

Multidisciplinary Approach to a Complex Case
A patient presenting with multiple challenging factors required creative orthodontic treatment planning.
A patient presenting with multiple challenging factors required creative orthodontic treatment planning
Canine impaction or ectopic eruption, idiopathic generalized root resorption, canine-induced root loss on lateral incisors and severe crowding each present distinct challenges in orthodontic treatment. When all of these factors are present in an individual patient, they create a complex case involving orthodontic and esthetic treatment challenges.
The patient in this case report presented with all of these orthodontic issues. Complicating this already difficult treatment was the esthetic concerns of the patient, who was entering her senior year in high school. The treatment modality selected would require dental spacing in the maxillary anterior dentition, along with the placement of a temporary prosthesis that would allow for the proposed tooth extrusion. This made the situation even more complex.
This report illustrates a creative approach to solving the dilemma of eruption of impacted/ectopically positioned maxillary canines into the very prominent lateral incisor space, while exercising extreme caution not to exacerbate root resorption and maintaining acceptable esthetics during tooth movement.
DIAGNOSIS AND ETIOLOGY
The patient was a 17-year-old Hispanic female who presented with the desire “to have my front teeth straightened.” The patient had no relevant medical history that could be associated with the generalized resorption exhibited radiographically. She also had no history of previous orthodontic treatment or trauma to her dentition.

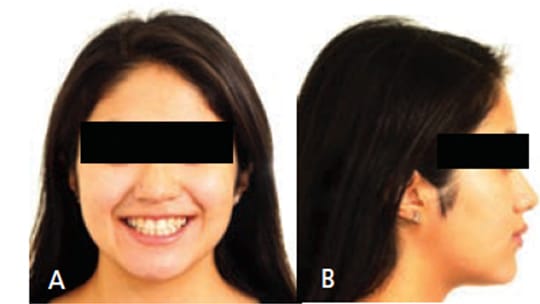
Extraoral examination showed a normal profile, with good facial symmetry when viewed frontally (Figures 1A and 1B). The intraoral examination revealed a Class I molar relationship with a slight posterior transverse deficiency, an anterior crossbite involving teeth #7 and 10, minimal overbite and overjet, and an estimated 15 mm of crowding in the maxillary anterior region and 12 mm of generalized crowding in the mandibular arch (Figures 2A through 2C). Tooth #14 had previous endodontic treatment and was restored with a porcelain-fused-to-metal crown, but had been asymptomatic for several years prior to presentation at the clinic.



The panoramic (Figure 3) and intraoral radiographic findings revealed generalized short roots (idiopathic root resorption versus anatomically short roots) on teeth #4, 5, 8, 9, 11, 12, 13, 20, 22, 27 and 29. The resorption present on teeth #7 and 10 was attributed to the proximity of the crowns of #6 and 11. A large restoration was noted on tooth #3. Teeth #1, 16, 17 and 32 were present on the radiograph. The condyles appeared symmetrical. Bone levels appeared to be normal.

The cephalometric findings revealed a Class I dental and skeletal relationship, with normal maxillary and mandibular position relative to the cranial base. The maxillary incisors were in a normal position relative to the maxillary bony base, as were the mandibular incisors relative to the mandibular bony base. Considering her chronological age and cervical vertebrae maturation, the patient had little, if any, remaining adolescent growth.
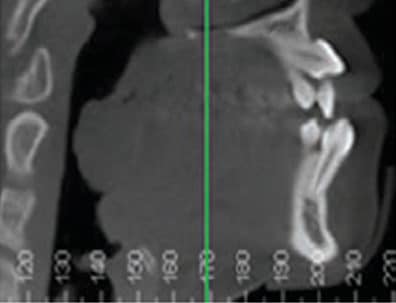
Cone beam computed tomography (CBCT) was obtained to assist in determining the position of tooth #11, as well as to assess the degree of root resorption of #7 and 10 (Figures 4A and 4B). It confirmed the finding of root resorption on the other teeth, as demonstrated by conventional radiographs.

The treatment objectives were to:
- Minimize any further root resorption due to orthodontic treatment
- Alleviate dental crowding
- Orthodontically extrude #6 and 11, and bring them into proper position
- Achieve slight transverse expansion of the maxillary dental arch
- Maintain Class I occlusal relationships
- Establish normal overbite and overjet
- Provide acceptable esthetics, both during treatment and at the conclusion of treatment (and with minimal prosthodontic treatment)
TREATMENT ALTERNATIVES
One of the biggest technical challenges was providing anterior anchorage to extrude teeth #6 and 11, while placing minimal pressure on #8 and 9, which could exacerbate the existing root resorption and possibly lead to the loss of the maxillary central incisors. After examination of the CBCT, the decision was made to extract teeth #7 and 10, and substitute the canines for the hopelessly resorbed maxillary lateral incisors. Teeth #21 and 28 were removed to resolve crowding in the mandibular arch.

Other treatment options for the maxillary arch included a more traditional extraction pattern, with extraction of maxillary first bicuspids and eruption and retraction of the maxillary canines into the extraction spaces. Due to the significant concern regarding the viability of teeth #7 and 10 — as demonstrated by the radiographs and CBCT (Figure 5) taken prior to treatment — this approach was not chosen. In addition, a nonextraction approach was ruled out due to severity of the crowding, soft tissue profile and depth of bite, as well as a probable increase in treatment time. Prosthetic replacement of all maxillary anterior teeth was also considered, especially in the event the maxillary canines were not amenable to orthodontic eruption. Due to the patient’s age and desires, however, this course of treatment was also dismissed.

Miniscrews were considered for potential bone anchorage in the maxillary anterior to assist in the extrusion of both canines, but the patient declined. Since exacerbation of the resorption of the central incisor roots was a concern, the anchorage used for extrusion of the maxillary canines was a maxillary lingual arch, with bands on the first molars, and occlusal rests on the maxillary first bicuspids. Placing appliances on the maxillary central incisors was delayed as long as possible, and the occlusion was built around the existing position of these two maxillary central incisors (Figure 6).

The other dilemma was maintaining dental esthetics during maxillary canine extrusion. Inconspicuous arms were placed on the maxillary lingual arch so that elastomeric traction could be applied at the disto-gingival aspect of the pontics. Fortunately, the patient did not display any maxillary gingiva upon smiling, which allowed continuous pontic shortening during the course of treatment. After the fabrication of the maxillary lingual arch, a temporary prosthesis with lateral incisor pontics was created so that it could be removed by the patient for cleaning — and by the practitioner to shorten the pontics, as needed (Figure 7).
TREATMENT PROGRESS
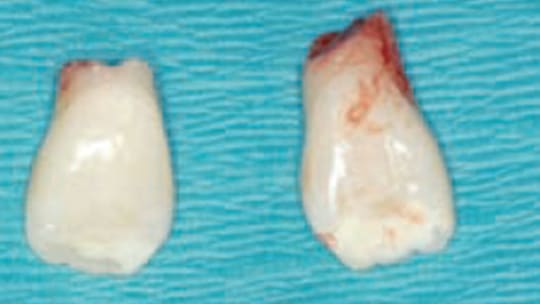
Bands were fit to the maxillary first molars and an impression was taken for the maxillary lingual arch one week prior to the surgical visit for the removal of teeth #1, 7, 10, 16, 17, 21, 28 and 32. At the same surgery visit, tooth #11 was surgically exposed and a button with a chain attachment was bonded to the tooth. The lingual arch was seated and cemented and traction was applied to teeth #6 and 11 using elastomeric thread. Next, the temporary prosthesis was seated over the lingual arch. The pontics were left slightly long to allow for settling of the appliance postsurgically (Figure 8 and Figure 9). The lack of root structure and poor prognosis of the maxillary lateral incisors was clinically confirmed following their removal (Figure 10).


Fixed mandibular orthodontic appliances were placed two months after surgery. Maxillary fixed appliances were placed approximately four months after the surgical exposure. The maxillary central incisors were not bracketed until late in treatment to limit the possibility of further root resorption. The maxillary lingual arch was removed six months into treatment when the arms began to interfere with extrusion of the maxillary canines.
The patient had minimal overbite at the initiation of therapy, and this continued to be problematic for much of the treatment. Controlling the open bite was complicated by not incorporating the maxillary central incisors into the appliance to avoid stressing them. Vertical control was enhanced with Class I box elastics from the maxillary canines and first bicuspids to the mandibular canines and lateral incisors. Sliding mechanics (coil springs) were used for space closure in the mandibular arch.
To avoid the possibility of continued root resorption, teeth #8 and 9 were bracketed only two months prior to appliance removal. The patient was consulted regarding her satisfaction with the overall treatment results after 20 months of therapy. She reported being pleased, and the decision was made to remove her appliances and retain the results (Figures 11A and 11B). She was also advised that loss of the maxillary central incisors over time was a very real possibility.
TREATMENT RESULTS
The posttreatment panoramic radiograph (Figure 12) demonstrated approximately the same amount of root resorption that was noted pretreatment. Significant measures were taken not to jeopardize the health of the maxillary central incisors. Although the maxillary canines could have been uprighted more, it was determined that the risk to adjacent teeth was greater than the potential benefit, so the teeth were left in their final position.

The dental crowding was alleviated and both arches were aligned. Teeth #6 and 11 were satisfactorily extruded into the dental arch and cosmetically reshaped to resemble maxillary lateral incisors. The maxillary arch was expanded slightly using archwire expansion establishing normal buccal overjet bilaterally. The molar relationship remained Class I, with very slight Class II windows in the bicuspid occlusion.
Treatment improved both the overbite and overjet, and the reshaped canines provided an esthetic and nonprosthetic solution for the missing maxillary lateral incisors. Examination of the post-treatment dental casts revealed that the Curve of Spee in the mandibular arch was not completely eliminated. This was due to concerns over length of treatment, as well as a desire to establish some overbite. Esthetic considerations were addressed by using an extraction pattern that did not over-retract the maxillary incisors. The uprighting of the mandibular incisors improved the overjet and overbite relationships (Figures 13A through 13C). To date, there has been no need for prosthodontic treatment following orthodontic treatment.



DISCUSSION
Any one of the mitigating conditions presented in this case — generalized root resorption, localized root resorption due to ectopic or impacted canines, lack of overbite and overjet, anterior crossbites, canine substitution and severe crowding — are problematic in and of themselves. When all nine of these conditions present in one patient, treatment requires innovative thinking.
Maxillary canine impaction occurs in approximately 2% of the population, with a 2:1 predominance of females to males. Impaction of maxillary canines is more than twice as prevalent as the impaction of mandibular canines.1,2 Among patients with impacted maxillary canines, 85% of cases include palatal impaction, and 15% involve facial impactions. Root resorption of adjacent permanent incisors has been reported in 48% of patients with ectopic eruption of maxillary canines, with resorption occurring equally in males and females.3 Studies using CBCT have shown an even higher incidence of resorption of the lateral incisors (67%) than have previous two-dimensional studies.4 Resorption of the roots of incisors adjacent to ectopically positioned/impacted canines may lead to tooth loss and/or time-consuming and expensive orthodontic treatment.5,6
With few exceptions, most cases of generalized external apical root resorption with no prior history of orthodontic tooth movement have no evident etiology.7 Suggested causes of root resorption with no apparent cause (i.e., idiopathic root resorption) include genetic influences,8,9 systemic factors,10,11 drugs (e.g., nambumetone),12 hormone deficiency, hypothyroidism, hypopituitarism,13–16 asthma,17 chronic alcoholism,18 root proximity to cortical bone, alveolar bone density,19 severity and type of malocclusion,20–22 tooth-root morphology, length, and developmental abnormalities,23–25 patient age7,26,27 and sex.28–30 The conditions contributing to idiopathic generalized root resorption were reviewed in detail in an article by Weltman et al31 in 2010.
Another possible explanation for the generalized incidence of anatomically short roots is a condition termed short root anomaly. Lind first identified it in 1972.32 It is not well documented and subsequently is poorly understood. It was defined as a condition in which the teeth exhibit “abnormally short, plump roots, always affecting the maxillary central incisors and rarely any other teeth.”32 This particular patient exhibited short roots on teeth other than the maxillary central incisors, but this would not definitively rule out a diagnosis of short root anomaly. In a study by Puranik et al,33 a group of Latino (26 subjects) and one Filipino subject were evaluated for short root anomaly. Teeth were affected bilaterally, with maxillary central incisors (63%) and mandibular second premolars (33%) being most commonly involved. Maxillary premolars can also be involved. The study, along with other supporting literature, demonstrated an autosomal dominant pattern of inheritance among the subjects and has also been referred to as hereditary idiopathic root malformation.
Dental crowding is the most frequent cause for seeking orthodontic treatment.34 The incidence of crowding in the late mixed dentition/early adult dentition affects between 32% to 50% of the population.35 This patient presented with a full spectrum of challenging conditions, including, but not limited to, severe dental crowding and a lack of overbite and overjet.
CONCLUSION
The technical difficulties of treatment and importance of providing acceptable esthetics for a 17-year-old high school senior complicated an already complex case. The incorporation of the removable prosthesis with pontics during the extrusion of the maxillary canines was an integral part of patient satisfaction with treatment. Although it added another technical step, it was well worth the time and effort to fabricate and place the appliance.
In this case, patient esthetics — both during and after treatment — were enhanced by adequate upper lip length that covered the maxillary anterior gingival tissue during extrusion of the ectopic canines. This also allowed the pontics to be shortened during extrusion without the hooks and elastomeric string showing. Following treatment, the substituted canines exhibited more crown length than lateral incisors, but the gingival margins were not typically displayed during the patient’s normal animated smile. The esthetic impact of the gingival margin discrepancy that accompanies canine substitution was less problematic as a result of her lip length.
This patient presented with multiple dental conditions that required an unusual treatment combination of a maxillary lingual arch for extrusion of ectopically erupted and impacted maxillary canines, coupled with the use of an overlay prosthesis to replace the removed maxillary lateral incisors. The prosthesis was unique because it could be adjusted as necessary for canine extrusion. Most of all, it allayed the fears of a young patient regarding her appearance while enabling normal occlusion to be established. Furthermore, the immediate need for prosthodontic treatment was negated. Should the patient eventually lose the maxillary central incisors or bicuspids, strong abutments will be strategically located for support of a fixed prosthesis
KEY TAKEAWAYS
- This case involved treating the eruption of impacted/ectopically positioned maxillary canines into the very prominent lateral incisor space, while exercising caution not to exacerbate root resorption and maintaining acceptable esthetics during tooth movement.
- The patient had no relevant medical history that could be associated with the generalized resorption exhibited radiographically.
- The decision was made to extract teeth #7 and 10, and substitute the canines for the hopelessly resorbed maxillary lateral incisors.
- Teeth #6 and 11 were satisfactorily extruded into the dental arch and cosmetically reshaped to resemble maxillary lateral incisors.
- The incorporation of a removable prosthesis with pontics during the extrusion of the maxillary canines was an integral part of patient satisfaction with treatment.
- This treatment approach improved the patient’s overbite and overjet, and the reshaped canines provided an esthetic and nonprosthetic solution for the missing maxillary lateral incisors.
REFERENCES
- Cook J, Wang HL. Canine impactions: incidence and management. Int J Periodontics Restorative Dent. 2006;26:483–491.
- Profitt WR, Fields HW, Sarver DM. Contemporary Orthodontics. 5th ed. St Louis: Mosby; 2013;422–423.
- Ericson S, Kurol J. Resorption of incisors after ectopic eruption of maxillary canines: a CT study. Angle Orthod. 2000;70:415–423.
- Walker L, Enciso R, Mah J. Three-dimensional localization of maxillary canines with cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2005;128:418–423.
- Ericson S, Kurol J. Radiographic examination of ectopically erupting maxillary canines. Am J Dentofacial Orthop. 1987;91:583–592.
- Kurol J, Ericson S, Andreason JO. The impacted maxillary canine. In: Andreason JO, Kolsen Petersen J, Laskin D, eds. Textbook and Color Atlas of Tooth Impaction. Copenhagen: Munksgaard;1997:125–175.
- Harris EF, Robinson QC, Woods MA. An analysis of causes of apical root resorption in patients not treated orthodontically. Quintessence Int. 1993;24:417–428.
- Al-Qawasmi RA, Hartsfield JK Jr, Everett ET, et al. Genetic predisposition to external apical root resorption. Am J Orthod Dentofacial Orthop. 2003;123:242–252.
- Sameshima GT, Sinclair PM. Predicting and preventing root resorption: part I. Diagnostic factors. Am J Orthod Dentofacial Orthop. 2001;119:505–510.
- Igarashi K, Adachi H, Mitani H, Shinoda H. Inhibitory effect of topical administration of a bisphosphonate (risedronate) on root resorption incident to orthodontic tooth movement in rats. J Dent Res. 1996;75:1644–1649.
- Attati I, Hammarstrom L. Root surface defects in rat molars after 1-hydroxyethylident-1, 1-bisphosphonate. Acta Odontol Scand. 1996;54:59–65.
- Villa PA, Oberti G, Moncada CA, et al. Pulp-dentine complex changes and root resorption during intrusive orthodontic tooth movement in patients prescribed nambumetone. J Endo. 2005;31:61–66.
- Poumpros E, Loberg E, Engstrom C. Thyroid function and root resorption. Angle Orthod. 1994;64:389–393.
- Shirazi M, Dehpour AR, Jefari F. The effect of thyroid hormone on orthodontic tooth movement in rats. J Clin Pediatr Dent. 1999;23:259–264.
- Loberg EL, Engstrom C. Thyroid administration to reduce root resorption. Angle Orthod. 1994;64:395–399.
- Christiansen RL. Commentary: thyroxine administration and its effects on root resorption. Angle Orthod. 1994;64:399–400.
- Brezniak N, Wasserstein A. Orthodontically induced inflammatory root resorption. Part II: the clinical aspects. Angle Orthod. 2002;72:180–184.
- Davidovitch Z, Godwin SL, Park YG, Dobeck JM, Lily CM, De Sanctis GT. The etiology of root resorption. In: McNamara JA, Trotman CA, eds. Orthodontic treatment: the management of unfavorable sequelae. Ann Arbor: University of Michigan Press; 1996;93–117.
- Otis L, Hong J, Tuncay O. Bone structure effect on root resorption. Orthod Craniofac Res. 2004;21:165–177.
- Mirabella AD, Artun J. Risk factors for apical root resorption of maxillary anterior teeth in adult orthodontic patients. Am J Orthod Dentofacial Orthop. 1995;108:48–55.
- Kaley J, Phillips C. Factors related to root resorption in edgewise practice. Angle Orthod. 1991;61:125–132.
- Segal G, Schiffman OP, Tuncay O. Meta analysis of the treatment-related factors of external apical root resorption. Orthod Craniofac Res. 2004;7:71–78.
- Newman WG. Possible etiologic factors in external root resorption. Am J Orthod. 1975;67:522–539.
- Sameshima GT, Sinclair PM. Characteristics of patients with severe root resorption. Orthod Craniofac Res. 2004;7:108–114.
- Ngan DC, Kharbanda OP, Byloff FK, Darendeliler MA. The genetic contribution to orthodontic root resorption: a retrospective twin study. Aust Orthod J. 2004;20:1–9.
- Linge BO, Linge L. Apical root resorption in upper anterior teeth. Eur J Orthod. 1983;5:173–183.
- Bishara SE, Vonwald L, Jakobsen JR. Changes in root length from early to mid-adulthood: resorption or apposition? Am J Orthod Dentofacial Orthop. 1999;115:563–568.
- Harris EF, Kineret SE, Tolley EA. A heritable component for external apical root resorption in patients treated orthdontically. Am J Orthod Dentofacial Orthop. 1997;111:301–309.
- DeShields RW. A study of root resorption in treated Class II, Division I malocclusions. Angle Orthod. 1969;39:231–245.
- Chan E, Darendeliler MA. Physical properties of root cementum: part 7. Extent of root resorption under areas of compression and tension. Am J Orthod Dentofacial Orthop. 2006;129:504–510.
- Weltman B, Vig KW, Fields HW, Shanker S, Kaizar EE. Root resorption associated with orthodontic tooth movement: A systematic review. Am J Orthod Dentofacial Orthop. 2010;137:462–476.
- Lind V. Short root anomaly. Scand J Dent Res. 1972;80:85–93.
- Puranik CP, Hill A, Henderson Jeffries K, Harrell SN, Taylor RW, Frazier-Bowers SA. Characterization of short root anomaly in a Mexican cohort — hereditary idiopathic root malformation. Orthod Craniofac Res. 2015;18:62–70.
- Shigenobu N, Hisano M, Shima S, Matsubara N, Soma K. Patterns of dental crowding in the lower arch and contributing factors. Angle Orthod. 2007;77:303–310.
- de Almeida M, Pereira A, de Almeida R, de Almeida-Pedrin R, da Silva Filho O. Prevalence of malocclusion in children aged 7 to 12 years. Dental Press J Orthod. 2011;16:123–131.
The author has no commercial conflicts of interest to disclose.
Featured photo by MICROSCAPE/SCIENCE SOURCE
From Decisions in Dentistry. January 2017;3(1):22-24, 26-27.
