

New Paradigms in Endodontic Irrigation
Advances in irrigation devices shorten appointment times and support positive patient outcomes.
The evolution of endodontics and the supporting science of the specialty continues to make retention of a patient’s natural teeth of paramount importance. Effective disinfection of the root canal system is fundamental to successful treatment.1 Technological advances, such as the surgical microscope, cone-beam computed tomography, bioceramics, and NiTi rotary files have paved the way for more conservative approaches to root canal treatment.2–5 Incorporating these technological advances in pursuit of tooth conservation through smaller coronal accesses and root preparations has created a need for supplementary and efficient canal disinfection and facilitated the evolution of irrigation advances.
In general, root canal treatment involves cleaning, disinfecting, and debriding the root canal system of vital tissue, necrotic tissue, and bacteria for the management of apical periodontitis.6 Typically, this involves a mechanical preparation of the root canal system in the presence of sodium hypochlorite (NaOCl) to allow further delivery of additional NaOCl throughout the root canal system.7 Within the evolution of endodontics, larger canal preparation sizes, different irrigants, and activation techniques have been developed to supplement NaOCl and to facilitate the deep removal of debris along the canal wall in order to, theoretically, eliminate more bacteria. Most research shows that a larger canal preparation allows for deeper delivery of chemical irrigants and removal of more bacteria, leading to improved healing.7–9
Other chemical irrigants have also been used to aid in smear layer removal and reduction of bacterial biofilm. Some of these include stand-alone irrigants, such as ethylenediamine tetraacidic acid (EDTA) and chlorhexidine digluconate, while others offer a combination of ingredients.10–12 In many cases, calcium hydroxide may be placed in the canals as an intracanal medicament to help with bacterial reduction.13 Calcium hydroxide placement, however, will add additional patient visits and, potentially, a reduced patient experience.
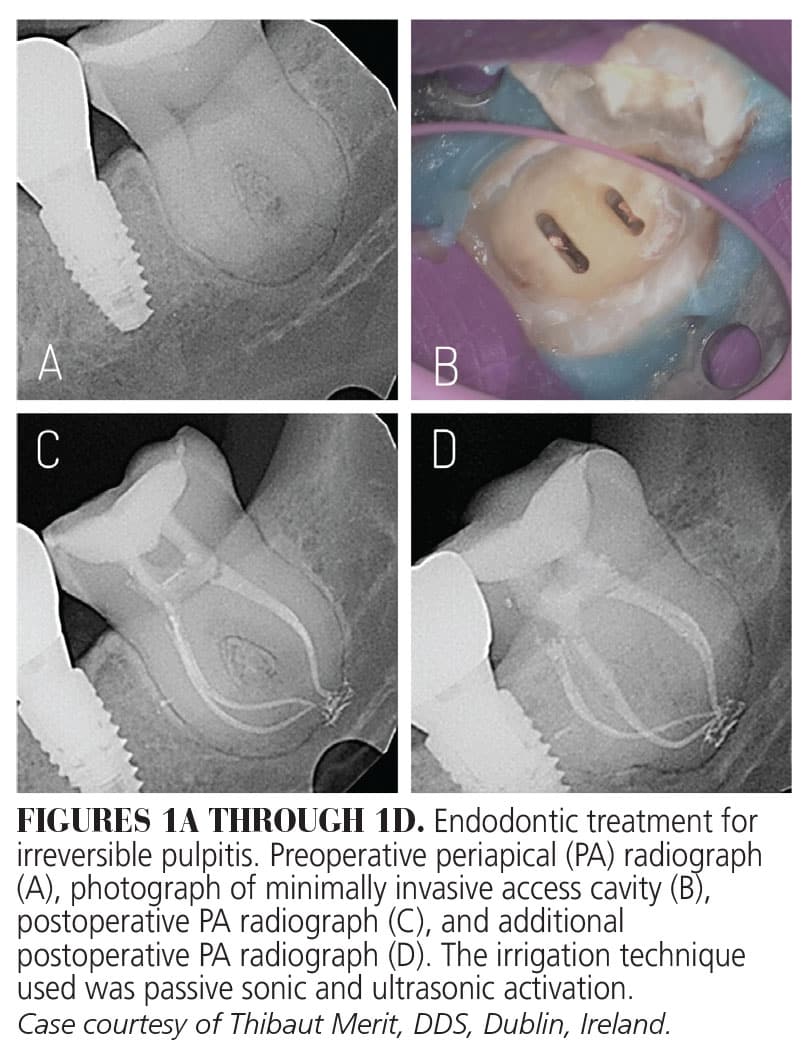 Historically, irrigation with NaOCl using a standard technique allows for high root canal treatment success and survival rates.6,14,15 In the hands of highly skilled endodontists, canal preparation can be rendered conservatively using traditional irrigation. Typically, irrigants are delivered into the root canal system using a standard syringe and needle tip. However, as coronal access and canal preparation become smaller to preserve structural strength within the tooth, other irrigation techniques are used to help activate and deliver the irrigants apically. Some of these techniques include heating of NaOCl, manual dynamic activation, negative pressure irrigation, and passive activation of the irrigants using a plastic tip/sonic or metal ultrasonic tip/device.16–19 Most research demonstrates an additional bacterial reduction with these supplemental disinfection techniques (Figures 1A through 1D). Nevertheless, concern remains regarding whether the irrigants deliver their disinfection capability within the apical third of all root canal systems, as well as allowing obturation after disinfection of smaller more complex spaces, which requires additional clinical expertise.
Historically, irrigation with NaOCl using a standard technique allows for high root canal treatment success and survival rates.6,14,15 In the hands of highly skilled endodontists, canal preparation can be rendered conservatively using traditional irrigation. Typically, irrigants are delivered into the root canal system using a standard syringe and needle tip. However, as coronal access and canal preparation become smaller to preserve structural strength within the tooth, other irrigation techniques are used to help activate and deliver the irrigants apically. Some of these techniques include heating of NaOCl, manual dynamic activation, negative pressure irrigation, and passive activation of the irrigants using a plastic tip/sonic or metal ultrasonic tip/device.16–19 Most research demonstrates an additional bacterial reduction with these supplemental disinfection techniques (Figures 1A through 1D). Nevertheless, concern remains regarding whether the irrigants deliver their disinfection capability within the apical third of all root canal systems, as well as allowing obturation after disinfection of smaller more complex spaces, which requires additional clinical expertise.
As the field of endodontics moves toward conservation of tooth structure and remaining tooth strength, effective root canal disinfection continues to be difficult. Because the majority of the canal walls cannot be sufficiently cleaned with mechanical methods, irrigation solutions are used to clean and disinfect the uninstrumented portions of the root canal system.20
Many endodontists are now embracing more advanced irrigation devices for canal disinfection, treatment efficiency, and improved patient experience. Endodontists using these advanced irrigation systems are reporting shorter treatment appointments, less tooth structure removal, and a more composed treatment of difficult and increasingly complex root canal systems.
Laser-assisted irrigation (LAI), which is also termed photodynamic therapy, has been shown to remove smear layer, bacteria, and debris during root canal treatment.21,22 This type of irrigation allows for shorter treatment times, more controlled disinfection, and smaller canal preparations.
The rapid fluid movement generated by lasers within the root canals, as a result of the creation and explosion of vapor bubbles, results in better delivery of the irrigation solutions throughout the anatomical complexities of the root canal system.23 Additionally, LAI has been proposed as an alternative irrigation technique for delivering irrigants deep down canals, resulting in increased smear layer removal and bacteria reduction.24,25 Typical syringe irrigation generally does not reach more than 2 mm beyond the needle tip.26
The erbium-based lasers have been shown to generate shock waves within the chemical irrigants of root canals.27 Therefore, laser-assisted root canal treatment may provide added flexibility when it comes to preparing the size of canals. The erbium chromium yttrium scandium gallium garnet (ErCr:YSGG) and erbium-yttrium aluminium garnet (Er:YAG ) lasers are most frequently used in laser-assisted root canal treatment.
Erbium Chromium Yttrium Scandium Gallium Garnet Laser
The ErCr:YSGG (2780 nm wavelength) laser has radial firing tips that can be used in the pulp chamber and within the canals. Its unique radial beam pattern does not fire directly into the apex, allowing added uniform coverage of the root surface during firing.28
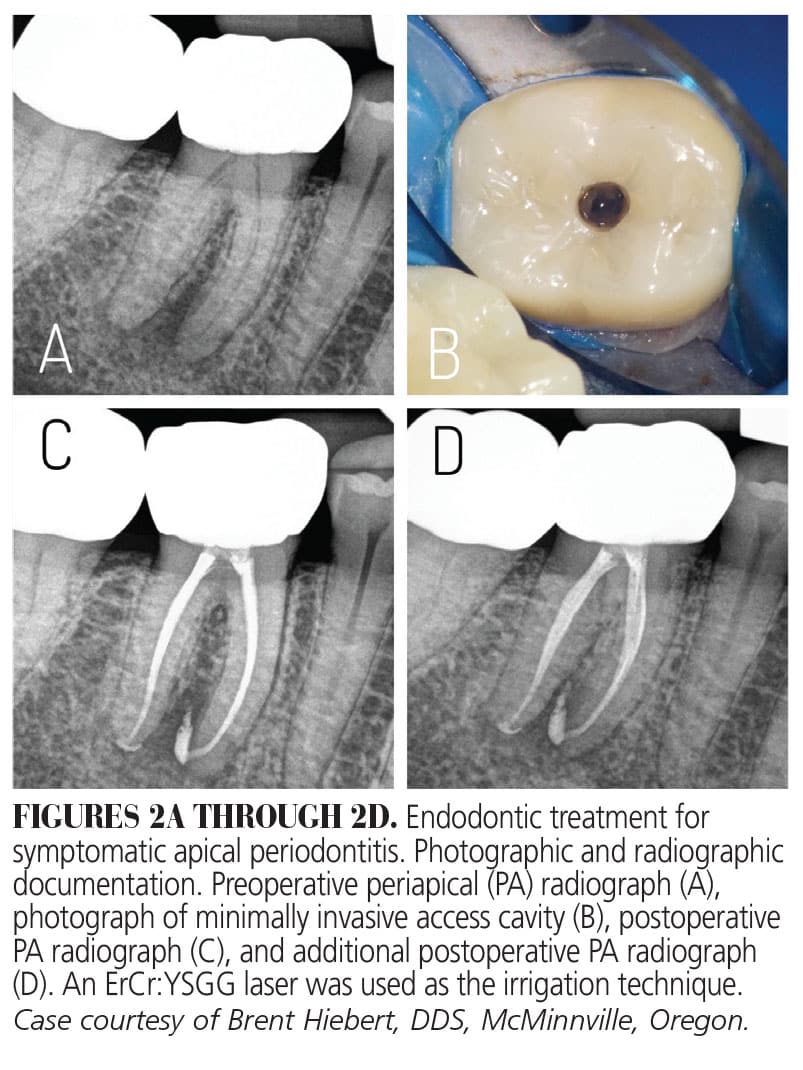 According to the manufacturer, once the tip is activated, it creates thousands of vapor bubbles per second, which then expand and explode. This creates acoustic streaming and cavitation effects within the irrigant and anatomical complexities of the tooth.25 Disinfection efficiency is improved by eliminating bacteria through cleaning of the canal walls, removal of biofilm, and opening dentinal tubules in order to allow for deeper cleaning.27 This type of laser may reduce treatment time and enable care to be provided in one appointment (Figures 2A through 2D).28,29
According to the manufacturer, once the tip is activated, it creates thousands of vapor bubbles per second, which then expand and explode. This creates acoustic streaming and cavitation effects within the irrigant and anatomical complexities of the tooth.25 Disinfection efficiency is improved by eliminating bacteria through cleaning of the canal walls, removal of biofilm, and opening dentinal tubules in order to allow for deeper cleaning.27 This type of laser may reduce treatment time and enable care to be provided in one appointment (Figures 2A through 2D).28,29
Erbium-Yttrium Aluminium Garnet Laser
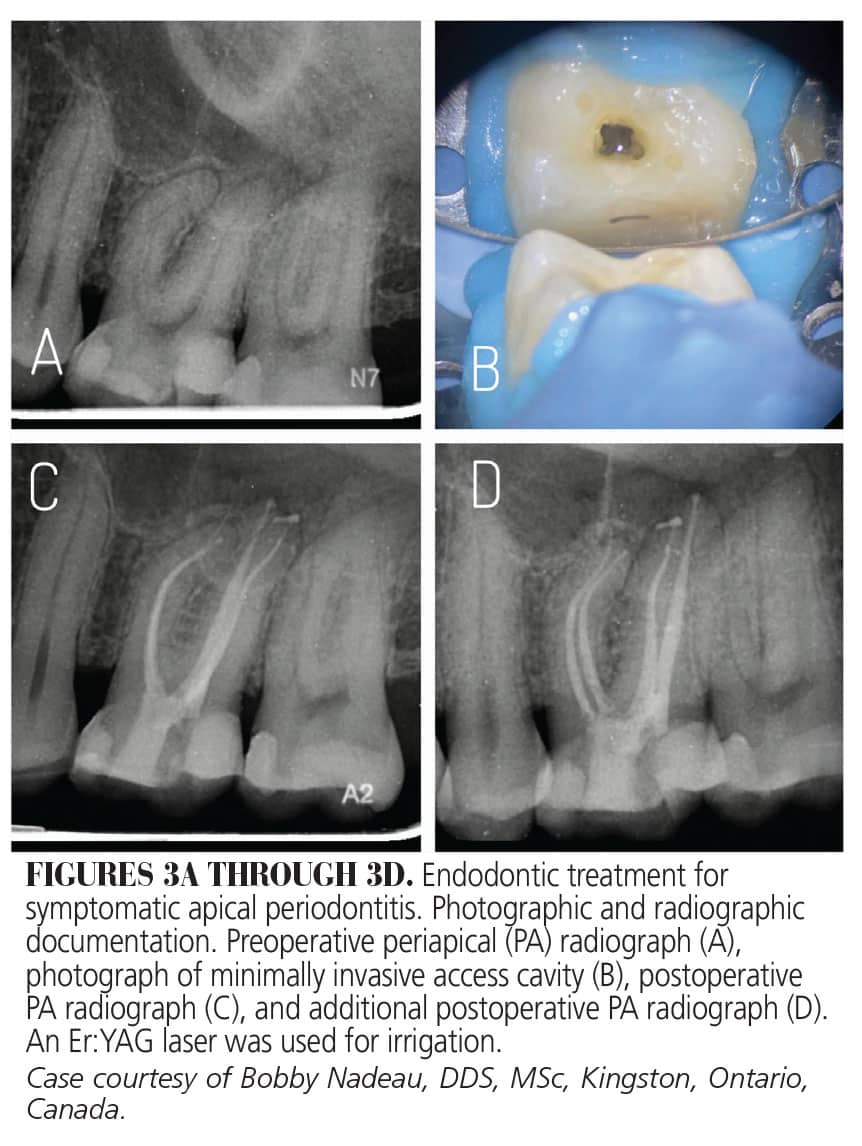
The Er:YAG (2940 nm wavelength) laser uses conical and striped fiber tips. These laser-emitting fiber tips fire only within the pulp chamber and direct the laser energy down into the root canal system.23 The newer Er:YAG lasers use a combination of super short pulse irrigation (also known as photoninduced photo-acoustic streaming) with shock wave-enhanced emission photo-acoustic streaming.24 This new laser generates synchronized primary and secondary shock waves emitted by collapsed bubbles throughout the confined root canal system.21,23 As with the ErCr:YSGG laser, the manufacturer and practitioners report the ability to provide reduced canal preparations, shorter treatment times, and more frequent single-visit appointments (Figures 3A through 3D).
Less Instrumentation
With the advent of newer irrigation technologies, many endodontists are moving toward less instrumentation. A novel irrigation using multisonic cleaning technology allows for acoustic streaming and tissue dissolution throughout the root canal system. This machine lends itself to single-visit appointments and caters to practitioners seeking less instrumentation and an added focus on irrigation delivery.30
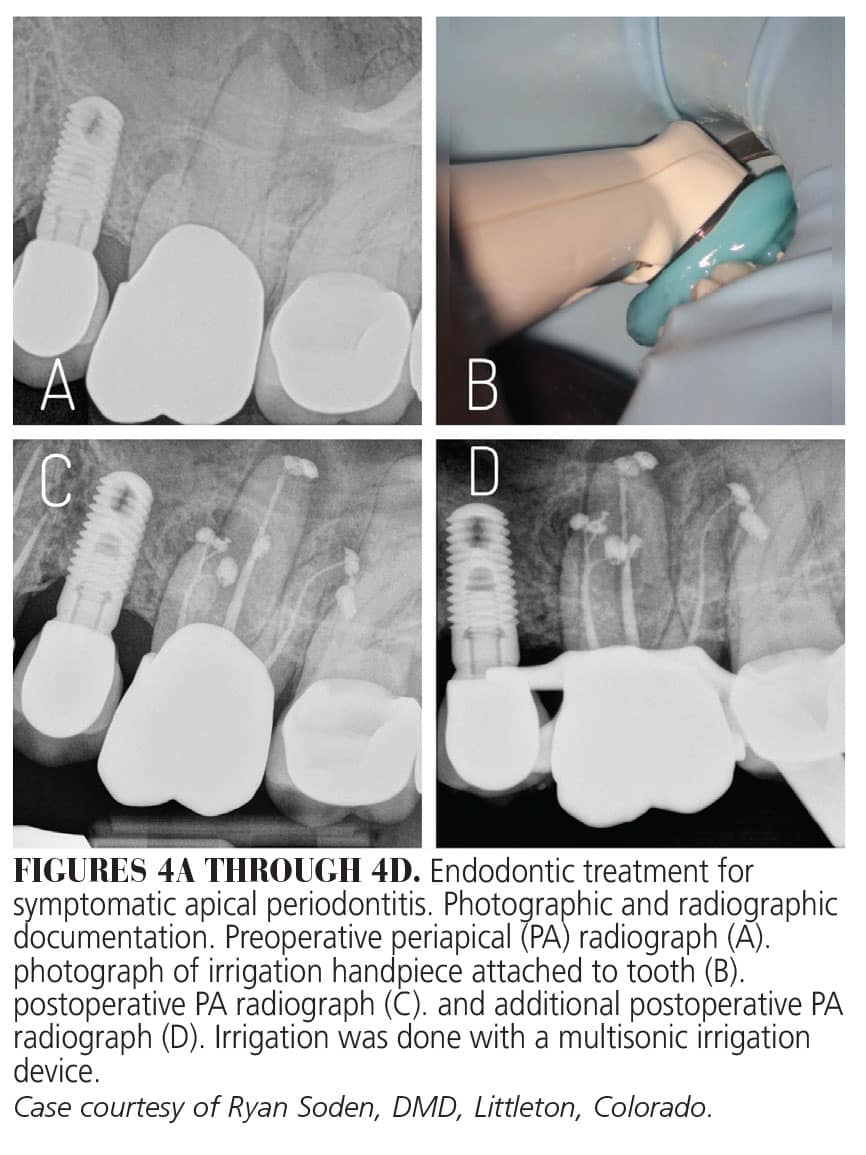
 This machine has a digital monitor with a large console housing the hardware and a sterile and single-patient use irrigation-handpiece.31 With this technique, once the tooth has been properly accessed and the canals minimally prepared, a special resin platform must be built around the tooth to seal the handpiece and secure the tip within the pulp chamber.30 Once secured, the handpiece delivers a constant stream of irrigants directly into the pulp chamber and throughout the root canal system. While the solution is delivered, a suction tip extending from the handpiece also removes excess irrigant from the chamber.31
This machine has a digital monitor with a large console housing the hardware and a sterile and single-patient use irrigation-handpiece.31 With this technique, once the tooth has been properly accessed and the canals minimally prepared, a special resin platform must be built around the tooth to seal the handpiece and secure the tip within the pulp chamber.30 Once secured, the handpiece delivers a constant stream of irrigants directly into the pulp chamber and throughout the root canal system. While the solution is delivered, a suction tip extending from the handpiece also removes excess irrigant from the chamber.31
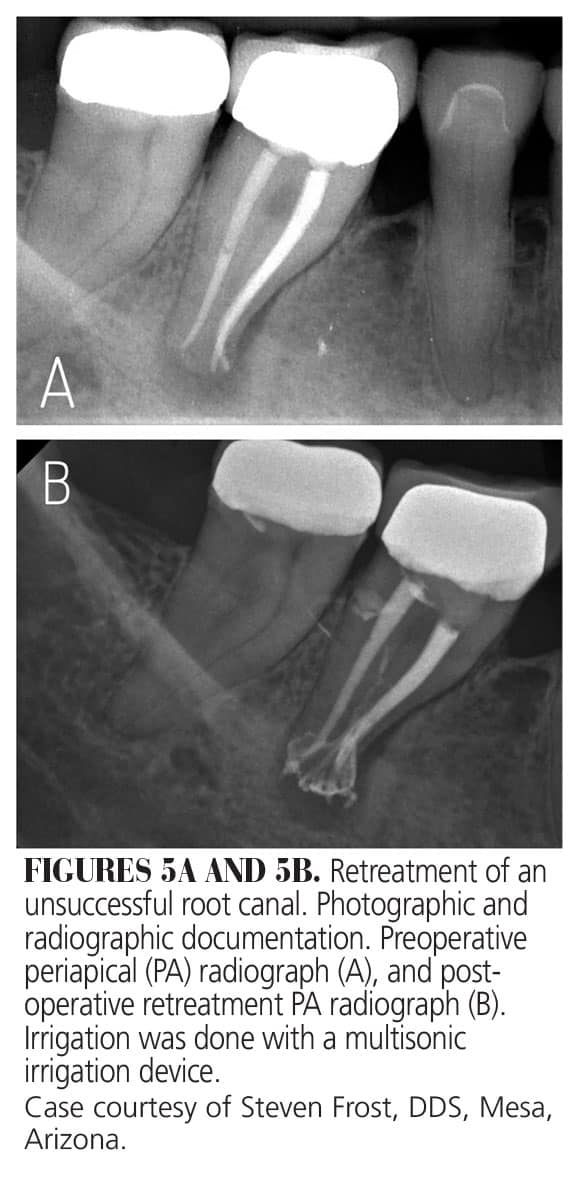
When activated, multisonic waves are generated at the tip of the handpiece, creating a hydrodynamic cavitation. This effect, along with the generation of microbubble implosions, generates an acoustic streaming phenomenon that extends to the apices of each root. The handpiece delivers constant cycles NaOCl, EDTA, and saline for 7 to 8 minutes throughout the root canal system, leading to enhanced cleaning, debridement, and disinfection of the root canal system. In addition to less instrumentation, this system allows for treatment of more complex canal anatomy, with providers reporting shorter treatment times and less post-operative pain.30,31 A short-term clinical study has demonstrated a high success rate using this approach (Figures 4A through 5B).32
Conclusion
As more patients look to retain their natural dentition, endodontics will always play an important and valued role in dentistry. Over the past two decades, endodontists and the scientific research within the specialty have allowed significant advances in technology, materials, and endodontic treatment procedures.
The evolution of new irrigation paradigms is exciting. New irrigants and devices are being developed to allow for better disinfection within a more conservative root preparation. The caveat here is that while cleaning and disinfection are significantly enhanced, these new irrigation technologies require responsible training and usage. In addition, obturation of smaller complex spaces requires real skill and competence. These advanced techniques and technologies seem to offer shorter treatment times and single visit appointments; however, even with these new irrigation technologies, the core principals of root canal treatment remain the same. If enough bacteria is eliminated within the root canal system, the body will heal the infectious insult. Most research demonstrates that a basic syringe irrigation technique with NaOCl will continue to provide high success and survival rates. Additionally, if advanced irrigant activation techniques are implemented, whether they be sonic, multisonic, or laser assisted, an even higher bacterial reduction occurs within the root canal system.
Based on current research, a predictable root canal treatment should always be provided when the practitioner is following the standards of endodontic practice supported by sound scientific principles. As additional clinical research data comparing activation techniques and irrigation technologies become available, endodontics will truly evolve.
References
- Zehnder M. Root canal irrigants. J Endod. 2006;40:389-398.
- AAE Position Statement. Use of microscopes and other magnification techniques.J Endod. 2012;38:1153-1155.
- American Association of Endodontists; American Acadamey of Oral and Maxillofacial Radiography. AAE and AAOMR joint position statement. Use of cone-beam-computed tomography in endodontics. Pa Dent J (Harrisb). 2011;78:37-39.
- Haapasalo M, Parhar M, Huang X, Wei, X, Lin J, Shen Y. Clinical use of bioceramic materials. Endodontic Topics. 2015;32(1):97-117.
- Walia H, Brantley W, Gerstein H, et al. An initial investigation of the bending and torsional properties of nitinol root canal files. J Endod. 1988;14:346-351.
- Peters OA, Peters CI, Basrani B. Cleaning and shaping the root canal system. In: Hargreaves KM, Berman LH, eds. Cohen’s Pathways of the Pulp. 11th ed. Philadelphia: Elsevier. 2016:209-279.
- Shuping G, Orstavik D, Sigurdsson A, Trope M. Reduction of intracanal bacteria using nicki-titanium rotary instrumentation and various medications. J Endod. 2000;26:751-755.
- Rodrigues R, Zandi H, Kristoffersen AK, et al. Influence of the apical preparation size and the irrigant type on bacterial reduction in root canal-treated teeth with apical periodontitis. J Endod. 2017;43:1058-1063.
- Khademi A, Yazdizadeh M, Feizianfard M. Determination of the minimum instrumentation size for penetration of the irrigants to the apical third of root canal systems. J Endod. 2006;32:417-420.
- Zandi H, Rodrigues R, Kristoffersen AK, et al. Antibacterial effectiveness of 2 root canal irrigants in root-filled teeth with infection: a randomized clinical trial. J Endod. 2016;42:1307-1313.
- Stojicic S, Shen Y, Qian W, Johnson B, Haapasalo M. Antibacterial and smear layer removal ability of a novel irritant, QMIX. Int Endod J.2011;45:363-371.
- Grawehr M, Sener B, Waltimo T, Zehnder M. Interactions of ethylenediamine tetra acetic acid with sodium hypochlorite in aqueous solutions. Int Endod J. 2003;36:411-415.
- Sjogren U, Figdor D, Spangberg L, Sundqvist G. The antimicrobial effect of calcium hydroxide as a short-term intracanal dressing. Int Endod J. 1991;24:119-125.
- Torabinejad M, Anderson P, Bader J, et al. Outcomes of root canal treatment and restoration, implant-supported single crowns, fixed partial dentures, and extraction without replacement: a systematic review. J Prosth Dent. 2007;98:285-311.
- Salehrabi R, Rotstein I. Endodontic treatment outcomes in a large patient population in the USA: an epidemiological study. J Endod. 2004;30:846-850.
- Stojicic S, Zivkovic S, Qian W, Zhang H, Haapasalo H. Tissue dissolution by sodium hypochlorite: effect of concentration, temperature, agitation, and surfactant. J Endod. 2010;36:1558-1562.
- Caron G, Nham K, Bronnec F, Machtou P. Effectiveness of different final irrigant activation protocols on smear layer removal in curved canals. J Endod. 2010;36:1361-1366.
- Jiang L, Lak B, Eijsvogels LM, Wesselink P, Lucas LWM. Comparison of the cleaning efficacy of different final irrigation techniques. J Endod. 2012;38:838-841.
- Munoz H, Camacho-Cuadra K. In vivo efficacy of three different endodontic irrigation systems for irrigant delivery to working length of mesial canals of mandibular molars. J Endod. 2012;38:445-448.
- Haapasalo M, Shen Y, Wang Z, Gao Y. Irrigation in endodontics. Br Dent J. 2014;216:299-303.
- Ivanusic T, Lukac M, Lukac M, Jezersek M. SSP/SWEEPS endodontics with the SkyPulse Er:YAG dental laser. Journal of the Laser and Health Academy. 2019;1:1-10.
- American Association of Endodontists. Use of Lasers in Dentistry. Available at: aae.org/wp-content/uploads/2019/10/2019_LasersinDentistry.pdf. Accessed March 7, 2024.
- Lukac N, Jezersek M. Amplification of pressure waves in laser-assisted endodontics with synchronized delivery of Er:YAG laser pulses. Lasers Med Sci. 2018;33:823-833.
- Lukac N, Muc B, Jezersek M, Lukac M. Photoacoustic endodontics using the novel SWEEPS Er:YAG laser modality. Journal of the Laser and Health Academy. 2017;1:1-7.
- Betancourt P, Merlos A, Sierra JM, Arnabat-Dominguez J, Vinas M. Er,Cr:YSGG Laser-activated irrigation and passive ultrasonic irrigation: comparison of two strategies for root canal disinfection. Photobiomodul Photomed Laser Surg. 2020;38:91-97.
- Falk K, Sedgley C. The influence of preparation size on mechanical efficiency of root canal irrigation in vitro. J Endod. 2005;31:742-745.
- Martins M, Carvalho M, Pina-Vaz I, Capelas JA, Martins MA, Gutknecht N. Outcome of Er,Cr:YSGG laser-assisted treatment of teeth with apical periodontitis: a blind randomized clinical trial. Photomed Laser Surg. 2014;32:3-9.
- Gordon W, Atabakhsh VA, Meza F, et al. The antimicrobial efficacy of the ErCrYSGG laser with radial emitting tips on root canal dentin walls infected with E faecalis. J Am Dent Assoc. 2007;138:992-1002.
- Soares F, Varella C, Pileggi R, Adewumi A, Guelman M. Impact of Er,Cr:YSGG laser therapy on the cleanliness of the root canal walls of primary teeth. J Endod. 2008;34:474-477.
- Velardi J, Alquria T, Alfirdous RA, Griffin IL, Tordik PA, Martinho FC. Efficacy of GentleWave System and passive ultrasonic irrigation with minimally invasive and conventional instrumentation technique against enterococcus faecalis lipoteichoic acid in infected root canals. J Endod. 2022;48:768-774.
- Vandrangi P, Basrani B. Multisonic ultracleaning in molars with the GentleWave System. Available at: oralhealthgroup.com/features/multisonic-ultracleaningt-in-molars-with-the-gentlewavet-system. Accessed March 6, 2024.
- Sigurdsson A, Garland R, Le KT, Woo SM. 12-month healing rates after endodontic therapy using the novel Gentlewave System: a prospective multicenter clinical study. J Endod. 2016;42:1040-1048.
From Decisions in Dentistry. March 2024; 10(2):10,13-15
