

Occlusal Plane Correction Using Flowable Composite In a Maxillary Denture
Utilizing three-dimensional printing, thermoformed matrices and flowable composite, this novel clinical technique helped correct the occlusal plane of the mandibular arch in preparation for a maxillary denture.
Many older adults are faced with terminal dentitions and limited treatment options. At the same time, clinicians must factor in patient desires, the individual’s health and ability to endure treatment, and possible constraints related to the time and money needed to achieve predictable outcomes. This clinical report details a novel approach using intraoral scanning, three-dimensional (3D) printing, thermoformed matrices, and flowable composite to correct the occlusal plane of the mandibular arch in preparation for fabrication of a complete maxillary denture.
An 86-year-old female presented to the clinic at Midwestern University College of Dental Medicine-Arizona with a chief complaint of missing teeth, broken teeth, missing crowns, and fractured restorations (Figure 1 through Figure 5). The patient reported having all the maxillary teeth crowned three years earlier and that they began breaking about one year ago. She expressed interest in replacing the missing teeth and having her function and smile restored. The patient had a complex medical history, difficulty being in the chair for extended periods, and had financial constraints that precluded an extensive implant-supported prosthesis. In addition, since care would be provided by third- and fourth-year dental students, the treatment modalities needed to be within their skill set.
A review of the patient’s medical history revealed that she was under the care of a cardiologist and being treated for hypertension and chronic pain disorders. The patient listed eight medications, including apixaban — and, due to the challenges posed by apixaban in managing bleeding during dental extractions, a medical consultation with her cardiologist was required.1 The patient, who was determined to be ASA II under the American Society of Anesthesiologists Physical Status Classification System, had limited mobility and required her daughter to act as her translator and power of attorney.


appointment.


condition.

COMPLETE EXAMINATION
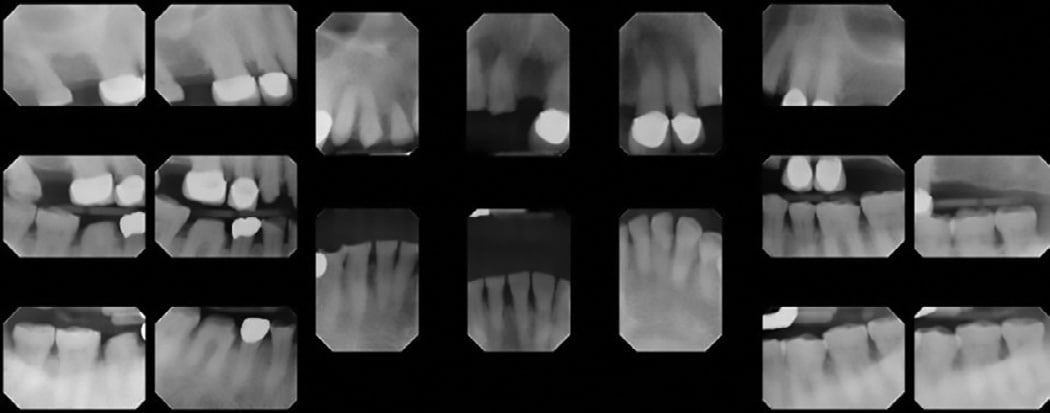
A complete intraoral examination — including a full-mouth series of radiographs (Figure 6), oral cancer screening, periodontal charting, photos and study models — was performed. The examination showed multiple decayed, missing, and fractured maxillary teeth and restorations. The mandibular teeth exhibited a combination of attrition, erosion, localized bone loss, calculus accumulation, and a missing crown on tooth #30.
Treatment planning utilized two strategies, one from Spear,2 and one from Kois3,4 Spear’s facially generated treatment planning was incorporated to put the teeth in the right location in the patient’s face. Kois’ risk factors were used to calculate the risk of tooth loss and help choose the materials and procedures that would minimize these risks. The factors are rated as low, medium or high, and the team wanted the treatment plan to minimize risk in each area of concern.
Mounted study models were used to determine the ideal position of the incisal edge, as well as the inclination of the maxillary central incisors. Next, the maxillary occlusal plane was determined using anatomic landmarks and the remaining teeth as a guide. The maxillary gingival display was evaluated before examining the positions of the mandibular incisors, occlusal plane and gingival display.
It was determined that to idealize the maxillary arch, a significant occlusal plane discrepancy would need to be addressed. Furthermore, there was some loss of vertical dimension that had to be regained in order to achieve the desired outcome of a stable and functional maxillary denture opposing a restored mandibular dentition.
REVIEW OF RISK FACTORS
Medical History — The patient was rated as a high medical risk due to hypertension and polypharmacy, including her apixaban script that increases risk for bleeding. In addition, the patient’s limited mobility/dexterity made it difficult for her to maintain proper self-care. Compounding the risk for caries, seven of her eight medications list xerostomia as a side effect.
Caries — The maxillary arch had significant recurrent decay around the existing restorations, indicating a high risk for caries. The mandibular arch had no decay and was deemed at medium risk for caries lesions due to medication-induced xerostomia and limited dexterity for self-care.
Periodontal — The initial presentation indicated a low risk for the mandibular arch. Residual calculus was found, but there was adequate bone support and attached tissue. It was determined the mandibular teeth should be able to withstand the forces of an opposing removable prosthesis. The team concluded that periodontal therapy with three-month recalls, and oral hygiene instruction will maintain a low risk for tooth loss.
Parafunction — The mandibular teeth exhibited attrition and erosion that put the patient at high risk for parafunction. That risk can be reduced by addressing the acid component of wear and providing a nightguard or opposing dentition that offers a low level of abrasiveness.
Biomechanical — It was determined the patient presented with a high risk factor due to a history of attrition and erosion leading to a diminished volume of tooth structure.
Esthetics/Expectations — While not related to tooth loss, this factor is especially important in assessing the patient’s esthetic desires and overall demeanor toward treatment. The patient and her daughter were at high risk in this regard, as both expected an excellent esthetic outcome and wanted treatment completed quickly — and with as few visits as possible.
TREATMENT PLAN PRESENTATION
A treatment plan was presented to the patient and her daughter/translator. The following options were discussed; however, some of the options meant they would have to seek care outside of the university clinic (indicated by an asterisk). The advantages, disadvantages, risks, and alternatives for each option were explained to them to their satisfaction.
Maxillary arch:
- No treatment
- Extract the maxillary teeth and place an immediate maxillary denture
- Extract the maxillary teeth, allow two months of healing, and then fabricate a transitional denture, followed by a final denture six to nine months later
- Extract, allow healing, place dental implants, allow healing, and place a hybrid denture*
- All-on-four treatment,* with extractions and immediate loading of a provisional prosthesis, followed by a final prosthesis four to six months later
Mandibular arch:
- No treatment
- Periodontal therapy that included root planing and oral hygiene instruction
- Restoration of teeth and correction of occlusal plane using matrices and direct composite
- Restoration of teeth and correction of occlusal plane using indirect restorations*
CASE ACCEPTANCE
After discussing options with the patient and daughter, it was agreed that treatment of the maxillary arch would involve removal of the remaining maxillary teeth and fabrication of a digital transitional denture, followed by a final digital denture in the future. The mandibular teeth would be maintained and undergo periodontal therapy before being restored with composite resin utilizing matrices fabricated from 3D-printed models from a digital wax-up.
The decision to extract the maxillary teeth rather than restore them was based on several factors. The cost, long chairtime for extensive visits, and difficulty in providing this level of care by undergraduate dental students made saving the teeth and conventionally restoring them unrealistic. It was determined that removing the remaining teeth and making a denture would satisfy the patient’s functional and esthetic needs. The removal of the remaining teeth was predicated on receiving clearance from the patient’s physician due to her complex medical history and use of apixaban.
On the mandibular arch, the decision was made to save and restore the remaining teeth following conservative periodontal therapy of root planing, coronal polishing, and oral hygiene instruction. The main decision involved how best to restore the teeth, keeping in mind risk factors and the team’s desire to reduce risk to the extent possible. Indirect restorations would require removal of more tooth structure and increase risks involving biomechanical issues and caries. This approach would also involve many long appointments and be the most expensive modality for saving the teeth. Equally significant, the technique would be beyond the students’ skill set at this point in their development.
The use of composite resin in vacuum-formed matrices provided several advantages.5,6 First, it required little to no preparation of the remaining tooth structure and would not increase biomechanical risk. Second, the risk of failure moves from the tooth (fracture and/or decay) to the restorative material (fracture/debonding of the composite). The resin is easily repairable intraorally by using the original matrices or a freehand technique.7 Economically, this was the best choice given the patient’s budget. Lastly, by utilizing the matrices, the students could restore all of the mandibular teeth in two visits and give the patient a positive outcome functionally and esthetically.8
APPOINTMENT SEQUENCE
Following case acceptance, consent was obtained before performing the extractions. Prior to this procedure, the patient was placed on a drug holiday from the apixaban by her physician. After the remaining maxillary teeth were removed, limited alveoloplasty was completed and the patient was allowed to heal prior to initiating fabrication of her maxillary prosthesis.
INITIAL IMPRESSIONS/SCANS
Eight weeks after the maxillary extractions, the patient presented for initial impressions that would allow fabrication of digital wax-ups to be used in creating maxillary transitional dentures and mandibular arch composite overlays. Maxillary edentulous and mandibular dentate impressions were taken using a two-part alginate material in stock impression trays. The vibrating line was marked on the maxillary impression. Papilla meter measurements were taken for rest, smile, and laughing high smile line. A centric bite tray was made with polyvinyl siloxane (PVS) putty at the desired vertical dimension of occlusion, and measurements were recorded for the lab to fabricate an upper bite plate for the second digital denture visit.
The lab used these measurements to digitally align the arches in the software for fabrication of a bite plate. In the digital denture protocol, a 3D bite plate is used to combine the final impression and maxillo-mandibular record visits into a single visit. The impressions were made, disinfected using surface disinfectant, and scanned. The impressions and centric bite tray were scanned into the design software to begin a mandibular wax-up for occlusal plane correction using resin composite, and to begin fabrication of a maxillary transitional denture at the properly adjusted vertical dimension of occlusion (VDO).
After scanning the impressions and centric bite tray into the design software, the lab technician generated digital wax-ups for the maxillary and mandibular arches based on the centric bite tray impression, papilla meter, and VDO, as measured previously. The maxillary arch wax-up standard tessellation language (STL) file was transferred to the digital denture module in the design software to begin the digital denture process. The mandibular arch wax-up STL file was imported into the software to be used to balance the occlusion. A final impression of the mandibular composite overlays will be imported prior to finalizing the maxillary transitional denture in consideration of expected variations in composite placement of the resin overlays.
The lab technician created two mandibular 3D-printed models from the digital scans and their subsequent wax-ups. The first model consisted of the wax-up to full contour of every alternating tooth (Figures 7A and 7B). The second model was the full wax-up of the mandibular teeth to full contour. Each 3D-printed model was then placed in a vacuum-forming machine with a transparent 0.5 mm viscoelastic material to produce clear matrices. The matrices were trimmed and removed from the models. A single vent hole was prepared at the incisal/occlusal of each tooth to be restored. The vent holes allowed placement of the syringe tips of the flowable composite tubes (Figure 8). In addition, a 3D bite plate was fabricated to be used at the next visit to capture final impressions and mark midline, canine and smile lines for the maxillary digital transitional denture.

(3D)-printed models of wax-ups correcting the lower occlusal plane.

RESTORATIONS
As planned, the mandibular restorations were completed by the students over two visits. Experienced practitioners could easily accomplish this in a single visit once they become familiar with the techniques. And because the teeth were not being prepared with a high-speed handpiece, no local anesthesia was used on either visit.


models, injecting composite.
For each session, the teeth were first isolated and then cleaned with pumice and water to remove any salivary proteins. At the first visit, every other tooth was to be restored. The teeth adjacent to those being restored were covered with plumber’s tape to prevent any accidental bonding. The target teeth were etched and bonded using a fourth-generation bonding agent. After the teeth were bonded and cured, the first matrix was placed over the teeth and a tight, precision fit was confirmed.
Once the fit was verified, the tip of the flowable composite syringe was inserted into the incisal/occlusal opening of the matrix and the heavily filled flowable composite was injected into the matrix until the mold for that individual tooth was filled. The tip was withdrawn, and a curing light was used to cure the flowable material through the clear matrix. This step was repeated until all target teeth were filled and cured. The matrix was removed, and each restoration was evaluated for voids and flash (Figure 9 through Figure 11). After removing the plumber’s tape from the adjacent teeth, the restorations were once again checked for flash, voids, and any irregularities that would irritate the patient’s tongue or oral mucosa. This technique was repeated at the next visit to complete the mandibular overlays and prepare for completion of the maxillary transitional digital denture.

the transparent viscoelastic matrix.

model.
TEMPORARY DENTURE FABRICATION
Once the mandibular overlays were completed (Figure 12), the team could continue with the maxillary transitional digital denture process. This approach offers benefits to the patient in that it reduces the number of visits in denture fabrication from five to four. This is due to combining the final impression and maxillo-mandibular records appointment into a single visit under the digital denture protocol. In addition, research suggests the digital denture technique produces excellent results in terms of fit and patient satisfaction.9–11
Before completing the composite overlays, the initial impressions were used to generate wax-ups for the maxillary and mandibular arches and fabrication of the 3D bite plate to be used after the overlays. At the second digital denture visit, the bite tray was tried in and assessed for incisal edge position, lip support, VDO and retention. The 3D bite plate was trimmed like a custom tray and rigid PVS was used to border-mold the tray, while light-body PVS impression material was used to make a wash impression in maximum intercuspation. Centric relation interocclusal records were made with a PVS material, an alginate impression of mandibular overlay occlusion was captured, and the denture tooth mold, tooth shade, and acrylic tissue shade were selected. Next, the lab technician imported a new scan of the mandibular impression into the software to help balance the occlusion using the digital articulator function before creating a 3D-printed trial denture.

composite restorations prior to fabrication
of an opposing denture.

At the third digital denture visit, the 3D-printed trial denture was tried in and evaluated for retention. The retention proved adequate, and the trial denture was evaluated for acceptable esthetics, phonetics and occlusion. The trial denture was approved by the patient and daughter, allowing the lab to proceed with the final milled prosthesis.
The definitive milled denture was delivered in traditional fashion at the fourth digital denture visit (Figure 13 and Figures 14A and 14B). The retention was verified, and any pressure spots were relieved using pressure-indicating paste and a slow-speed handpiece. The occlusion was checked and adjusted, and self-care instructions were given. The patient and her daughter were pleased with the final result. The patient was scheduled to complete crowns on teeth #30 and #29, but, as of presstime, have yet to return to the clinic.
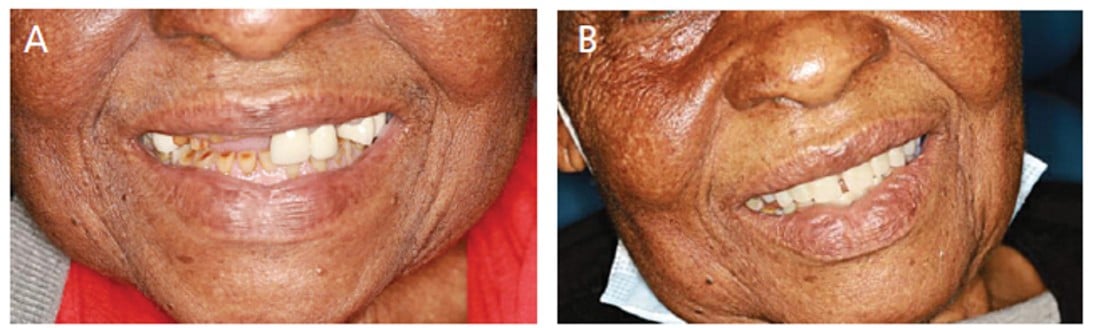
transitional denture (B).
SYNOPSIS OF TREATMENT
This case demonstrates the successful use of flowable composite to treat a mandibular dentate arch predictably and conservatively in preparation for construction of an opposing maxillary denture using a combination of digital and analog prosthetic techniques. The use of modern materials and methods allowed the completion of treatment by dental students that both satisfied the needs of the patient and maintained a conservative approach to care.
Acknowledgment: This case report was approved by the Midwestern University Office of Research and Sponsored Programs Institutional Review Board AZCS-248.
key takeaways
- This clinical report details a novel approach using intraoral scanning, three-dimensional (3D) printing, thermoformed matrices, and flowable composite to correct the occlusal plane of the mandibular arch in preparation for fabrication of a complete maxillary denture.
- In order to idealize the maxillary arch, a significant occlusal plane discrepancy would need to be addressed.
- Furthermore, there was some loss of vertical dimension that had to be regained in order to achieve the desired outcome of a stable and functional maxillary denture opposing a restored mandibular dentition.
- After discussing options with the patient, it was agreed that treatment of the maxillary arch would involve removal of the remaining maxillary teeth and fabrication of a digital transitional denture, followed by a final digital denture in the future.
- The mandibular teeth would be maintained and undergo periodontal therapy before being restored with composite resin utilizing matrices fabricated from 3D-printed models from the digital wax-up.
References
- Inokoshi M, Kubota K, Yamaga E, Ueda K, Minakuchi S. Postoperative bleeding after dental extraction among elderly patients under anticoagulant therapy. Clinical Oral Investig. 2021;25:2363–2371.
- Spear FM. Interdisciplinary management of worn anterior teeth. Facially generated treatment planning. Dent Today. 2016;35:104–107.
- Kois JC. No dentistry is better than no dentistry … really? J Cosmet Dent. 2016;32:54–61.
- Kois DE, Kois JC. Comprehensive risk-based diagnostically driven treatment planning: Developing sequentially generated treatment. Dent Clin North Am. 2015;59:593–608.
- Terry DA, Powers JM. A predictable resin composite injection technique, part I. Dent Today. 2014;33:96, 98–101.
- Terry DA, Powers JM, Mehta D, Babu V. A predictable resin composite injection technique, part 2. Dent Today. 2014;33:12.
- Ghazal M, Hedderich J, Kern M. Wear of feldspathic ceramic, nano-filled composite resin and acrylic resin artificial teeth when opposed to different antagonists. Eur J Oral Sci. 2008;116:585–592.
- Ypei Gia NR, Sobral Sampaio C, Higashi C, Sakamoto A Jr, Hirata R. The injectable resin composite restorative technique: a case report. J Esthet Restor Dent. 2021;33:404–414.
- Fernandez MA, Nimmo A, Behar-Horenstein LS. Digital denture fabrication in pre- and postdoctoral education: a survey of U.S. dental schools. J Prosthodont. 2016;25:83–90.
- Clark WA, De Kok IJ, Wolcott MD. Increasing clinic utilization with digital dentures in the pre‐doctoral clinics. J Dent Educ. September 8, 2020. Online ahead of print.
- Carreriro AFP, Cardodo RG, Tôrres ACSP, Lira AF, Melo LA, Cooper V. Masticatory efficiency, quality of life, comfort, retention and satisfaction on digital denture: case report. Rev Gaúch Odontol. 2021;69:e20210052.
From Decisions in Dentistry. March 2023;9(3)10,13-14,16-18.
