
 FLOORTJE / E+/ GETTY IMAGES PLUS
FLOORTJE / E+/ GETTY IMAGES PLUS
Preventing Oral Diseases With Biomimetic Hydroxyapatite
This overview presents clinical applications for hydroxyapatite in managing caries, erosion, periodontal disease and dentinal hypersensitivity.
The Global Burden of Oral Diseases study demonstrated that good oral health is essential to maintaining systemic health, and is a determining factor in quality of life.1 Oral diseases are a major global health issue owing to their high prevalence and incidence in all regions.1 Without proper oral care, pathogens can reach levels that might lead to oral infections, such as dental caries and periodontal disease.2 Caries and periodontal conditions are the most common oral diseases across the globe.3 This underscores the importance of developing effective prevention and management strategies to reduce the burden of oral conditions.
As part of preventive self-care, selection of appropriate products for the individual patient is key to optimal oral health. For example, toothpaste is widely used for the delivery of active substances that help prevent caries and support periodontal health. These agents reduce and prevent plaque, calculus, gingivitis, oral malodor, dentinal hypersensitivity and erosion, while also facilitating removal and prevention of extrinsic stain.4 However, toothpastes are complex formulations with varying ingredients and active substances.4 Fluoride compounds are often used for caries prevention and remineralization.4 For this reason, fluorides have been the standard in caries prevention studies to assess and quantify the efficacy of new active substances.
That noted, some countries limit the amount of fluoride in toothpaste, as it is considered toxic in higher concentrations and can cause fluorosis in children.4 Recently, due to the similarity of hydroxyapatite (HAP) to the crystallites in enamel, synthetic HAP has gained attention as a biomimetic agent used in preventive oral care products for all age groups. This article presents an overview of applications for HAP, and the clinical studies that support its use for controlling caries, erosion, periodontal disease and dentinal hypersensitivity.
A biomimetic agent is a substance, device or system that can actively stimulate or direct specific cellular or tissue responses, or both, for the purpose of achieving tissue repair, regeneration, or control of diseases by mimicking natural biological processes.5 These agents have the advantage of enhancing the natural biological process to achieve the targeted goal at a faster rate. An example is the biomimetic remineralization of caries in enamel using HAP toothpaste, gel or mouthrinse. In addition to providing calcium and phosphate ions, the HAP nanoparticles penetrate the lesion’s micropores, and templates de novo HAP crystallites form around each particle by attracting calcium and phosphate ions from the surrounding solution into the tooth tissue, thus promoting crystal integrity and growth.6 This biomimetic mineralization process enables the regeneration of enamel and dentin. Myriad studies have shown its clinical efficacy against caries, dental erosion, dentinal hypersensitivity and other clinical concerns in preventive dentistry.7 The concentration of calcium phosphates used is not limited since there is no risk of fluorosis in children if swallowed.7,8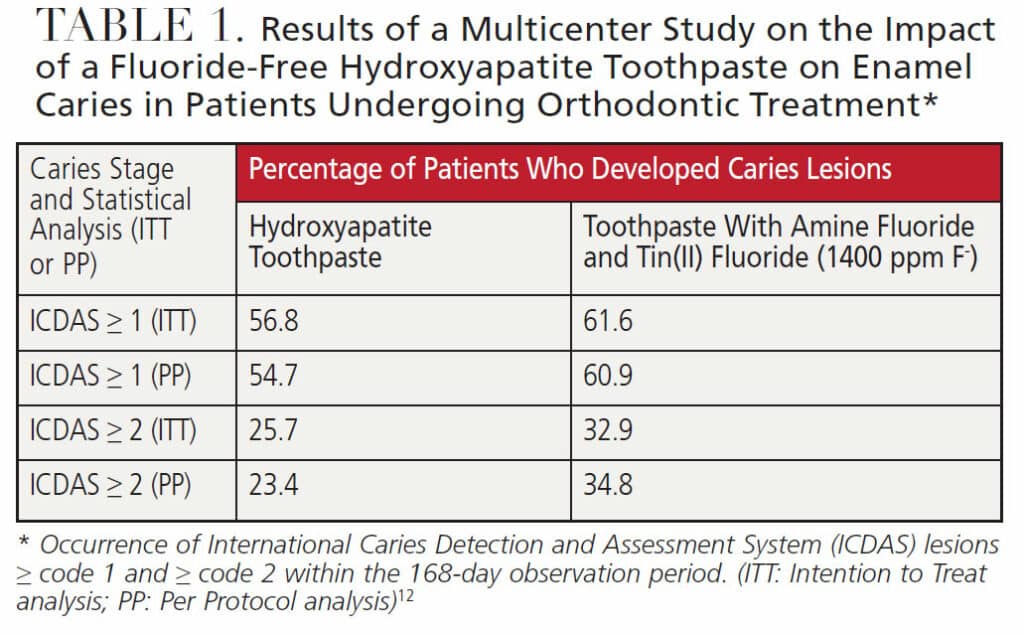
APPLICATIONS FOR PREVENTION
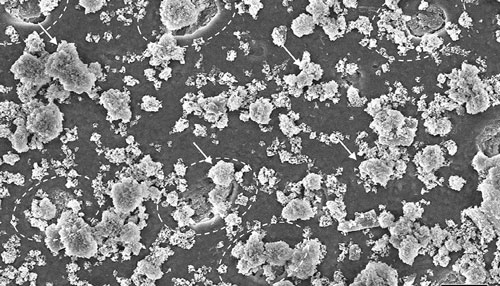
Among the synthetic calcium phosphates used in oral care products, HAP has the highest structural and chemical similarity to the enamel crystallites in teeth, and, as such, offers high biocompatibility and potential to interact with tooth surfaces. It is therefore classified as a biomimetic active substance.7,9 Although the crystallites of synthetic HAP used in toothpastes, gels and rinses are similar chemically and dimensionally to natural HAP in enamel, the crystallites in enamel are oriented in parallel, forming the prismatic and interprismatic enamel. By comparison, the crystallites of synthetic HAPs are densely packed, yet lack an apparent preferential spatial orientation; rather, they aggregate in random orientations to form stable, mostly spherical, clusters.10 The first clinical studies of HAP in oral disease prevention were published in the 1980s,11 and there has been a significant increase in the number of publications in recent years.7,9
REMINERALIZATION AND CARIES PROTECTION
A considerable number of research studies supporting HAP’s clinical efficacy have been published in the past few years.9,12,13 A recent multicenter, randomized clinical trial reported that HAP in toothpaste is a clinically relevant biomimetic alternative to fluorides in caries prevention in patients at high caries risk.12 The study demonstrated that a fluoride-free HAP toothpaste is “non-inferior” to a toothpaste with amine fluoride and tin(II) fluoride in respect to prevention of caries in patients undergoing orthodontic treatment (Table 1).12 Patients with fixed orthodontic appliances are known to have an increased risk of caries due to plaque retention around brackets. It was suggested that HAP toothpaste may be particularly relevant for patients with fixed orthodontic appliances considering that a previous study showed HAP can penetrate dental plaque and serve as a potential source of calcium and phosphate, as well as an acid buffer.14 The presence of calcium and phosphate ions would obviously minimize demineralization and promote remineralization.
When calcium and phosphate ions accumulate on enamel surfaces, enamel dissolution will be inhibited by the common ion effect. At the same time, the ions diffuse through the enlarged pores of the demineralized enamel into the solution phase between the crystallites. As the concentration of these ions increases, crystal growth (remineralization) may occur on the surface of the partially dissolved crystallites.15 Another clinical trial demonstrated the clinical non-inferiority of HAP toothpaste to a fluoride toothpaste in the prevention of early childhood caries.13 Other studies have provided evidence of remineralization of early caries lesions and protection against demineralization with HAP-based formulations.16–18 Compared with fluoride, in situ research has shown that HAP remineralizes subsurface layers of early caries lesions, while fluoride primarily remineralizes the surface layer.16
In addition to toothpastes, higher concentrated HAP gels can be used as a supplement for intensive remineralization overnight. High-dose fluoride gels indicated for the same purpose are classified as drugs and may be applied, at most, once a week, while HAP gels can be applied daily.17 This means that even children under the age of 6 can use HAP gels.
EFFICACY AGAINST DENTAL EROSION
Dental erosion is the loss of dental hard tissue through chemical etching and dissolution by acids of nonbacterial origin. Sources of the acid may be acidic beverages, foods and drugs, or gastric juice contacting the teeth due to medical conditions, such as reflux diseases and bulimia. Overzealous toothbrushing may also cause tooth wear. As noted, HAP in oral care products can serve as a reservoir for calcium and phosphate ions, and as an acid buffer, thus reducing demineralization and promoting remineralization.14 Furthermore, studies have shown that HAP forms a protective layer on eroded tooth surfaces that protects against subsequent acid attack.10,18–20 An Italian research group showed that eight weeks of in vivo application of a HAP toothpaste resulted in the formation of a protective layer that was not observed when using the fluoride control toothpaste.20
MANAGING GINGIVITIS AND PERIODONTITIS
Another focus in oral healthcare is the prevention of gingivitis and periodontitis. Toothpastes and mouthrinses with potent antibacterial substances, such as tin(II) salts21 and chlorhexidine,22 are often recommended for prevention of periodontal disease during self-care. However, these do not simply kill harmful bacteria; they also kill commensal microorganisms. This may cause a shift in the ecological balance of the oral microbiota, which, in turn, may favor inflammation. Furthermore, some of these active substances, especially tin and chlorhexidine, can stain the tooth surfaces and tongue, which can significantly reduce patient compliance.23 For this reason, there is a high demand for alternative active substances and concepts — such as HAP — that minimize bacterial adhesion on tooth surfaces without interfering with the ecological balance.24
A 12-week, multicenter randomized clinical trial investigated the impact of the combined use of a HAP toothpaste and clinical prophylaxis in patients with periodontitis.25 Significant improvements in plaque control and bleeding on probing were reported after 12 weeks (Table 2). There was no clinically significant difference in efficacy observed between the HAP toothpaste and a control toothpaste with amine fluoride and tin(II) fluoride.
One may argue that professional prophylaxis made the difference rather than the agents applied to the teeth. However, a clinical study demonstrated that a mouthrinse containing only water and HAP minimized the initial bacterial colonization of enamel surfaces just as effectively as the gold standard 0.2% chlorhexidine.24 The authors attribute this to HAP’s ability to induce coaggregation of bacteria in saliva and plaque. Acting as a so-called “bacterial magnet,” this improved periodontal health by reducing bacterial colonization of tooth surfaces while also promoting their clearance from the oral cavity via salivary action.24
Besides reducing microbial adhesion on teeth by inducing bacterial coaggregation, the use of HAP helps maintain the ecological balance of the oral microbiota — with the added benefit of not staining oral tissues. Instead of staining, the use of HAP can result in teeth appearing brighter (i.e., a whitening effect).26 For these reasons, it is recommended to only prescribe chlorhexidine mouthrinse if specifically indicated.
REDUCING DENTINAL HYPERSENSITIVITY
Hypersensitivity due to exposed dentin is highly prevalent and can severely limit quality of life. Worn enamel and gingival recession are the main causes of dentin exposure. A study of HAP toothpaste for the treatment of hypersensitive exposed roots showed that 60%, 90% and 5% of the subjects reported significant improvement in symptoms after few days of using the toothpaste containing HAP (Ø grain size 6 µm), HAP (Ø grain size 2 µm), and a placebo, respectively.11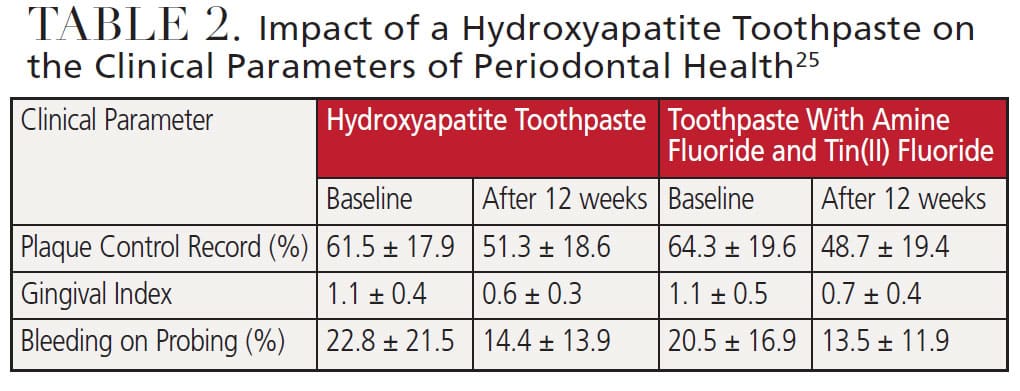
Another randomized clinical trial tested the desensitizing effects of a toothpaste containing HAP particles against a toothpaste with potassium nitrate (KNO3).27 Compared with the KNO3 toothpaste, HAP toothpaste was significantly more effective, as measured with an air syringe test (a 46.0% reduction with HAP versus 29.4% with KNO3), and subjective testing (47.5% versus 28.1%). Relative to the placebo, significant effects were documented for both toothpastes after just four weeks. In terms of action, KNO3 reduces sensitivity by numbing the tooth nerve, while HAP occludes exposed dentinal tubules and blocks transmission of the pain stimulus (Figure 1).28 Sensitivities associated with professional bleaching with peroxides have reportedly been relieved with HAP formulations.26
Besides HAP and KNO3, other active substances are used in toothpaste and mouthrinse to reduce dentinal hypersensitivity. These include calcium sodium phosphosilicate, arginine, fluorides and strontium salts. A current meta-analysis concluded that toothpastes with HAP are more effective in relieving sensitivity than other active substances after both two weeks and four weeks of use.29 The meta-analysis summarized that HAP and arginine can be recommended as active substances for relieving dentinal hypersensitivity, with HAP showing the greater desensitizing effect.29
CASE REPORTS
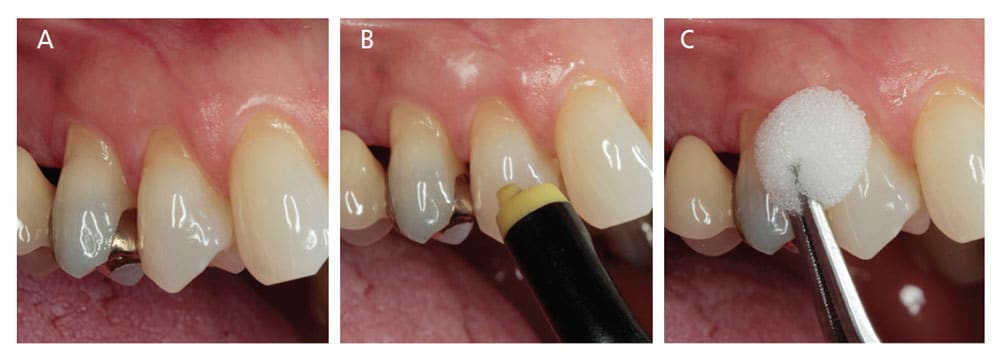
In Case Report 1, a 44-year-old female presented for prophylaxis. Gingival recessions were visible on teeth #4, 5 and 6. The patient reported experiencing occasional hypersensitivity, which was confirmed with an air syringe and ice. The application of HAP gel was recommended following toothbrushing (Figures 2A through 2C). The patient presented again after four weeks, and these symptoms were significantly reduced. There was no long-term follow-up.
In Case Report 2, a 36-year-old female presented for prophylaxis and reported experiencing severe hypersensitivity that was negatively affecting her quality of life (Figures 3A through 3C). Daily use of HAP gel after toothbrushing was recommended. The patient presented again after four weeks, and these symptoms were significantly reduced. There was no long-term follow-up.
CONCLUSIONS
In light of the foregoing analysis, the authors offer the following conclusions:
- HAP can be used in dental care for all age groups and is not subject to any restrictions in concentration or frequency of application.
- Results of various studies confirm the clinical efficacy of HAP in the prevention and management of caries, erosion and periodontal disease.
- A meta-analysis of clinical studies shows that toothpastes with HAP are equally or more effective than those with other active substances in reducing dentinal hypersensitivity.
- This biomimetic agent acts in a number of beneficial ways, including reducing bacterial adhesion on tooth surfaces without interfering with the ecological balance of the oral flora.
- It also serves as a source of calcium and phosphate ions, and as an acid buffer in cariogenic biofilms, thus further supporting HAP’s use in caries management and periodontal applications.
Due to its many indications in clinical dentistry and self-care, biomimetic HAP holds significant promise in the prevention and management of oral challenges. By mimicking natural biological processes, this agent supports a balanced oral microbiome while simultaneously promoting remineralization and optimal oral health.
KEY TAKEAWAYS
- Due to the similarity of hydroxyapatite (HAP) to the crystallites in enamel, synthetic HAP has gained attention as a biomimetic active ingredient used in preventive oral care products for all age groups.
- Various clinical studies support the use of HAP for controlling dental caries, erosion, periodontal disease and dentinal hypersensitivity.
- As a biomimetic agent, HAP helps promote the regeneration of enamel and dentin.
- Besides reducing microbial adhesion on teeth by inducing bacterial coaggregation, the use of HAP helps maintain the ecological balance of the oral microbiota — with the added benefit of not staining oral tissues.
- Due to its many indications in clinical dentistry and self-care, biomimetic HAP holds significant promise in the prevention and management of global oral health challenges.
The authors disclose either working for, or having received financial research support from, Dr. Kurt Wolff GmbH & Co. KG.
REFERENCES
- Jin LJ, Lamster IB, Greenspan JS, Pitts NB, Scully C, Warnakulasuriya S. Global burden of oral diseases: emerging concepts, management and interplay with systemic health. Oral Dis. 2016;22:609–619.
- Wade WC. The oral microbiome in health and disease. Pharmacol Res. 2013;69:137–143.
- Frencken JE, Sharma P, Stenhouse L, Green D, Laverty D, Dietrich T. Global epidemiology of dental caries and severe periodontitis — a comprehensive reviewJ J Clin Periodontol. 2017;44:S94–S105.
- van Loveren C. Preventive dentistry 1. Fluoride toothpaste, the cornerstone of caries prevention. Ned Tijdschr Tandheelkd. 2016;123:601–608.
- Vincent JF, Bogatyreva OA, Bogatyrev NR, Bowyer A, Pahl AK. Biomimetics:its practice and theory. J R Soc Interface. 2006;3:471–482.
- Amaechi BT, van Loveren C. Fluorides and non-fluoride remineralization systems. Monogr Oral Sci. 2013;23:15–26.
- Enax J, Fabritius H-O, Fabritius-Vilpoux K, Amaechi BT, Meyer F. Modes of action and clinical efficacy of particulate HAP in preventive oral health care — state of the art. Open Dent J. 2019;13:274–287.
- Epple M. Review of potential health risks associated with nanoscopic calcium phosphate. Acta Biomater. 2018;77:1–14.
- Meyer F, Enax J, Amaechi BT, et al. Hydroxyapatite as remineralization agent for children’s dental care. Front Dent Med. 2022;3:859560.
- Fabritius-Vilpoux K, Enax J, Herbig M, Raabe D, Fabritius H-O. Quantitative affinity parameters of synthetic HAP and enamel surfaces in vitro. Bioinspir Biomim Nan. 2019;8:141–153.
- Hüttemann RW, Dönges H. Untersuchungen zur Therapie überempfindlicher Zahnhälse mit Hydroxylapatit. Dtsch Zahnärztl Z. 1987;42:486–488.
- Schlagenhauf U, Kunzelmann KH, Hannig C, et al. Impact of a non-fluoridated microcrystalline HAP dentifrice on enamel caries progression in highly caries-susceptible orthodontic patients: A randomized, controlled 6-month trial. J Investig Clin Dent. 2019;10:e12399.
- Paszynska E, Pawinska M, Gawriolek M, et al. Impact of a toothpaste with microcrystalline HAP on the occurrence of early childhood caries: a 1-year randomized clinical trial. Sci Rep. 2021;11:2650.
- Cieplik F, Rupp CM, Hirsch S, et al. Ca2+ release and buffering effects of synthetic HAP following bacterial acid challenge. BMC Oral Health. 2020;20:85.
- Cury JA, Tenuta LMA. Enamel remineralization: controlling the caries disease or treating early caries lesions? Braz Oral Res. 2009;23:23–30.
- Amaechi BT, AbdulAzees PA, Alshareif DO, et al. Comparative efficacy of a HAP and a fluoride toothpaste for prevention and remineralization of dental caries in children. BDJ Open. 2019;5:18.
- Amaechi BT, AbdulAzees PA, Okoye LO, Meyer F, Enax J. Comparison of HAP and fluoride oral care gels for remineralization of initial caries: a pH-cycling study. BDJ Open. 2020;6:9.
- Limeback H, Enax J, Meyer F. Biomimetic hydroxyapatite and caries prevention: a systematic review and meta-analysis. Can J Dent Hyg. 2021;55:148–159.
- Nobre CMG, Pütz N, Hannig M. Adhesion of HAP nanoparticles to dental materials under oral conditions. Scanning. 2020;2020:6065739.
- Lelli M, Putignano A, Marchetti M, et al. Remineralization and repair of enamel surface by biomimetic Zn-carbonate HAP containing toothpaste: a comparative in vivo study. Front Physiol. 2014;5:333.
- Hu D, Li X, Liu H, et al. Evaluation of a stabilized stannous fluoride dentifrice on dental plaque and gingivitis in a randomized controlled trial with 6-month follow-up. J Am Dent Assoc. 2019;150:S32–S37.
- James P, Worthington HV, Parnell C, et al. Chlorhexidine mouthrinse as an adjunctive treatment for gingival health. Cochrane Database Syst Rev. 2017;3:CD008676.
- Watts A, Addy M. Tooth discolouration and staining: a review of the literature. Br Dent J. 2001;190:309–316.
- Kensche A, Holder C, Basche S, Tahan N, Hannig C, Hannig M. Efficacy of a mouthrinse based on HAP to reduce initial bacterial colonisation in situ. Arch Oral Biol. 2017;80:18–26.
- Harks I, Jockel-Schneider Y, Schlagenhauf U, et al. Impact of the daily use of a microcrystal HAP dentifrice on de novo plaque formation and clinic/l/microbiological parameters of periodontal health. A randomized trial. PloS One. 2016;11:e0160142.
- Epple M, Meyer F, Enax J. A critical review of modern concepts for teeth whitening. Dent J. 2019;7:79.
- Orsini G, Procaccini M, Manzoli L, Giuliodori F, Lorenzini A, Putignano A. A double-blind randomized-controlled trial comparing the desensitizing efficacy of a new dentifrice containing carbonate/HAP nanocrystals and a sodium fluoride/potassium nitrate dentifrice. J Clin Periodontol. 2010;37:510–517.
- Amaechi BT, Mathews SM, Ramalingam K, Mensinkai PK. Evaluation of nanoHAP-containing toothpaste for occluding dentin tubules. Am J Dent. 2015;28:33–39.
- Hu ML, Zheng G, Lin H, Yang M, Zhang YD, Han JM. Network meta-analysis on the effect of desensitizing toothpastes on dentine hypersensitivity. J Dent. 2019;88:103170.
- Hiller K-A, Buchalla W, Grillmeier I, Neubauer C, Schmalz G. In vitro effects of HAP containing toothpastes on dentin permeability after multiple applications and ageing. Sci Rep. 2018;8:4888.
From Decisions in Dentistry. August 2022;8(8)9-10,13-14.
