
 WATANYOU/ISTOCK/GETTY IMAGES PLUS
WATANYOU/ISTOCK/GETTY IMAGES PLUS
Managing Supernumerary and Ectopic Teeth
Early diagnosis and evaluation for genetic health conditions are key to providing comprehensive, patient-centered care for this population.
PURCHASE COURSE
This course was published in the October 2021 issue and expires October 2024. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the October 2021 issue and expires October 2024. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify the prevalence of supernumerary and ectopic teeth.
- Describe clinical and radiographic presentations of supernumerary and ectopic teeth.
- Discuss treatment protocols for ectopic teeth.
The appearance of supernumerary teeth (ST), or hyperdontia, is a developmental anomaly defined as any teeth or tooth structure outside of the normal series of deciduous or permanent dentition.1,2 These teeth can be unilateral or bilateral and single or multiple. They may involve both arches, and can be associated with deciduous and permanent dentitions.1–3 Ectopic eruption of teeth into the dental environment is common; however, ectopic eruption of a tooth in other sites is rare. Cases of ectopic ST have occurred in the nasal cavity, maxillary sinus, palate, mandibular condyle, coronoid process, orbit and chin.4–11 This article provides an overview of ST and ectopic teeth, as well as a case report of a supernumerary ectopic tooth in the maxillary right sinus.
In general, the prevalence of ST in the deciduous dentition is between 0.2% and 0.8%, while the prevalence of ST in the permanent dentition is between 0.5% and 5.3%.1 This condition is most common in men, with a male-to-female ratio of 2:1. These teeth tend to present more frequently in the maxilla,12 and are seen more often in the midline region with men and the incisor region in women.13
The etiology of ST is multifactorial, and multiple theories only partially explain their formation. Theories regarding ST etiology include:12–16
- Atavism or phylogenetic related to ancestral tooth tissues
- Tooth germ dichotomy
- Heredity
- Progress zone theory
- Unified etiology
- Hyperactivity of the dental lamina
Hyperactivity of dental lamina is the most commonly accepted etiology; however, the role of genetic or environmental factors in causing hyperactivity is still unknown.12
Although ST can be idiopathic and occur sporadically, most cases are related to syndromic diseases with familial heredity. Idiopathic ST presents as a single tooth approximately 80% of the time, while 15% to 20% of cases demonstrate two ST. Three ST are present about 3% to 4% of the time, and more than four ST occur in less than 1% of cases.12,17,18 Inheritance patterns of genetic diseases with ST include autosomal dominant (AD) nonsyndromic, autosomal recessive, or an X-linked chromosome (XL).19–22

Multiple ST are rare and often manifest in syndromic genetic diseases, such as:13,19,20,22,23
- Cleidocranial dysplasia (AD)
- Gardner syndrome (AD)
- Ehlers-Danlos syndrome (AD)
- Fabry-Anderson syndrome (XL)
- Familial adenomatous polyposis (AD)
- Trichorhinophalangeal syndrome Type I (AD)
- Rubinstein-Taybi syndrome (AD)
- Nance-Horan syndrome (XL)
- Opitz G/BBB syndrome (AD)
- Culofaciocardiodental syndrome (XL)
- Robinow syndrome (AD)
An evaluation of current literature suggests the genetic association with Ehlers-Danlos syndrome and Fabry-Anderson syndrome is weak.20 In addition, two rare diseases have suspected ST associations: Kreiborg-Pakistani syndrome and Ellis-van Creveld syndrome — however, more research is needed to confirm a positive correlation. Individuals with nonsyndromic cleft lip and cleft palate also have a greater incidence of ST.22–24
Ectopic teeth are not uncommon, and are most often formed in the palate and maxillary sinus.25,26 These teeth are present across the lifespan, and may appear in children through older adults.27,28 The prevalence of ectopic tooth eruption is unknown, and the mechanism of ectopic tooth formation is still not fully understood. Possible etiologies include trauma, embryonic factors involving different stages of tooth development, atavism, and genetic and developmental abnormalities.13,25,27,29
A recent longitudinal case study surmised that ectopic tooth eruption is a gradual process of mineralization and is genetically regulated independent of normal tooth development.25 In this study, the patient presented with an ectopic tooth in the maxillary sinus. During a 6-year follow-up, scans revealed the development of an additional supernumerary ectopic tooth that gradually mineralized from the crown to the root after adolescence. This suggests a congenital bone defect remaining after embryonic development in the maxillary sinus may serve as the germinal center for the ectopic tooth, and gene regulation is activated at a different time than normal tooth eruption.
![TABLE 1. Pathologic Conditions That May Be Associated With Unerupted Supernumerary Teeth1,30]() Clinical Presentation of Supernumerary Teeth
Clinical Presentation of Supernumerary Teeth
Clinically, ST are classified based on their position and morphology. Positional variations include mesiodens, paramolars, distomolars and parapremolars. The frequency of occurrence based on position varies according to different studies.30 Classification of ST based on morphology is associated with two types: normal shapes and sizes (or eumorphic), and abnormal shapes and sizes (dysmorphic). Dysmorphic ST present in particular forms, such as conical, tuberculate, infundibular or molariform.
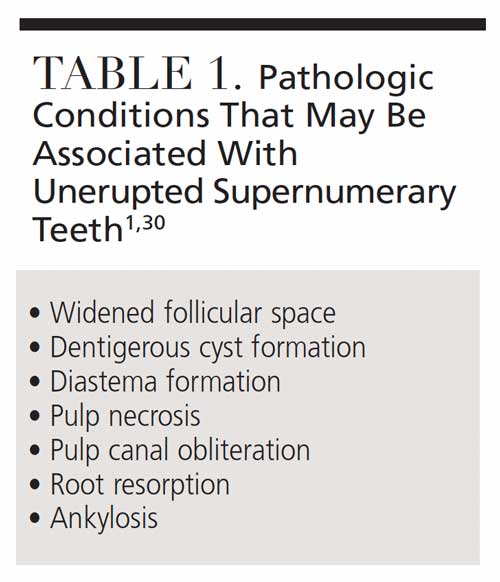
Unerupted ST may be related to pathologic conditions (Table 1).1,30 While most ST are asymptomatic, some ST erupt in the oral cavity. These teeth either erupt normally, are inverted, or become impacted. Other complications include malpositions of teeth, root changes, development of dentigerous cysts, increased caries risk, loss of vitality of adjacent teeth, elevated risk for periodontal disease, and occlusal disturbances.2,12,30,31 These teeth may also interfere with bone grafting and implant placement.3
Ectopic ST may be asymptomatic or present with a variety of signs and symptoms, such as nasal obstruction, rhinorrhoea, nasal congestion, pain, chronic inflammation, persistent discharge and crusting, nasal bleeding, septal abscess and fistula formation, and external nasal deviation. These symptoms can be long-standing, recurrent, and unresponsive to systemic therapy with antibiotics and corticosteroids.24–32
Differential Diagnosis and Diagnosis
Clinical considerations for differential diagnosis of ectopic ST include compound odontoma, complex odontoma, and dentigerous cysts. Compound odontomas resemble a small collection of teeth and are usually found in the maxillary area, while complex odontomas are a mass of enamel, dentin, cementum and pulp typically found in the mandibular region.33–35 In most cases, ectopic ST are found in the periapical regions, but, in rare instances, they may be found radiographically in the maxillary sinus.36 These masses are opaque in nature, resembling a toothlike structure, and may be accompanied by a radiolucent halo.35
Dentigerous or follicular cysts are the second most common odontogenic cysts, and are the most common developmental cyst of the jaws. They are found surrounding the crown of an unerupted tooth and are attached to the tooth cervix at the cementoenamel junction. They present as well-defined unilocular radiolucencies, with displacement of the unerupted tooth on occasion.35
Diagnosis of ectopic ST or ST requires the following:1,3,12,37
- Thorough medical history
- Clinical examination
- Radiographs, including panoramic imaging and cone beam computed tomography (CBCT)
Three-dimensional CBCT scans provide an accurate view of internal and external structures on a 360° axis prior to surgical removal of the tooth.38 Early diagnosis of ST can be important, as this condition may be indicative of syndromic and genetic diseases. As such, a referral for genetic counseling and further medical evaluation should be considered.
Treatment and Prognosis
Management of ST depends on the type, position and potential complications, such as a delay in eruption, displacement of teeth, presence of pathological lesions, occurrence of radicular resorption, or eruption of the ST.39 While surgical excision is the treatment of choice for ST, this approach may be hindered by the presence of surrounding oral structures. Currently, there is no clear consensus on the appropriate time to remove ST.12
Multiple surgical approaches are used to remove ST, with the most common being palatal-lingual, as most ST are located in a lingual position.40 However, other methods may be appropriate, such as when ectopic ST erupt into the sinus. The Caldwell-Luc procedure is recommended for this extraction.41–43 It is performed with a vestibular incision from the lateral incisor to the second molar. An osteotomy is made, gaining access to the maxillary sinus for extraction of the ectopic ST.41
Nasal endoscopy can also be used in the removal of an ectopic ST to minimize postoperative discomfort.44,45 Nasal cavity ventilation expansion surgery is another method to extract the ectopic tooth.25 The prognosis for surgical access and removal of ectopic ST or ST is good. Full recovery and elimination of symptoms are typically observed.41–43
Case Report
A 16-year-old female presented for a regular dental visit in 2021. She had no major surgeries or any known medical complications. The patient did not take any medications or supplements, and did not have any allergies. She had been routinely seen at her dental home, and a panoramic radiograph was recommended to note the development of third molars. A review of the clinical examination and radiographs revealed conservative dental restorations on the mesial of tooth #3 and the occlusal of #19. No other significant dental findings were noted from previous visits.
Upon radiographic examination, a unilocular corticated mixed lucent-opaque lesion was found lateral to the nasal cavity in the maxillary right sinus (Figure 1). The lesion was not present on intraoral examination, and the patient did not report experiencing any symptoms of the ectopic ST. Because it is usually asymptomatic, ectopic ST eruption in the maxillary sinus can be discovered accidentally during routine radiographic or clinical evaluation.41
The patient was advised the ectopic tooth would be observed, as it caused no discomfort. The future treatment plan included the dentist removing the ectopic ST when the wisdom teeth were extracted. The patient and her guardian gave consent for these planned procedures.
Conclusion
Supernumerary and ectopic teeth are distinctive disorders that are more common in men, in the maxilla, and in the permanent dentition. Complications may include impactions, delayed eruptions, recurrent sinus infections, and formation of other pathologies. Management of ST and ectopic ST depends on their type, position, and potential for complications. Early diagnosis and evaluation for genetic health conditions are important for comprehensive, patient-centered care.
References
- Hajmohammadi E, Najirad S, Mikaeili H, et al. Epidemiology of supernumerary teeth in 5000 radiography films: investigation of patients referring to the clinics of Ardabil in 2015–2000. Int J Dent. 2021;2021:6669436.
- Shetty S, Agarwal N, Shetty P, et al. Twin supernumerary teeth: a tale of two cases. Can J Dent Hyg. 2019;53:67–71.
- Parolia A, Kundabala M, Dahal M, et al. Management of supernumerary teeth. J Conserv Dent. 2011;14:221–224.
- Elango S, Palaniappan SP. Ectopic tooth in the roof of the maxillary sinus. Ear Nose Throat J. 1991;70:365–356.
- Dayal PK, Dewan SK, Bihani VK, et al. Eruption of a tooth into the nasal cavity due to osteomyelitis. J Layrngol Otol. 1981;95:509–512.
- Pracy JP, Williams HO, Montgomery PQ. Nasal teeth. J Laryngol Otol. 1992;106;366–367.
- Carver DD, Peterson S, Owens T. Intranasal teeth. Oral Surg Oral Med Oral Pathol. 1990;70:804–805.
- Spencer MG, Couldery MG. Nasal tooth. J Laryngol Otol. 1985;99:1147–1150.
- Gadalla GH. Mandibular incisor and canine ectopia. A case of two teeth in the chin. Br Dent J. 1987;163:236.
- De Felice R, Lombardi T. Ectopic third molar in the maxillary sinus. Aust Dent J. 1995;40:236–237.
- Kim DH, Kim JM, Chase SW, et al. Endoscopic removal of an intranasal ectopic tooth. Int J Pediatr Otorhinolaryngol. 2003;67:79–81.
- Ata-Ali F, Ata-Ali J, Peńarrocha-Oltra D, et al. Prevalence, etiology, diagnosis, treatment and complications of supernumerary teeth. J Clin Exp Dent. 2014:6:e414–e418.
- Anthonappa RP, Omer RS, King NM. Characteristics of 283 supernumerary teeth in southern Chinese children. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105:e48–e54.
- Brooke AH. A unifying aetiological explanation for anomalies of human tooth number and size. Arch Oral Biol. 1984;29:373–378.
- Lui JF. Characteristics of premaxillary supernumerary teeth: A survey of 112 cases. ASDC J Dent Child. 1995;62:262–265.
- Primosch RE. Anterior supernumerary teeth — assessment and surgical intervention in children. Pediatr Dent. 1981;3:204–215.
- Bereket C, Cakir-Ozhhan N, Sener I, et al. Analyses of 1100 supernumerary teeth in a nonsyndromic Turkish population: a retrospective multicenter study. Niger J Clin Pract. 2015;18:731–738.
- Acikgoz A, Acikgoz G, Tunga U, et al. Characteristics and prevalence of non-syndrome multiple supernumerary teeth: a retrospective study. Dentomaxillofac Radiol. 2006;35:185–190.
- Takahashi M, Hosomichi K, Yamaguchi T, et al. Whole-exome sequencing analysis of supernumerary teeth occurrence in Japanese individuals. Hum Gen Variation. 2017;4:16046.
- Lubinsky M, Kantaputra PN. Syndromes with supernumerary teeth. Am J Med Genet. 2016;170:2611–2613.
- de Souza Batista FR, Bonardi JP, Silva LF, et al. Supernumerary teeth in non syndrome patient. J Craniofac Surg. 2017;28:583–584.
- Subasioglu A, Savas S, Kucukyilmaz E, et al. Genetic background of supernumerary teeth. Eur J Dent. 2015;9:153–158.
- Cammarata-Scalisi F, Avendaño A, Callea M. Main genetic entities associated with supernumerary teeth. Arch Argent Pediatr. 2018;116:437–444.
- Moller LH, Pradel W, Gedrange T, Botzenhart UU. Prevalence of hypodontia and supernumerary teeth in a German cleft lip with/without palate population. BMC Oral Health. 2021;21:1–7.
- Lui J, Zhou M, Liu Q, et al. Process of ectopic tooth formation in the maxillary sinus: follow-up observation of one case. J Int Med Res. 2019;47:6356–6364.
- Kratz B, Chhabra N. Ectopic tooth of the nasal cavity. Ear Nose Throat J. 2020;99:NP13–NP14.
- Lombroni LG, Farronato G, Santamaria G, et al. Ectopic teeth in the maxillary sinus: a case report and literature review. Indian J Dent Res. 2018;29:667–671.
- Gupta YK, Shah N. Intranasal tooth as a complication of cleft lip and alveolus in a four year old child: case report and literature review. Int J Paediatr Dent. 2001;11:221–224.
- Agrawal M, Khan TS, Gupta T, Khanna S. Intranasal tooth: ectopic eruption 1 year after maxillofacial trauma. BMJ Case Rep. 2014;2014:bcr2014204432.
- Chalakkal P, Krishnan R, De Souza N, et al. A rare occurrence of supplementary maxillary lateral incisors and a detailed review on supernumerary teeth. J Oral Maxillofac Pathol. 2018;22:149.
- Rajab LD, Hamdan MA. Supernumerary teeth: Review of the literature and a survey of 152 cases. Int J Paediatr Dent. 2002;12:244–254.
- Accorona R, Colombo G, Ferrari M, et al. Inverted supernumerary intranasal teeth as unusual indications of endoscopic surgery. Iran J Otorhinolaryngol. 2020;32:181–186.
- Dokania V, Kinnera H, Shweta S, et al. Ectopic deciduous maxillary tooth in the nasal cavity following trauma. Cureus. 2021;13:e14154.
- Erkmen N, Ölmez S, Önerci M. Supernumerary tooth in the maxillary sinus; Case report. Aust Dent J. 1998;43:385–386.
- DeLong L, Burkhart NW. General and Oral Pathology for the Dental Hygienist. 3rd ed. Philadelphia: Wolters Kluwer; 2019:450–475.
- Visioli AR, Silva CO, Marson FC, et al. Giant complex odontoma in maxillary sinus. Annals Maxillofacial Surg. 2015:5:123–126.
- Chen KC, Huang JS, Chen MY, et al. Unusual supernumerary teeth and treatment outcomes analyzed for developing improved diagnosis and management plans. J Oral Maxillofacial Surg. 2018;77:920–931.
- Liu DG, Zhang WL, Zhang ZY, et al. Three-dimensional evaluations of supernumerary teeth using cone-beam computed tomography for 487 cases. Oral Med Oral Pathol Oral Radiol Endo. 2007;103:403–411.
- Shah A, Gill DS, Tredwin C, et al. Diagnosis and management of supernumerary teeth. Dent Update. 2008;35:510–520.
- Ferres-Padro E, Prats-Armengol J, Ferres-Amat E. A descriptive study of 113 unerupted supernumerary teeth in 79 pediatric patients in Barcelona. Med Oral Patol Oral Cir Bucal. 2009;14:E146–E152.
- Kayabasoglu G, Karaman M, Kaymaz R, et al. A rare entity causing chronic sinusitis: ectopic tooth in maxillary sinus. European Journal of General Medicine. 2015;12(1):86–89.
- Buyukkurt MC, Tozoglu S, Aras MH, et al. Ectopic eruption of a maxillary third molar tooth in the maxillary sinus. J Contemp Dent Pract. 2005;3:1–4.
- Dhingra S, Gulati A. Teeth in rare locations with rare complications: an overview. Indian J Otolaryngol Head Neck Surg. 2015;67:438–440.
- Priya M, Doomra S, Angral S, et al. Supernumerary tooth: endoscopic removal for a rare cause of recurrent epistaxis. Indian J Otolaryngol Head Neck Surg. Epub: October 17, 2020.
- Saleem T, Khalid U, Hameed A, et al. Supernumerary, ectopic tooth in the maxillary antrum presenting with recurrent haemoptysis. Head Face Med. 2010:6:1–3.
From Decisions in Dentistry. October 2021;7(10):26-28,31.

