
 EDWARDOLIVE / ISTOCK / GETTY IMAGES PLUS
EDWARDOLIVE / ISTOCK / GETTY IMAGES PLUS
Maximizing Dental Implant Longevity
The proper selection of implant components and regular maintenance are critical to the long-term success of implant therapy.
Modern dental implants offer predictable solutions for restoring edentulous areas1 and supporting orofacial structures; however, they also present challenges for providers and patients alike. Thus, proper treatment planning, placement and oral care — both pretreatment and posttreatment — are critical to the success of implant therapy and optimal patient health.
The American College of Prosthodontists estimates that more than 36 million Americans are edentulous, and 120 million are missing at least one tooth.2 The National Institute of Dental and Craniofacial Research reports that nearly one-third of individuals age 65 and older are edentulous.3 Patients at the greatest risk for edentulism are older adults, active smokers, patients with diabetes, and those with limited education or lower socioeconomic status.
An average implant treatment takes approximately a year to complete and is costly.4 Yet technological advances — including three-dimensional digital imaging and surgical planning software — allow implant treatments to be more accessible, safe, fast and affordable.1 With these changes, the implant market is projected to nearly double from $3.9 billion in 2018 to $7.4 billion in 2027.5 As such, dental professionals can expect a significant influx of patients seeking dental implant therapy.
DENTAL IMPLANT MATERIALS
Clinical familiarity with the materials used in dental implants is essential to successful long-term outcomes. These materials vary based on implant components, including the implant body, abutment and prosthesis (fixed or removable). Fixed partial dentures on implants can be retained with either screws or cement. Table 1 lists the materials used for fixed prostheses. Implant-supported removable prostheses used as part of overdenture, hybrid or telescopic structures can be made of acrylic, composites, polymethyl methacrylate or high-performance polymers.6
Currently, the most widely used implant materials are titanium and zirconia. Titanium, in particular, is preferred for its durability, low toxicity and high corrosion resistance. Zirconia improves esthetics, helps clinicians avoid or reduce the occurrence of soft-tissue complications, and provides an alternative for patients prone to rare allergic reactions to titanium. And while early zirconia implants were subject to fracture, modern zirconia and titanium exhibit excellent mechanical strength, fracture resistance, biocompatibility, tissue integration, and low plaque affinity.7–10
A significant disadvantage of titanium implants relates to the dark gray color of the implant body, which is especially visible in areas of thin tissue or gingival recession. The gray oxide layer on titanium’s surface, called titanium dioxide (TiO2), is formed by exposure of titanium to oxygen or water. The TiO2 layer facilitates the implant’s biocompatibility with surrounding structures. As long as this layer is intact, it prevents the release of particles and ions from the implant to neighboring tissue, minimizes foreign body reactions, and allows osseointegration to occur.11
Unlike the body of the implant, the gray shade of a titanium abutment can be masked by anodization, which allows surface color changes.12 During this process, the titanium abutment is placed in an electrolytic bath, where an electric current speeds up the oxidization process, creates a thicker oxide layer (less than 1 um), and increases surface roughness and hardness — without modifying the material’s other properties. When a precise voltage is applied, the light reflections from the titanium and oxide layer result in different surface colors. For example, 65 volts generate a gold hue used on substructures for fixed restorations, while 75 volts produce a pink surface utilized in substructures made for removable prostheses. Anodized titanium is very durable in the oral environment, but friction or scratches can still damage the surface.13
Zirconia, on the other hand, has a white, tooth-like color and exhibits lesser ion release than titanium.10,14 Disadvantages include microcracks and stress breaks attributed to many factors, including incorrect design or fabrication in which dull burs used in the milling process create minor fractures that grow under pressure and cause breakage over time.15 In addition, modifying the surface of zirconia is challenging. Yet studies show that osseointegration, surface roughness, and stress distribution in zirconia implants are comparable to those of titanium implants.10,14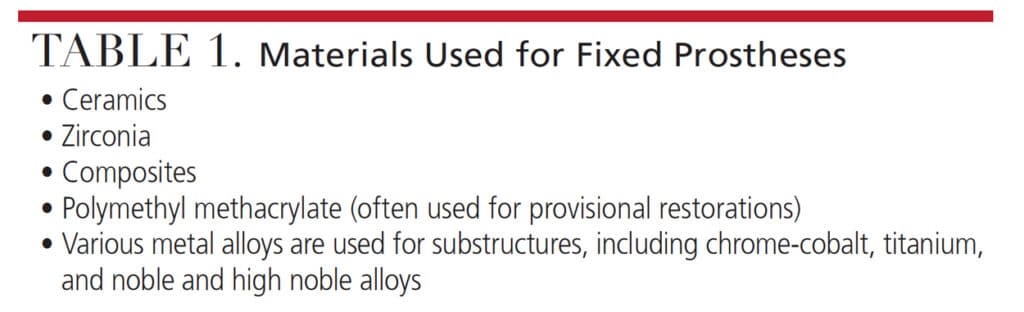
IMPLANT DESIGNS AND SURFACE TREATMENTS
Various implant designs and surface treatments influence osseointegration by generating improved biological and mechanical connections between the implant and alveolar bone. For instance, tapered implant designs add initial stability and reduce the risk of micro gaps and micro-movements.16 Mechanical, chemical and physical surface modifications can also enhance the interaction between the implant’s surface and bone, promote a longer-lasting bond, and minimize bacterial colonization to reduce the risk of biofilm formation. Moreover, surface modifications can deter the adhesion of microbes by repelling or killing pathogens, especially the species most associated with dental implant associated inflammation. But while greater surface roughness stimulates denser bone fixation, it also attracts bacterial retention, which promotes biofilm accumulation.15
Mechanical treatments are utilized to create smoother or rougher implant surfaces, and may incorporate grinding, machining or blasting. The latter technique removes parts of the implant material, creating slight irregularities and roughened surfaces. Machining leaves grooves and ridges on the implant surface, while grinding produces coarseness that contributes to better bone-implant connections.9
Chemical modifications change surface topography and composition while enhancing surface energy. These include acids, alkali, sol-gel or anodization processes.9 Acids applied to the surfaces of the implant’s body increase surface roughness and surface area. Alkali-etching creates a porous, hydrated and reactive titanium oxide surface.17 The sol-gel process deposits biocompatible hydroxyapatite to the implant’s surface to improve osseointegration and provide antibacterial and anticorrosive properties.18 Anodization is an electromechanical process that thickens and roughens the oxide layer.9,16
Physical modifications effecting connections between the implant and alveolar bone include plasma spraying and ion deposition. Plasma spraying involves using a plasma torch to spray tiny particles of metal or ceramic to create a thick coating with a high level of adhesion. The ion deposition method generates a specific pattern on the surface of an implant for better adhesion during osseointegration.9,16,19
Some surface modifications are growing in popularity, including sandblasting and acid etching. However, studies of surface modifications show variable results or suggest most implants are comparable, regardless of their morphological characteristics, surface structure or type.9,20 Research indicates that moderately rough surfaces are most favored, as biofilm is more easily removed from these surfaces than rougher variations. That said, some evidence indicates that not all biofilm should be removed from implant surfaces21 — although such assertions are subject to debate.
IMPLANT FAILURES
The long-term success of implants and prostheses depends on biological and mechanical factors, including oral hygiene and maintenance. The biological aspects contributing to implant survival include the health of the tissue and bone, whereas mechanical elements rely on the stability of the implant body and restorative components. Implant failures are often caused by inflammatory processes that lead to peri-implant mucositis (an inflammatory response of the soft tissues), and peri-implantitis (an inflammatory response of the bone).22–24 Biological failures may involve loss of bone around the implant or failure to integrate. Mechanical failures of implant components include mobility, fractures, breakage, occlusal overload or implant removal. Implant design, surface treatment, and surrounding bacteria determine how the bone grows to the top of the implant and how the tissue follows the bone.24
Most implant failures are classified as early failures, occurring before osseointegration, or late failures, taking place after implant integration and loading. Early failures occur due to the bone overheating during placement, surface contamination at the time of surgery, infections, implant placement at a site where periapical pathology existed on the extracted tooth, overloading a provisionalized, immediately placed implant, or lack of initial stability (e.g., placement in poor quality bone). Reasons for late failures include occlusal overload, parafunction and peri-implantitis. Occlusal overload occurs due to many factors, including an incorrect implant or restoration design. It can also result when not enough implants are placed to balance the occlusal load, or from large cantilevers, steep cuspal inclines, poor distribution of forces, occlusal interferences, or parafunctional habits, such as bruxing or clenching.24
In some cases, the loss of bone and soft tissue surrounding dental implants can be associated with metallosis, an inflammatory process engendered by small particles and ions of titanium25 — a finding supported by similar responses found in failed metal-on-metal joint prostheses. When acid from bacteria acts on the implant surface at the same time mechanical forces are applied (e.g., occlusal loading), increased cracking and exposure of the implant’s non-oxidated surfaces may occur.
Once corrosion emerges, bacterial attachment to the implant escalates, resulting in further corrosion. Bacterial attachment can occur within 30 minutes after implant placement, and surface corrosion can occur within two days after bacterial attachment. When bacteria, oral biofilm or mechanical forces partially destroy the TiO2 layer, the areas of exposed titanium allow the release of titanium particles and ions into the surrounding tissue. The inflammatory response is proportionate to the amount of titanium that enters the tissue — a process that can eventually lead to tissue and bone loss. It has also been determined that bone will not reattach to areas of corrosion. Besides titanium implants, similar corrosion has been found on devices made from zirconium.25
ESSENTIAL ROLE OF ONGOING CARE
Dental teams play an essential role in customizing oral care to meet patients’ needs during implant therapy. Establishing suitable oral hygiene habits to prevent the formation of biofilm-induced disease surrounding teeth and implants is vital to the success of implant therapy and maintenance. Considering that dental implants are significant investments in oral health, a three-month recare regimen should be maintained until the patient has demonstrated acceptable oral hygiene around the implants. During these visits, providers can identify biological and/or mechanical areas of concern.
In the case of cement-retained implant prostheses, any excess cement that is not removed can cause peri-implantitis, increasing the risk of bone loss and affecting the longevity of the implant. If pain is present, it most likely comes from the surrounding areas rather than the inert implant itself. Inflammation or bone loss may occur due to abutment connections linked to the smooth neck of an implant, excessive stress and strain from occlusion, parafunction, or cantilever length. Other signs of inflammation include mobility, exudate, peri-implant mucositis or peri-implantitis, which should be examined with light peri-implant probing, assessment of bleeding on probing, and radiographic examination.26–28
Compared to teeth, the calculus formed on nonporous titanium implant surfaces tends to be softer.29 Ideally, dental instruments used on smooth surfaces should produce minimal or no surface damage, which could cause bacterial colonization and affect the implant/soft tissue interface. The use of air polishers with glycine can help preserve smooth or rough implant surfaces. Hand scaling instruments, preferably made from titanium, are most effective; however, they may still scratch the implant’s surface and should be used with caution.30,31 Less aggressive means of biofilm removal may be indicated, including the use of sterile saline on a cotton pellet. This approach has been shown to allow re-osseointegration in animals.21,32 Unnecessary lateral forces via professional debridement of the surface of the post, abutment and restoration should be avoided.33 To reduce the risk of implant fractures, occlusal guards are recommended when parafunctional habits are noted.34
Oral care instructions should include detailed verbal and visual guidance throughout the treatment regimen. Afterward, the patient’s oral upkeep should be reevaluated during regularly scheduled visits. It is important to remember that mechanical plaque control is contraindicated during the postsurgical oral care and healing period; chemical agents are recommended instead.29 Patients should also avoid ordinary dental floss since leftover threads may lead to peri-implant disease.28 In light of the increasing number of dental implants in use, improvements are needed in implant maintenance protocols and research.
Professional expertise and patient compliance are both crucial to successful long-term implant outcomes. Thus, dental teams should keep abreast of the latest research and continually upgrade their clinical skills to ensure optimal care.
CONCLUSION
The demand for long-term survival of dental implants continues to evolve as patients seek innovative solutions to replace missing teeth. Developments in technique and clinical understanding, new trends in material science, and technological innovations inspire creative treatments to solve some of the most complex oral problems. When adequately executed and properly maintained, dental implants can last a lifetime.
KEY TAKEAWAYS
- Proper treatment planning, placement and oral care — both pretreatment and posttreatment — are critical to the success of dental implant therapy and optimal patient health.
- Clinical familiarity with the materials used in implants is essential to successful long-term outcomes.
- Various implant designs and surface treatments influence osseointegration by generating improved biological and mechanical connections between the implant and alveolar bone.
- Mechanical, chemical and physical surface modifications can also enhance the interaction between the implant’s surface and bone, promote a longer-lasting bond, and minimize bacterial colonization to reduce the risk of biofilm formation and peri-implant disease.
- The long-term success of implants and the prostheses used to restore them depends on biological and mechanical factors, including personal oral hygiene and regular maintenance.
- The biological aspects contributing to implant survival include the health of the tissue and bone, whereas mechanical elements rely on the stability of the implant body and restorative components.
- Implant failures are often caused by inflammatory processes that lead to peri-implant mucositis and peri-implantitis. Thus, clinical expertise and patient compliance are both crucial to successful long-term implant outcomes.
REFERENCES
- American Academy of Implant Dentistry. Types of Implants and Techniques. Available at: http/://www.aaid-implant.org/what-are-dental-implants/types-of-implants-and-techniques/. Accessed September 7, 2022.
- American College of Prosthodontists. Facts and Figures. Available at: https://www.gotoapro.org/facts-figures/. Accessed September 7, 2022.
- National Institute of Dental and Craniofacial Research. Tooth Loss in Seniors. Available at: https://www.nidcr.nih.gov/research/data-statistics/tooth-loss/seniors. Accessed September 7, 2022.
- Saghiri MA, Freag P, Fakhrzadeh A, et al. Current technology for identifying dental implants: a narrative review. Bull Natl Res Cent. 2021;45:7.
- Mazda J. Know your implant options. Inside Dent Tech. 2021;12:6–11.
- Galvis OD. A plethora of options for implants: everyday abutment selection and bar designs. Inside Dent Tech. 2020;11:38–41.
- Cionca N, Hashim D, Mombelli A. Zirconia dental implants: where are we now, and where are we heading? Periodontol 2000. 2017;73:241–258.
- Petrungaro PS. Implant esthetics in an immediate restoration protocol: Incorporating a one-piece ceramic implant design to manage compromised soft tissue volume and quality. Inside Dent. 2021;17:28–29.
- Kendall C. Dental Implant Surface Treatments: What You Need to Know. Available at: https://www.nobelbiocare.com/blog/news/dental-implant-surface-treatments-what-you-need-to-know/. Accessed September 7, 2022.
- Zeynep O, Ender K. Zirconia dental implants: a literature review. J Oral Implantol. 2011;37:367–376.
- Wang G, Li J, Lv K, et al. Surface thermal oxidation on titanium implants to enhance osteogenic activity and in vivo osseointegration. Sci Rep. 2016;6:31769.
- Birdi B, Barrie A, Ouriques F, Chay C. Innovations in implantology: Advances in surfaces, perio-prosthetic platforms, digital workflow, and materials from the single molar to the full arch. Inside Dent. 2021;17:18–26.
- Rugh A. Gold-Anodizing Titanium Abutments. Available at: https://obriendentallab.com/videos/?wchannelid=jz9lql9gw9&wmediaid=e8vf0ql6jh. Accessed September 7, 2022.
- Archibald J. The timeless art of troubleshooting: why is your zirconia breaking? Inside Dent Tech. 2020;11:30–34.
- Kligman S, Ren Z, Chung CH, et al. The impact of dental implant surface modifications on osseointegration and biofilm formation. J Clin Med. 2021;10:1641.
- Horowitz RA. Petrungaro PS. Raymond C. Implant Designs and Treatments. Available at: https://www.aegisdentalnetwork.com/tv/inside-dentistry-roundtable/s4e3. Accessed September 7, 2022.
- Šimůnek A, Kopecká D, Strnad J. Alkali treatment: new concept of titanium implant surface modification. Clin Oral Implants Res. 2004;15:4.18.
- Tranquillo E, Bollino F. Surface modifications for implants lifetime extension: an overview of sol-gel coatings. Coatings. 2020;10:589.
- Barfeie A, Wilson J, Rees J. Implant surface characteristics and their effect on osseointegration. Brit Dent J. 2015;218:E9.
- Bullis G, Shah S. Implant surface treatments: a literature review. Available at: https://glidewelldental.com/education/inclusive-dental-implant-magazine/volume-5-issue-2/implant-surface-treatments-a-literature-review/. Accessed September 7, 2022.
- Alhag M, Renvert S, Polyzois I, Claffey N. Re-osseointegration on rough implant surfaces previously coated with bacterial biofilm: an experimental study in the dog. Clin Oral Implants Res. 2008;19:182–187.
- Pirc M, Dragan IF. The key points of maintenance therapy for dental implants: a literature review. Compendium Contin Educ Dent. 2017;38:e5–e8.
- Schwarz F, Derks J, Monje A, Wang H-L. Peri-implantitis. J Periodontol. 2018;89(Suppl 1):S267–S290.
- Froum SJ, Rosen PS, Wang H. Why do implants fail? Compendium Contin Educ Dent. 2017;38:360–364.
- Wilson TG Jr. Bone loss around implants — is it metallosis? J Periodontol. 2021;92:181–185.
- Lineberry J. Implant crown restorations: considerations for deciding between cement- and screw-retained options. Inside Dent Tech. 2020;11:24–30.
- Renvert S, Hirooka H, Polyzois I, Kelekis-Cholakis A, Wang H. Diagnosis and non-surgical treatment of peri-implant diseases and maintenance care of patients with dental implants — consensus report of Working Group 3. Intern Dent J. 2019;69:12–17.
- Oral Hygiene for Implants. Available at: https://dimensionsofdentalhygiene.com/oral-hygiene-implants/. Accessed September 7, 2022.
- Gulati M, Govila V, Anand V, Anand B. Implant maintenance: a clinical update. Int Sch Res Notices. 2014;2014:908534.
- Louropoulou A, Slot DE, Barendregt DS, van der Weijdent FA. Prevention and treatment of peri-implant diseases: current evidence on cleaning of titanium dental implant surfaces. Int J Evidence-Based Prac Dental Hygienists. 2017;3:128–141.
- Hatfield S. Implant maintenance: an overview. Available at: https://www.todaysrdh.com/implant-maintenance-an-overview/. Accessed September 7, 2022.
- Kolonidis SG, Renvert S, Hämmerle CH, Lang NP, Harris D, Claffey N. Osseointegration on implant surfaces previously contaminated with plaque. An experimental study in the dog. Clin Oral Implants Res. 2003;14:373–380.
- Suzuki JB, Terracciano-Mortilla LD, Misch CE. Maintenance of Dental Implants. Available at: pocketdentistry.com/葮-maintenance-of-dental-implants. Accessed September 7, 2022.
- Najafi-Abrandabadi S, Quader AA, Ojjeh YR. Classification and selection criteria for dental ceramics. Inside Dent Tech. 2021;12:16.
From Decisions in Dentistry. October 2022;8(10):14,16,19-20.
