

Beaded Implants — Do They Last?
This case report involves the placement of three lower anterior beaded implants that have been followed over a 17-year period of successful integration and function.

The interest in dental implants has grown exponentially since Linkow introduced the blade in 1967. Since that time, many different implants have come to the market in an attempt to develop the ideal shape and surface texture for long-term success. Except for some early implants made from materials such as carbon,1 carbon fiber2 and sapphire,3 most modern implant bodies are made from titanium; some are smooth, some are coated, and some are specially treated to provide a textured surface to enhance bone ingrowth and attachment.
In the 1980s, a company named Innova introduced the Endopore dental implant system, which was designed at the University of Toronto by Deporter, Watson and Pillar. Although this unique beaded implant design is no longer on the market, this paper will present a case report involving the placement of three lower anterior Endopore implants that have been followed over a 17-year period of successful integration and function.
By way of background, the Endopore implant has a 5-degree truncated shape made of a high-strength Ti6A14V alloy cone, with a multilayer porous surface over most of its length. The porous surface was achieved by sintering spherical particles, which create the possibility of three-dimensional bone ingrowth (Figure 1). It was first used in humans in 1989.

This implant system was distinctly different from others because the implant was made with a proprietary design incorporating a surface of interlocking beads. The resulting mechanical interlocking of bone and implant at the interface provided an effective means of force transfer between the implant and peri-implant tissues, including the ability to effectively transfer tensile forces. Both the axial and transverse force components (tensile, shear and compressive) acting on the implant are effectively resisted, resulting in a more uniform distribution of mechanical stresses in the peri-implant bone. As a result, peak stresses next to the most coronal portion of the porous-surfaced implant are significantly lower compared to the stresses that would occur with a threaded implant because the forces are distributed more uniformly.4
The design of the Endopore implant allowed for ease of placement, three-dimensional ingrowth of bone (and thus greater resistance to torque), and faster healing. The truncated-conical design provided better distribution of stress and more leeway for error when placed adjacent to vital structures or in narrow regions of bone.5 Due to the increased surface area provided by the novel beaded design, shorter devices could be used in many cases. With this device, it was often possible to avoid sinus lifts or other augmentation procedures in the maxilla and mandible, allowing for less patient morbidity and implant reconstruction that was potentially less traumatic and more affordable for the patient.6

Despite these advantages, the device never gained popularity due to concerns the beaded design would result in rapid epithelial ingrowth and/or that infection would invade the interconnecting beads, resulting in immediate failure. A search of the literature does not substantiate these concerns, but, instead, presents multiple articles reporting both short- and long-term success in the mandible and maxilla.6–10 At this time, no negative reports regarding the use of this implant were found in the literature.
Case Report
In October 2003, the patient in this case report presented with the chief complaint that he wanted to replace his lower anterior removable partial denture (RPD). The existing appliance was loose and had irritated the soft tissue around the anterior abutment teeth. Upon examination, the patient was missing anterior teeth #22, 23, 24, 25 and 26 due to an accident 20 years earlier. The remaining residual alveolar ridge was resorbed both from an occlusal and buccal-lingual dimension. After a complete oral examination, diagnostic models (Figure 2), as well as panoramic (Figure 3) and periapical radiographs were taken. Cone beam computed tomography was not used for this case due to lack of significant anatomical structures in the lower anterior region and minimal depth of soft tissue in this area.

After reviewing all the diagnostic information, the patient was presented with two treatment options to replace the existing RPD: a new RPD involving more posterior teeth for added support and retention, or an implant-supported fixed partial denture (FPD). He chose the implant option, noting he was “dissatisfied with his current RPD and wanted something that did not come out.”
Using topical anesthesia, the minimal width of the residual anterior ridge was obtained by inserting a periodontal probe into the soft tissue in the general location of the proposed implants and recording the depth of soft tissue covering the bone on the incisal, buccal and lingual areas. Then, by subtracting this from the total width of the ridge as measured on the study model, the remaining bone height/width was obtained. Based on this measurement, the decision was made to place three Endopore implants, which were chosen because their beaded surface allowed placement in an area of minimal bone support.

The proposed treatment plan involved placing three implants to support a five-unit lower anterior FPD. In addition, the placement of these implants would be possible without the need for bone grafting due to the available sizes and increased surface area of this particular implant system.
Measurements of the study casts and radiographs indicated that three 9×3.5-mm implants could be used, placed in the positions of sites #22, 23 and 26, and an acrylic surgical guide was fabricated with holes over the proposed implant sites. Owing to the morphology of these devices, the effective load-bearing properties of the three short implants would be equivalent to three traditional, longer implants (which would otherwise be needed to withstand the shear loads placed on the lower anterior teeth during normal biting and chewing).
Under minimal local infiltration anesthesia, the implants were placed without complications in April 2004. When exposed during surgery, as suspected, the remaining alveolar ridge was knife-edged. Therefore, removal of 2 mm of the crestal bone produced an acceptable ridge width, and all implants were placed level to the height of the residual ridge (Figure 4). The tissue was sutured with a continuous 4-0 silk suture and the patient was given instructions on proper postoperative care. The patient was contacted that night and reported no discomfort or edema.
Three Months for Post-Placement
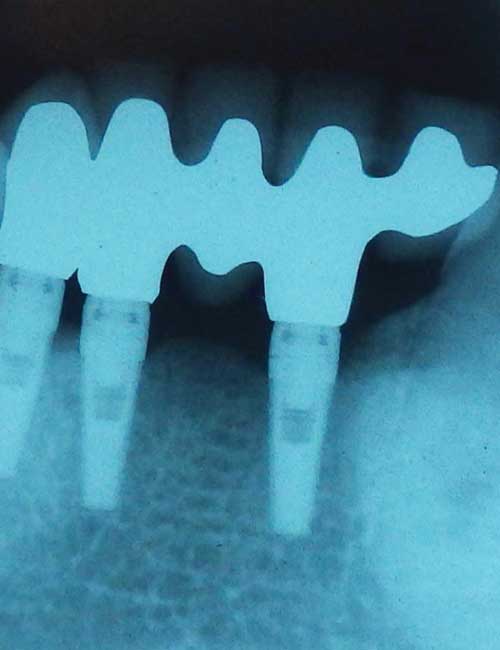
Three months post-placement, the patient returned and the implants were exposed, impression analogs were placed (Figure 5) and impressions taken to fabricate a five-unit FPD. Two weeks later, the framework was tried in and a passive fit was verified. It was returned for the addition of porcelain. The patient returned again in another two weeks for final cementation (Figures 6A and 6B). He was given additional instructions on the care and proper hygiene necessary to ensure long-term implant success.
Subsequent to the placement of these implants, Sybron, which currently owns the Innova implant system, stopped producing the Endopore implant due to the lack of wide-scale acceptance of its design and the vast improvement of the traditional, screw-type implant systems on the market. Another overriding factor leading to discontinuing this implant design was the high production cost of the beaded coating. Therefore, Sybron removed the Endopore platform from its production and inventory.
Long-Term Follow-Up
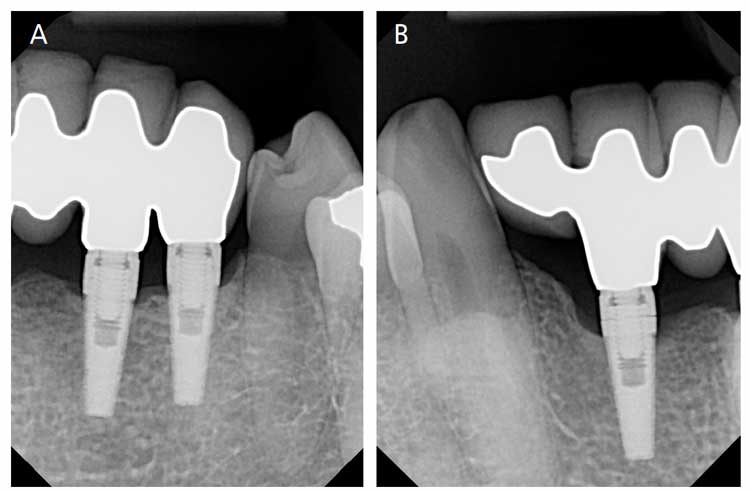
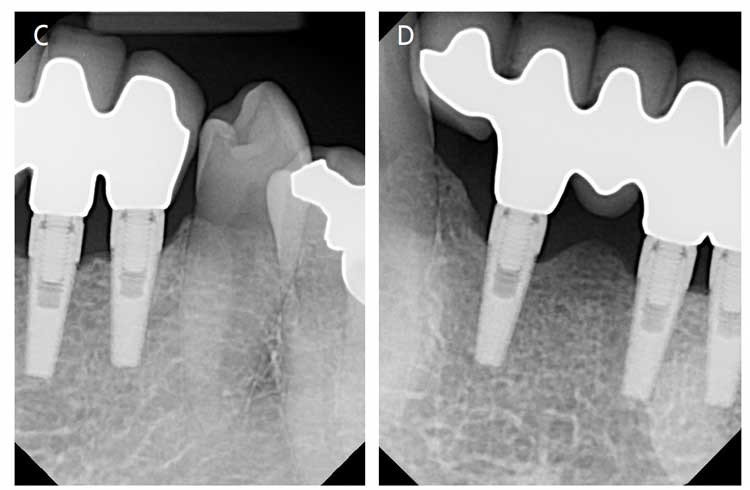
As a follow-up on this case, the patient has been contacted on an annual basis to see how his FPD is performing. He reports maintaining his routine biannual dental examinations with his primary general dentist, and has no issues with his new FPD. In addition, all reports have been positive and he always comments that his FPD is so much better than the RPD it replaced (Figures 7A and 7B).
In early 2018, the patient was contacted once again and asked to get follow-up radiographs and photos of the implant-supported FPD to further document how the tissue and bone appeared after 14 years. His primary dentist saw him for routine care in February 2018, and, with the patient’s approval, sent radiographs for review (Figures 7C and 7D). The patient was last contacted in July 2021, 17+years post-placement, and reported that he and his primary dentist are pleased with the FPD and, to date, have no issues with the health of the supporting bone and soft tissue. In addition, the patient took photos of his mouth in July 2021 and forwarded them (Figure 8).

Although short-lived, the Endopore implant system provided the dentist/implantologist an interesting alternative design in a period when hard tissue adaption/integration was in question. Many thought the design was flawed and that infection would surely spread rapidly down the entire implant body through the interconnecting spaces created by the sintered beads. As stated earlier, this turned out to be untrue — and, in this case, also proved not to be an issue over many years of service. When the implant bodies were properly placed, apical migrating infection did not occur. As can be seen in this case, due to hygiene issues there is evidence of plaque and calculus formation on the gingival area of site #23 (Figure 8), but there is no apical migration of soft tissue or beaded surface exposure over this 17-year period, and the bone height has not migrated apically (compare the 2014 periapical radiographs Figures 7A and 7B with Figures 7C and 7D from 2018).
Conclusion
While the Endopore and other implants are no longer in production, dentists should be familiar with all forms of devices that patients may present with. The Endopore implant is unique in its design, and, due to the beaded surface, if it needs to be removed it presents a difficult surgical challenge. Since the bone may have grown into the undercuts provided by the beaded surface, the entire device will need to be removed in a block section. If necessary, an alternative would be to bury the implant and provide a new treatment plan working around the remaining Endopore device.
Patients should be comfortable selecting implants as an alternative to traditional RPDs and FPDs. As this case shows, when placed following the manufacturer’s guidelines, dental implants can provide many years of service. They can replicate the function of the natural dentition while providing an acceptable cosmetic appearance without the embarrassment of an appliance coming loose or falling out.

Key Takeaways
- Most modern implant bodies are made from titanium; some are smooth, some are coated, and some are specially treated to provide a textured surface to enhance osseointegration.
- In the 1980s, Innova introduced the Endopore implant that featured a unique beaded design to encourage three-dimensional bone ingrowth and attachment.
- Although no longer on the market, this implant system provided potential advantages compared to other designs of that period. This case report documents long-term follow-up of a patient with three successful beaded implants.
- Owing to its beaded surface, this device produced mechanical interlocking of bone and implant at the interface, which provided an effective means of force transfer between the implant and peri-implant tissues.
- This beaded device also allowed for ease of placement, three-dimensional ingrowth of bone (and thus greater resistance to torque), and faster healing.
- The implant’s truncated-conical design helped distribute stress and allowed more leeway for error when placed adjacent to vital structures or in narrow regions of bone.5
- Despite these advantages, the device never gained popularity due to concerns the beaded design would result in rapid epithelial ingrowth and/or infection.
- A search of the literature does not substantiate these concerns. In fact, at this time, no negative reports regarding the use of this implant were found.
- Although the beaded implant is no longer in production, dentists should be familiar with all forms of devices patients may present with.
References
- Hottel TL. Effects of surface structure of carbon implants on the gingival morphology. Case Western Reserve University Biomedical Engineering Masters Thesis: Cleveland, Ohio; 1975.
- Adams D, Williams DF, Hill J. Carbon fiber-reinforced carbon as a potential implant material. J Biomed Mater Res. 1978;12:35–42.
- Takahashi T, Sato T, Hisanaga R, et al. Long-term observation of porous sapphire dental implants. Bull Tokyo Dent Coll. 2008;49:23–27.
- Shafie H. Endopore Dental Implant System. Available at: https://pocketdentistry. com/12-endopore-dental-implant-system/. Accessed September 8, 2021.
- Fleming AE. The Endopore dental implant system: implant treatment simplified. J Can Dent Assoc. 1994;60:785–789.
- DePorter DA, Todescan R, Watson PA, Pharoah M, Pilliar RM, Tomlinson G. A prospective human clinical trial of Endopore dental implants in restoring the partially edentulous maxilla using fixed protheses. Int J Oral Maxillofac Implants. 2001;16:527–536.
- Zheng XY, Le JC. Application of Endopore implant in inadequate alveolar bone. J Clin Rehab Tissue Eng Res. 2008;12:7093–7096.
- Deporter D, Watson P, Pharoah M, Levy D, Todescan R. Five-to-six-year results of a prospective clinical trial using the Endopore dental implant and a mandibular overdenture. Clin Oral Implants Res. 1999;10:95–102.
- Deporter DA, Kermalli J, Todescan R, Atenafu E. Performance of sintered, porous-surfaced, press-fit implants after 10 years of function in the partially edentulous posterior mandible. Int J Perio Rest Dent. 2012;32:563–570.
- Deporter D, Todescan R, Watson PA, Pharoah M, Levy D, Nardini K. Use of the Endopore dental implant to restore single teeth in the maxilla: protocol and early results. Int J Oral Maxillofac Implants. 1998;13:262–272.
From Decisions in Dentistry. October 2021;7(10)16-18,22.
