SM, Breeding LC. Implant abutment screw torque generated by general dentists using a hand driver in a limited access space simulating the mouth. J Oral Implantol. 2007;33:277–279.
- Albayrak H, Gumus HO, Tursun F, Kocaagaoglu HH, Kilinc HI. Accuracy of torque-limiting devices: A comparative evaluation. J Prosthet Dent. 2017;117:81–86.
- Wadhwani CPK, Frantz WT, Schoenbaum TR, Rosen PS, Nhan D, Chung KH. Effect of activation rate on output torque values from a dental implant toggle-style torque wrench. J Prosthet Dent. September 2, 2021. Epub ahead of print.
- Gutierrez J, Nicholls JI, Libman WJ, Butson TJ. Accuracy of the implant torque wrench following time in clinical service. Int J Prosthodont. 1997;10:562–567.
- Wadhwani CP, Rosen PS, Yang G, et al. Survey of dental clinicians for attitude and use of torque-limiting devices. Int J Oral Maxillofac Implants. 2021;36:538–545.
- Wadhwani CPK, O’Brien R, Rosen PS, Chung KH. Effect of viewing angles on measurement errors when using an implant cantilever beam torque-limiting device. J Prosthet Dent. January 4, 2022. Epub ahead of print.
- Alnasser AH, Wadhwani CPK, Schoenbaum TR, Kattadiyil MT. Evaluation of implant abutment screw tightening protocols on reverse tightening values: An in vitro study. J Prosthet Dent. 2021;125:486–490.
- Dusto A. Static Friction: Definition, Coefficient & Equation (w/Examples). Available at: https://sciencing.com/static-friction-definition-coefficient-equation-w-examples-13720447.html. Accessed December 8, 2022.
- Lin KC, Wadhwani CP, Cheng J, Sharma A, Finzen F. Assessing fit at the implant-abutment junction with a radiographic device that does not require access to the implant body. J Prosthet Dent. 2014;112:817–823.
- Xiao H, Yang Y, Liu Z, Taylor TD. Opinions regarding reuse or replacement of implant prosthesis retaining screws: A systematic review. Int J Oral Maxillofac Implants. 2017;32:985–991.
- Kim YJ, Ko KH, Huh YH, Cho LR, Park CJ. Initial change in the occlusal force and occlusal contact area following single molar implant restoration. Int J Oral Maxillofac Implants. 2021;36:1139–1146.
- Varthis S, Tarnow DP, Randi A. Interproximal open contacts between implant restorations and adjacent teeth. Prevalence — causes — possible solutions. J Prosthodont. 2019;28:e806–e810.
- Bernard JP, Schatz JP, Christou P, Belser U, Kiliaridis S. Long-term vertical changes of the anterior maxillary teeth adjacent to single implants in young and mature adults. A retrospective study. J Clin Periodontol. 2004;31:1024–1028.
- Oesterle LJ, Cronin Jr RJ. Adult growth, aging, and the single-tooth implant. Int J Oral Maxillofac Implants. 2000;15:252–260.
- Latimer JM, Gharpure AS, Kahng JH, Aljofi FE, Daubert DM. Interproximal open contacts between implant restorations and adjacent natural teeth as a risk-indicator for peri-implant disease — a cross-sectional study. Clin Oral Implants Res. 2021;32:598–607.
- Greenstein G, Carpentieri J, Cavallaro J. Open contacts adjacent to dental implant restorations: etiology, incidence, consequences, and correction. J Am Dent Assoc. 2016;147:28–34.
- Koori H, Morimoto K, Tsukiyama Y, Koyano K. Statistical analysis of the diachronic loss of interproximal contact between fixed implant prostheses and adjacent teeth. J Prosthodont. 2010;23:535–540.
From Decisions in Dentistry. January 2023;9(1)10,13-14,16.
