
 YALCINSONAT1/ISTOCK/GETTY IMAGES PLUS
YALCINSONAT1/ISTOCK/GETTY IMAGES PLUS
Managing Thermal Injury Following Endodontic Post Preparation
This case report explores iatrogenic considerations when introducing significant heat in the root canal system during post preparation
PURCHASE COURSE
This course was published in the November 2020 issue and expires November 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the November 2020 issue and expires November 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Explain the clinician’s choices, as well as clinical and iatrogenic considerations, when removing gutta-percha from a root canal to create room for a restorative post.
- Describe pertinent details of this case report, as they apply to the post preparation outcome.
- List the symptoms and possible causes for the ulcerative gingival lesion associated with endodontically treated tooth #28.
Over time, the theory of cleaning, shaping and obturating in endodontics has remained relatively constant; however, the armamentarium and technology continue to advance. The use of gutta-percha, for example, has changed from laterally compacting1 multiple gutta-percha cones to thermoplasticizing a single, large taper gutta-percha cone.2 All endodontic techniques attempt to fill canal irregularities and ultimately achieve a fluid-tight bacterial seal.2 A somewhat recent advance is the continuous wave of vertical condensation technique that utilizes an electric heat source with variable temperature settings and pre-fit pluggers.3 Thermoplasticized gutta-percha is then introduced into the canal and incrementally compacted until the cementoenamel junction is reached.
After root canal treatment, reamers, rotary files or heat sources are often used to remove gutta-percha from the coronal half to two-thirds of the canal in preparation for a post. A heat source is generally considered the least invasive method in that it is unlikely to ledge or perforate the canal, or otherwise unnecessarily remove tooth structure.4 However, current literature suggests the possibility of iatrogenic events when introducing significant heat in the root canal system, as inappropriate use can cause extensive injuries to the periodontium. The following case report presents sudden bone loss associated with an endodontically treated tooth that had a post space created using a heat source.
MATERIALS AND METHODS
A 23-year old male was referred for periodontal emergency examination of tooth #28 after presenting with a chief complaint of a bad taste in his mouth and sensitivity of a tooth that was recently treated. The history indicated he had a post placed in tooth #28 five days prior. Clinical examination revealed a white, 3- to 4-mm ulcerative lesion on the gingiva surrounding the tooth (Figure 1). The patient was not taking any medications and reported no allergies or significant medical history; he also claimed no history of tobacco use.
The patient’s dentist reported the procedure for post and core as follows: After induction of local anesthesia via an inferior alveolar nerve block, a dental dam was placed with the clamp on tooth #30. Post space was prepared in the buccal canal using a heat source to remove existing gutta-percha to working length, minus 7 mm. The canal was irrigated with 17% ethylenediaminetetraacetic acid (EDTA), followed by 2% chlorhexidine (CHX), with passive ultrasonic irrigation for 60 seconds each before being dried with sterile paper points. The fiber post was treated (outside the mouth) with 9.6% hydrofluoric acid for 20 seconds. Next, the post was cemented in the canal per the manufacturer instructions. The enamel was etched with 37% phosphoric acid, rinsed and air dried. After bonding, buildup was completed incrementally, with each layer light cured. Occlusion was checked and adjusted. Five days later, the patient called to report moderate pain and gingival ulceration.
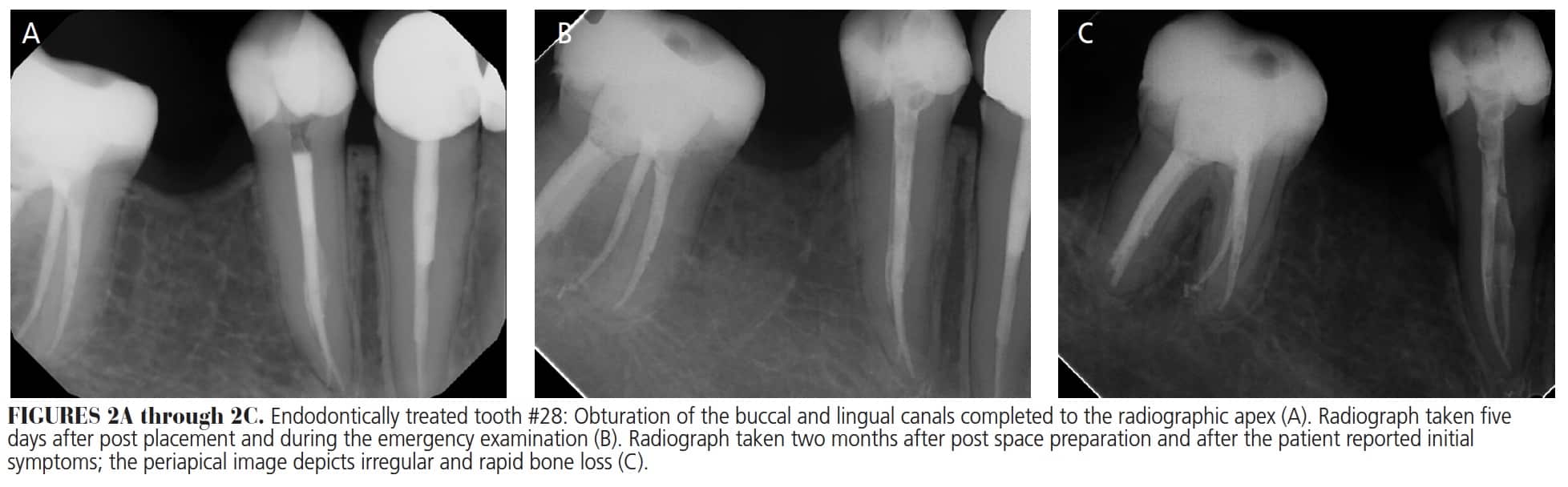
 The periodontal intraoral examination revealed the ulcerative tissue sloughed off when rubbed, and the tissue was painful to the touch. A periapical radiograph was taken, which exhibited no significant findings compared to the original periapical image (Figures 2A and 2B). The periodontal ligament (PDL) was intact, and all bone trabeculation appeared normal. The endodontic treatment was determined to be of adequate length, with the buccal and lingual canals obturated. It was unknown at this point whether the patient’s ulceration and symptoms were caused by a chemical, thermal or allergic reaction. Recommendations were for palliative care and to have the patient return in 10 days for reevaluation.
The periodontal intraoral examination revealed the ulcerative tissue sloughed off when rubbed, and the tissue was painful to the touch. A periapical radiograph was taken, which exhibited no significant findings compared to the original periapical image (Figures 2A and 2B). The periodontal ligament (PDL) was intact, and all bone trabeculation appeared normal. The endodontic treatment was determined to be of adequate length, with the buccal and lingual canals obturated. It was unknown at this point whether the patient’s ulceration and symptoms were caused by a chemical, thermal or allergic reaction. Recommendations were for palliative care and to have the patient return in 10 days for reevaluation.
At the follow-up appointment, the patient observed the white tissue had fallen off, and “now my gums are receded down.” An intraoral examination noted significant tissue recession; however, the previous symptoms were beginning to subside, so he was encouraged to continue palliative treatment with ibuprofen, as needed.
TWO MONTHS POST-PLACEMENT
The patient presented two months after post placement, and while the intraoral examination revealed no signs of an ulcerative lesion, cervical bony areas were now visible coronal to the receded gingiva. A periapical radiograph of tooth #28 exhibited an ill-defined, irregular radiolucent band extending from the alveolar crest circumferentially around mid-root level. A break in the continuity of supporting alveolar bone (with formation of sequestrum) was distinctly evident on the distal aspect (Figure 2C).
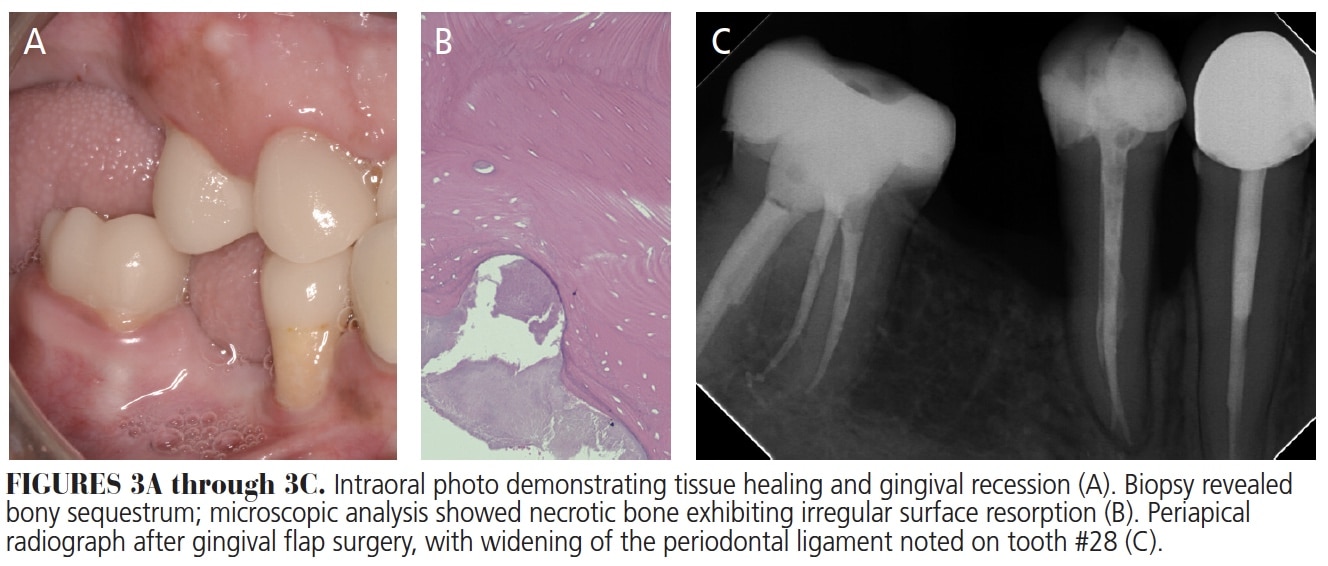
It was decided to perform gingival flap surgery to remove the affected area and obtain a biopsy sample. After anesthesia was achieved, a full-thickness intrasulcular flap was reflected in the tooth #28 area. What appeared to be necrotic bone was identified surrounding #28; it was easily flecked off with a curet and obtained for biopsy. Root instrumentation was carried out with ultrasonic and hand instruments, and the area closed with 4-0 chromic sutures. Postoperative healing proved uneventful. The patient presented for a 10-day postop evaluation and appeared to be healing well, albeit with receded gingiva (Figure 3A). The biopsy results indicated a diagnosis of sequestrum, and the microscopic description was “necrotic bone exhibiting irregular surface resorption” (Figure 3B).
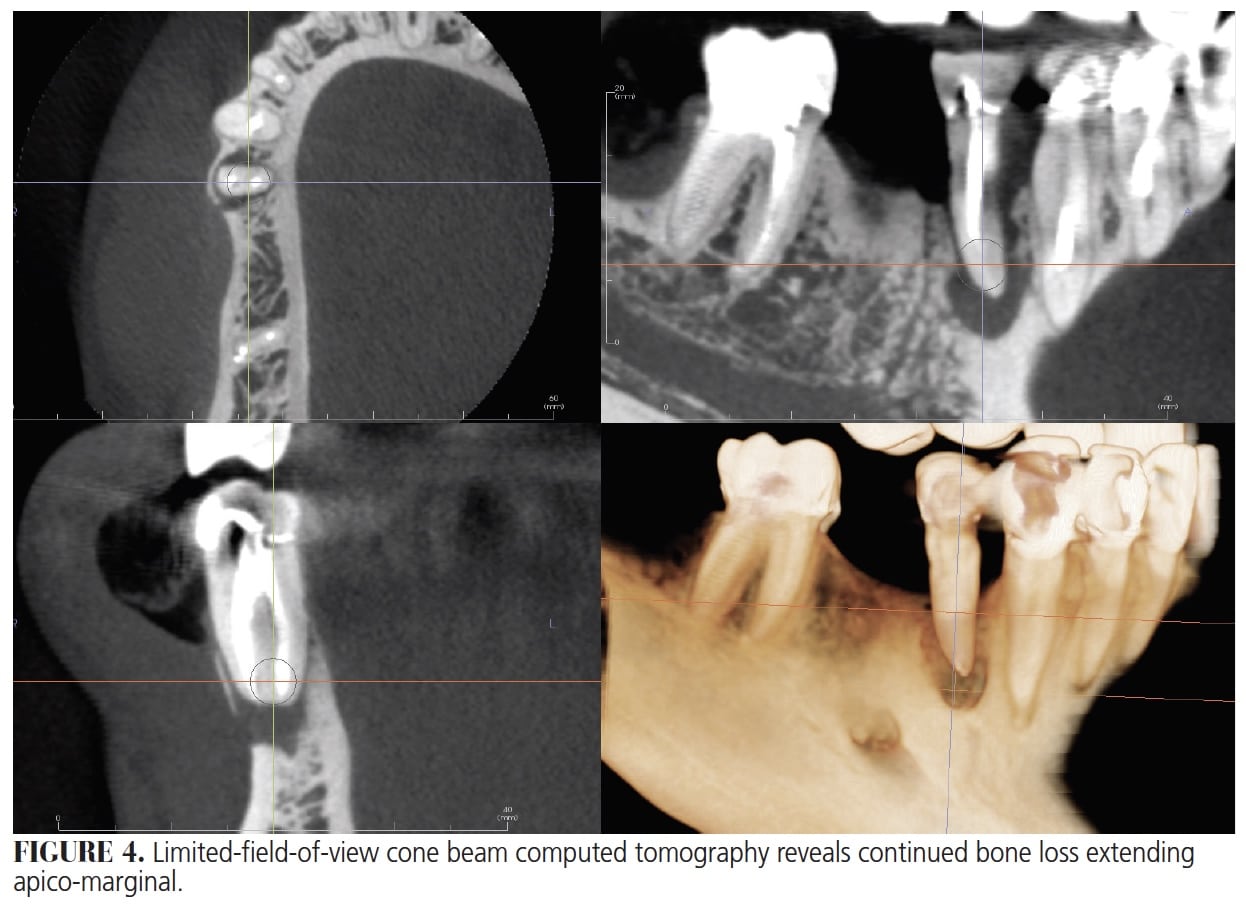
 Tooth #28 was asymptomatic and maintained for two years until recently, when a follow-up radiograph revealed periapical pathosis (Figure 3C). An endodontic evaluation was obtained. The tooth was slightly painful to percussion, normal to palpation, and had a 6-mm probing depth along the distobuccal and 7 mm along the mesial aspect. Limited-field-of-view cone beam computed tomography (Figure 4) revealed a well-obturated root canal system. Both canals showed adequate density and good apical length, with no radiographic sign of perforation. An isthmus connected the buccal and lingual canals. Irregular bone loss noted on the mesial buccal aspect appeared to be apical-marginal. The crestal bone loss was continuous, with a large, 6-mm periapical radiolucency centered on the apex of tooth #28.
Tooth #28 was asymptomatic and maintained for two years until recently, when a follow-up radiograph revealed periapical pathosis (Figure 3C). An endodontic evaluation was obtained. The tooth was slightly painful to percussion, normal to palpation, and had a 6-mm probing depth along the distobuccal and 7 mm along the mesial aspect. Limited-field-of-view cone beam computed tomography (Figure 4) revealed a well-obturated root canal system. Both canals showed adequate density and good apical length, with no radiographic sign of perforation. An isthmus connected the buccal and lingual canals. Irregular bone loss noted on the mesial buccal aspect appeared to be apical-marginal. The crestal bone loss was continuous, with a large, 6-mm periapical radiolucency centered on the apex of tooth #28.
The treatment options presented included no treatment, retreatment, or extraction. In this case, extraction was recommended due to periodontal-endodontic bone loss, a poor crown-to-root ratio, and the complexity of possible retreatment with a crown and fiber post. Further considerations included continued bone necrosis and resorption from the previous iatrogenic injury, and continued failure due to occlusion without supporting periodontium. The patient elected to have the tooth extracted.
DISCUSSION
This case report describes the diagnosis and treatment of a patient with a suspected thermal injury to the periodontium of tooth #28 caused during preparation of the post space with an electric heat source. This possibility has been extensively studied and proven in vitro. Using alginate surrounding a tooth to simulate the PDL, Romero et al5 showed that when operating at appropriately 200° C, the PDL temperature increased by only 1° to 2° C. However, research also shows that inappropriate use of a heat source can cause increased temperatures, resulting in minor injuries (such as hyperemia and fat cell deposition6) or more significant damage, including ankylosis,7 bone resorption and bone necrosis.6,8 Eriksson and Albrektsson6 reported an increase of 6° to 10° C above body temperature in the apical periodontium as the terminal temperature. Similarly, Dominici et al9 demonstrated damage to periodontal structures resulting from the significant heat created by the use of ultrasonics during post removal.
The ulcerative tissue sloughing and subsequent bone necrosis in this case appear similar to a thermal injury case report by Schwartz and Robbins10 that resulted from overuse of ultrasonic instrumentation. However, few in vivo studies describe tissue sloughing and bone necrosis caused by a heat source used for obturation.
While many studies have shown that a properly used electric heat source is safe to the periodontium, it is possible for temperatures to rise above recommended manufacturer and literature guidelines. The recommended device temperature is 200° C. However, temperatures can easily rise to levels as high as 600° C. In this case, it is the authors’ hypothesis that intracanal temperatures increased to where the PDL reached the terminal level of 43° to 47° C.
 A chemical cause of the foregoing seems unlikely. The dental dam and all restorative materials appeared to be used properly, and it did not seem likely that topical chemical irritation could cause such severe damage to the underlying bone in such a short period. Furthermore, the operator reported using EDTA and CHX during post placement, which are relatively inert to biologic tissues.11 An apical extrusion of irrigants is also unlikely considering the apical bone (at two month follow-up) remained intact, while more coronal bone had been destroyed. In addition, the patient did not present with symptoms typically seen in a hypochlorite accident.12 The intraoral ulceration and radiographic presentation of bone loss also led the authors to rule out the possibility of root perforation.
A chemical cause of the foregoing seems unlikely. The dental dam and all restorative materials appeared to be used properly, and it did not seem likely that topical chemical irritation could cause such severe damage to the underlying bone in such a short period. Furthermore, the operator reported using EDTA and CHX during post placement, which are relatively inert to biologic tissues.11 An apical extrusion of irrigants is also unlikely considering the apical bone (at two month follow-up) remained intact, while more coronal bone had been destroyed. In addition, the patient did not present with symptoms typically seen in a hypochlorite accident.12 The intraoral ulceration and radiographic presentation of bone loss also led the authors to rule out the possibility of root perforation.
It is possible there was a malfunction in the heat unit itself. Retrospectively, it was reported that during use the unit display did not appear to be working and the temperature setting went blank. Yet the unit could still have been producing heat. It is possible the dial was increased to terminal temperatures the operator did not identify.
CONCLUSION
Periodontal thermal damage, while extensively studied in vitro, is seldom reported in the literature. Terminal temperatures representing a 6° to 10° C increase above body temperature in the apical periodontium can be reached during endodontic treatment with a heat source; thus, care should be taken to understand manufacturer recommendations while using heat in these procedures. Nonetheless, while it is possible to have a faulty unit, the operator is ultimately responsible for maintaining treatment devices and ensuring their proper function and use.
References
- Cailleteau JG, Mullaney TP. Prevalence of teaching apical patency and various instrumentation and obturation techniques in United States dental schools. J Endod. 1997;23:394–396.
- Buchanan LS. Continuous wave of condensation technique. Endod Prac. 1998;1:7–10,13–16,18.
- Wu MK, Kast’akova A, Wesselink PR. Quality of cold and warm gutta-percha fillings in oval canals in mandibular premolars. Int Endod J. 2001;34:485–491.
- Mattison GD, Delivanis PD, Thacker RW Jr., Hassell KJ. Effect of post preparation on the apical seal. J Prosthet Dent. 1984;51:785–789.
- Romero AD, Green DB, Wucherpfennig AL. Heat transfer to the periodontal ligament during root obturation procedures using an in vitro model. J Endod. 2000;26:85–87.
- Eriksson AR, Albrektsson T. Temperature threshold levels for heat-induced bone tissue injury: a vital-microscopic study in the rabbit. J Prosthet Dent. 1983;50:101–107.
- Atrizadeh F, Kennedy J, Zander H. Ankylosis of teeth following thermal injury. J Periodontal Res. 1971;6:159–167.
- Eriksson RA, Albrektsson T. The effect of heat on bone regeneration: an experimental study in the rabbit using the bone growth chamber. J Oral Maxillofac Surg. 1984;42:705–711.
- Dominici JT, Clark S, Scheetz J, Eleazer PD. Analysis of heat generation using ultrasonic vibration for post removal. J Endod. 2005;31:301–303.
- Schwartz RS, Robbins JW. Post placement and restoration of endodontically treated teeth: a literature review. J Endod. 2004;30:289–301.
- Jeansonne MJ, White RR. A comparison of 2.0% chlorhexidine gluconate and 5.25% sodium hypochlorite as antimicrobial endodontic irrigants. J Endod. 1994;20:276–278.
- Hulsmann M, Hahn W. Complications during root canal irrigation — literature review and case reports. Int Endod J. 2000;33:186–193.
From Decisions in Dentistry. November 2020;6(10): 34-35.

