

Recession Defects on a Maxillary Single Tooth Implant
This case study looks at a treatment plan to successfully treat this fairly common implant complication.
Single implant restorations have become an integral part of the contemporary dental practice. With the increasing number of implants placed over the past decade, the incidence of implant complications has also increased. One of the most common complications associated with a maxillary anterior dental implant is the development of a mid-facial recession.1,2
A systematic review showed that advanced mid-facial recessions (≥ 1.0 mm) were seen in up to 64% of immediate implant therapy cases.3 The midfacial recession associated with implant restorations seems to be a common sequela of the implant positioning into the alveolus.4 The anatomy of the premaxilla commonly includes a concavity on the facial aspect and implants are usually placed with an orientation to avoid an apical perforation of the ridge.5
Consequences of a poorly angulated implant in the esthetic zone include the unwanted over-contouring of the abutment and the crown that puts pressure on the facial tissue, leading to gingival recession.6 The treatment approach to correct these defects hinges on the decision of whether to save or remove the implant; this decision is especially critical if the implant is located in the esthetic zone. Treatment also must consider the three-dimensional (3D) implant position, periodontal condition of the implant, and availability of the implant component.
Clinical Case
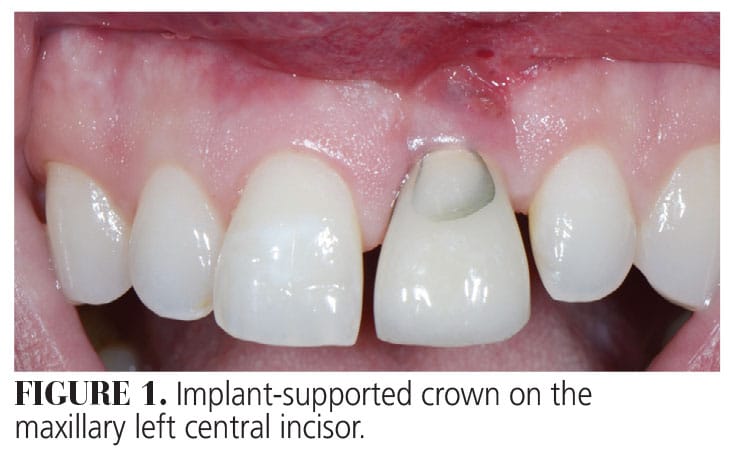 Patient A was referred to our dental office for evaluation of a single implant-supported crown that replaced his maxillary left central incisor (Figure 1). His chief complaint was the unesthetic appearance when he smiled, spaces between his teeth, and orientation and shape of his teeth. Furthermore, the patient complained about the chipped porcelain on his implant-supported crown.
Patient A was referred to our dental office for evaluation of a single implant-supported crown that replaced his maxillary left central incisor (Figure 1). His chief complaint was the unesthetic appearance when he smiled, spaces between his teeth, and orientation and shape of his teeth. Furthermore, the patient complained about the chipped porcelain on his implant-supported crown.
Patient A’s natural tooth was lost after an endodontic procedure failed and he was treated with an immediate implant placement after tooth extraction. This entire dental treatment was performed overseas in 2007, therefore any information regarding the implant (type, size) was not available.
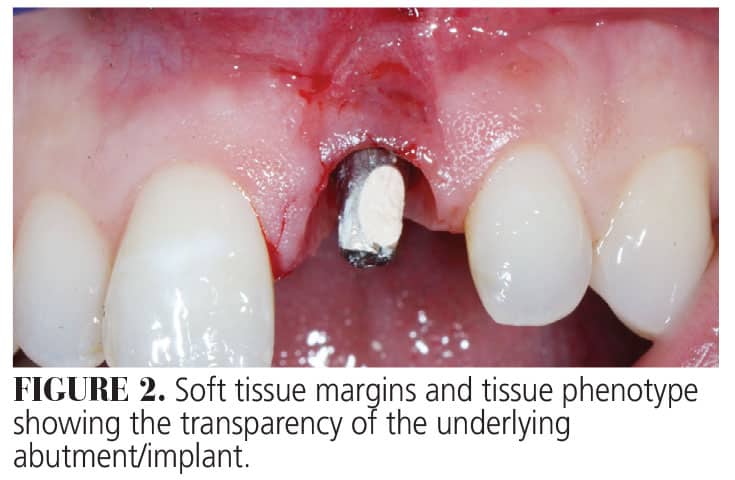
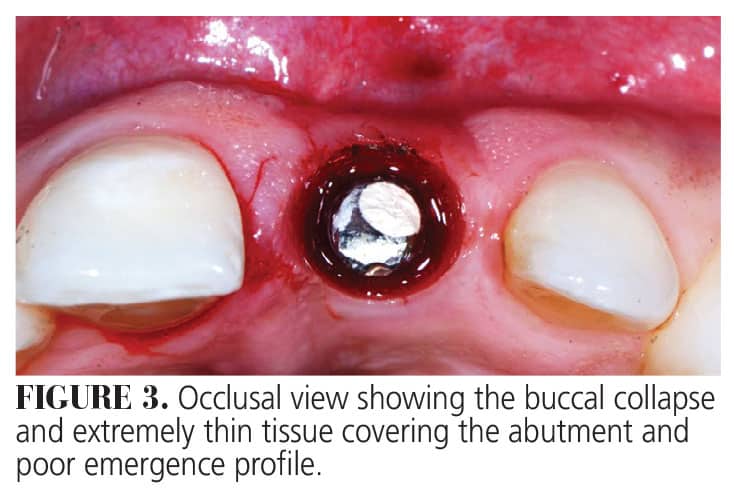
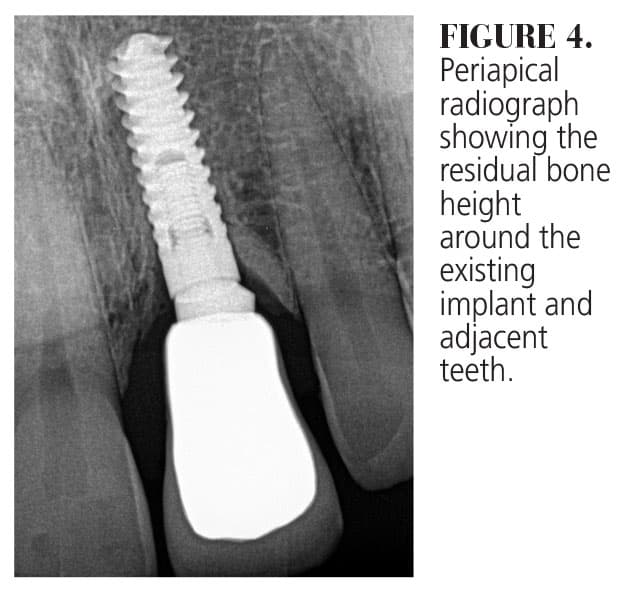
The patient’s medical history revealed no systemic contraindications for dental treatment. Clinical examination showed a thin tissue phenotype, with the gingival margin of the implant in a more apical position with respect to the adjacent natural teeth. The tissue was very thin, allowing the underlying grayish hue of the implant surface to be visible (Figure 2). In addition to the horizontal soft tissue deficiency, there was inadequate emergence profile of the implant abutment (Figure 3). Fortunately, radiographic examination determined that interproximal bone loss around the implant and the adjacent teeth was minimal. In addition, no signs of any peri-implant issues were present (Figure 4).
 The primary treatment goals were to reduce the soft tissue deficiency (vertically and horizontally), eliminate the soft tissue discrepancy between the implant restoration and the right central incisor, and place a new crown over the implant. The plan also included changing position and angulation of the maxillary anterior teeth as well as their shape as the patient desired squarer-looking teeth. Furthermore, the tissue thickness over the implant was to be increased to mask the implant/abutment.
The primary treatment goals were to reduce the soft tissue deficiency (vertically and horizontally), eliminate the soft tissue discrepancy between the implant restoration and the right central incisor, and place a new crown over the implant. The plan also included changing position and angulation of the maxillary anterior teeth as well as their shape as the patient desired squarer-looking teeth. Furthermore, the tissue thickness over the implant was to be increased to mask the implant/abutment.
Provisional Prosthetic Phase. The implant crown restoration was removed 2 weeks before the surgery. As no parts were available, the already existing abutment was modified to diminish its buccal inclination. Then a properly contoured provisional polymethyl methacrylate (PMMA) crown was fabricated and cemented with temporary cement. This would remain in place for several months to allow the buccal and interproximal soft tissue time to fill the space previously occupied by the existing porcelain crown.
Surgical Protocol. The soft tissue defect was treated with a modified coronally advanced tunnel technique including a connective tissue graft (CTG) harvested from the tuberosity. Following local anesthesia, a poach was created with a modified orban knife on the facial aspect of the implant abutment, preserving the interdental papillae. The flap was raised in a split thickness approach in a coronal apical direction to permit the coronal displacement. Careful dissection was performed to avoid thinning of the buccal flap (Figure 5). The connective tissue was harvested from the tuberosity via a table-top technique and inserted into the pouch. The graft and the flap were stabilized with sling sutures around the cingulum of the temporary crown (Figure 6).


Postsurgical Infection Control. The patient was prescribed antibiotics (amoxicillin plus clavulanic acid 875/125 mg) starting 1 hour before the surgery and for the next 7 days. In addition, one tablet of Ibuprofen (800 mg) and 8 mg of dexamethasone were given 1 hour before the surgery to mitigate any edema in the surgical area (due to the patient’s position working with clients). The anti-inflammatory medication (ibuprofen, 600 mg) was recommended every 6 hours for 5 days, while the dexamethasone was given as directed for 3 days.
The patient was instructed to avoid brushing the surgical site but to rinse with 0.12 % chlorhexidine solution three times a day. The sutures were removed 3 weeks after the surgery. Plaque control was maintained by continuing the use of chlorhexidine rinse for another 2 weeks. After this period, the patient was instructed to start mechanical plaque control with a ultrasoft surgical brush in a roll technique for another month. The patient was then scheduled for a recare prophylaxis every 3 months.
Prosthetic Protocol. Five months after the surgery, the patient underwent orthodontic treatment on the maxillary arch only, which lasted for 6 months. The healed surgical site soft tissue was consistent in color and texture with the surrounding area (Figure 7). After completion of the orthodontic treatment, the original abutment was scanned and new hybrid zirconia coping was made to fit over it, transforming it to a hybrid abutment (Figure 8).


A new PMMA temporary crown was made to fit over this hybrid abutment. The increase in the size of the hybrid zirconia abutment compressed the soft tissue between the implant abutment and the adjacent teeth, providing a new finish line for a provisional crown. At the same time, per the patient’s request, two no-prep veneers were made for the lateral incisors to give his smile more of a square look. The change in the emergence profile, together with the newly resorted contact points, provided support for the interdental papillae.
 Final prosthetic treatment was completed 1 year after the periodontal surgery. A new impression was taken and a new lithium disilicate restoration was used to rehabilitate the patient to the new correct emergence profile. At the patient’s request, a small diastema was created between the two maxillary central incisors (Figure 9).
Final prosthetic treatment was completed 1 year after the periodontal surgery. A new impression was taken and a new lithium disilicate restoration was used to rehabilitate the patient to the new correct emergence profile. At the patient’s request, a small diastema was created between the two maxillary central incisors (Figure 9).
Discussion
In this case report, a dental implant was saved that had developed a midfacial recession in the esthetic zone. The decision to save the implant was based on the following:
- Implant was in a restorable position.
- Implant was healthy.
- No radiographic bone loss was present interproximally or on the facial aspect of the existing implant.
- Implant was placed at the correct 3D position.
- Existing abutment could be used as a base to form a new hybrid (metal-zirconia abutment).
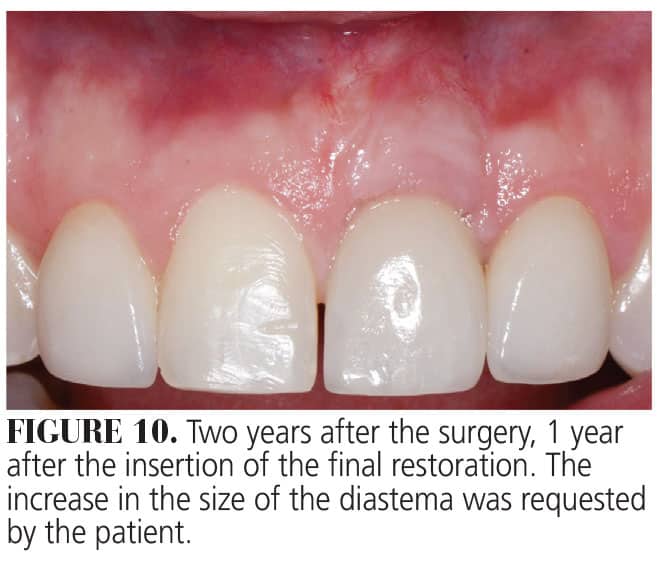 The soft tissue deficiency in both the horizontal and vertical direction was corrected with a modified coronally advanced tunnel and CTG. One year after treatment, the gingival margin was at the same level and color as the adjacent central incisor. Patient A requested that the diastema be enlarged; this was completed. (Figure 10) Furthermore, the increase in the tissue thickness on the buccal aspect of the implant was sufficient to mask the gray hue from the implant/abutment and also allowed for a correct emergence profile of the implant-supported crown. The CTG was harvested from the tuberosity.
The soft tissue deficiency in both the horizontal and vertical direction was corrected with a modified coronally advanced tunnel and CTG. One year after treatment, the gingival margin was at the same level and color as the adjacent central incisor. Patient A requested that the diastema be enlarged; this was completed. (Figure 10) Furthermore, the increase in the tissue thickness on the buccal aspect of the implant was sufficient to mask the gray hue from the implant/abutment and also allowed for a correct emergence profile of the implant-supported crown. The CTG was harvested from the tuberosity.
Advantages of this technique include an easy harvesting method and the presence of a low fatty tissue in the graft while providing a supply of rich connective tissue.7–9 The CTG may act as a biological filler, improving the adaptation and stability of the flap to the root during early wound repair.10 As a result, the gingival phenotype becomes thicker and the potential of achieving complete root coverage is higher. However, it is still unclear how much the composition of the graft influences the outcomes of mucogingival surgery. Limited evidence suggests that CTG impacts soft tissue thickness and keratinized tissue width while having no effect on the amount of root coverage.11,12 One of the drawbacks of the connective tissue harvested from the tuberosity is the possibility of an unesthetic hyperplastic response in cases with a thick phenotype or when esthetics is a concern.13
The 3D implant position is critical for saving an implant. If the implant is placed in a nonrestorable position, surgical procedures cannot correct the esthetic problems. The implant placement in the correct apico-coronal position is critical for the resultant restoration to be functional and esthetic. The biological width around the implant should be 3 to 4 mm in apico-coronal direction, accounting for 2 mm of junctional epithelium and 1 to 2 mm of connective tissue attachment.14 In this case, the implant platform was about 3 mm from the gingival margin.
Conclusion
Digital dentistry provided a solution to the lack of the implant component parts in this case. A hybrid abutment was created by scanning the original abutment and then fabricating a new retrofit abutment with the proper alignment to accept a new restoration. The original abutment was used as a hybrid abutment base on which the zirconia mesostructure was bonded in the laboratory with multilink abutment cement. The postsurgical replacement of the temporary crown played a critical role in the conditioning of the soft tissue — not only on the buccal aspect but also interproximal, facilitating the growth of the interdental papillae.
This case study showed the possibility of correcting a severe horizontal and vertical soft tissue deficiency and achieving a highly esthetic result and patient satisfaction. This case illustrates the advantages of using an interdisciplinary approach using three different disciplines (periodontal-orthodontic-restorative) to properly diagnose and treat this patient, resulting in a positive outcome, both functionally and esthetically.
References
- Cheng Q, Su YY, Wang X, Chen S. Clinical outcomes following immediate loading of single-tooth implants in the esthetic zone: a systematic review and meta-analysis. Int J Oral Maxillofac Implants. 2020;35:167-177.
- Chen ST, Buser D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla — a systematic review. Int J Oral Maxillofac Implants. 2014;29(Suppl):186-215.
- Cosyn J, Hooghe N, De Bruyn H. A systematic review on the frequency of advanced recession following single immediate implant treatment. J Clin Periodontol. 2012;39:582-589.
- Cosyn J, Sabzevar MM, De Bruyn H. Predictors of inter-proximal and midfacial recession following single implant treatment in the anterior maxilla: a multivariate analysis. J Clin Periodontol. 2012;39:895-903.
- Hwang KG, Park CJ. Ideal implant positioning in an anterior maxillary extraction socket by creating an apico-palatal guiding slot: a technical note. Int J Oral Maxillofac Implants. 2008;23:121-122.
- Su H, Gonzalez-Martin O, Weisgold A, Lee E. Considerations of implant abutment and crown contour: critical contour and subcritical contour. Int J Periodontics Restorative Dent. 2010;30:335-343.
- Zuhr O, Baumer D, Hurzeler M. The addition of soft tissue replacement grafts in plastic periodontal and implant surgery: critical elements in design and execution. J Clin Periodontol. 2014;41(Suppl 15):S123-142.
- Roccuzzo M, Dalmasso P, Pittoni D, Roccuzzo A. Treatment of buccal soft tissue dehiscence around single implant: 5-year results from a prospective study. Clin Oral Investig. 2019;23:1977-1983.
- Sanz-Martin I, Rojo E, Maldonado E, Stroppa G, Nart J, Sanz M. Structural and histological differences between connective tissue grafts harvested from the lateral palatal mucosa or from the tuberosity area. Clin Oral Investig. 2019;23:957-964.
- Cairo F, Cortellini P, Pilloni A, et al. Clinical efficacy of coronally advanced flap with or without connective tissue graft for the treatment of multiple adjacent gingival recessions in the aesthetic area: a randomized controlled clinical trial. J Clin Periodontol. 2016;43:849-856.
- Amin PN, Bissada NF, Ricchetti PA, Silva APB, Demko CA. Tuberosity versus palatal donor sites for soft tissue grafting: A split-mouth clinical study. Quintessence Int. 2018;49:589-598.
- Rojo E, Stroppa G, Sanz-Martin I, Gonzalez-Martin O, Alemany AS, Nart J. Soft tissue volume gain around dental implants using autogenous subepithelial connective tissue grafts harvested from the lateral palate or tuberosity area. A randomized controlled clinical study. J Clin Periodontol. 2018;45:495-503.
- Tavelli L, Bacootchi S, Greenwell H, Wang H Is a sorf tissue graft harvested from the maxillary tuberosity the approach of choice in an isolated site? J Periodontol. 2019;90:821-825.
- Berglundh T, Lindhe J. Dimension of the periimplant mucosa. Biological width revisited. J Clin Periodontol. 1996;23:971-973.
From Decisions in Dentistry. March 2024; 10(2):16-19
