
 HELIN LOIK-TOMSON/ISTOCK/GETTY IMAGES PLUS
HELIN LOIK-TOMSON/ISTOCK/GETTY IMAGES PLUS
Substance Use Disorders Among Dentists
An examination of work-life areas that may contribute to substance use disorders in the dental profession — and solutions to mitigate their impact.
PURCHASE COURSE
This course was published in the October 2021 issue and expires October 2024. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the October 2021 issue and expires October 2024. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe substance use and addictions affecting dental personnel, and factors that contribute to the development of substance use disorders (SUDs).
- Explain triggers and potential consequences associated with SUDs among dentists, including burnout and suicide.
- Discuss preventive efforts, treatment approaches, and resources available to dentists who develop SUDs.
The expression “ignoring the elephant in the room” may sometimes reflect the dental team’s reaction to a dentist who is abusing drugs or alcohol. The office atmosphere may become tense because staff members may suspect or know of substance abuse by the dentist, but are afraid to say anything due to fear of termination or making unsubstantiated accusations. This may create a “conspiracy of silence” within the team, who acts as if nothing is wrong — a dynamic that may serve as a protective mechanism to maintain a sense of normalcy.
Most of the research on substance use disorders (SUDs) and professional health programs (PHPs) that help advocate for, and monitor, healthcare professionals in recovery involves physicians. However, it is reasonable to expect dentists to respond in similar fashion to the same treatment recommendations, support systems, and outcomes as physician-based PHPs. This article will discuss the prevalence of SUDs among dentists, and the corresponding relationship to stress, depression, burnout and suicide in dentistry. The discussion will center on work-life areas that may contribute to SUDs — and present solutions to mitigate the impact of such disorders.
Often misunderstood, SUDs frequently carry negative connotations. It is important to define and understand this condition and its implications, as this will help oral health professionals seek mitigation strategies for effective management.
Also known as addiction, SUD is defined as a primary, chronic disease of brain reward, motivation, memory and related circuitry. Dysfunction in these circuits leads to characteristic biological, psychological, social and spiritual manifestations. This is reflected in an individual pathologically pursuing reward and/or relief through substance use and other behaviors.1
Addiction is characterized by the inability to consistently abstain from use, despite negative consequences. The person with addiction may exhibit impairment with emotional responses and behavioral control, including cravings and a diminished recognition of significant problems with one’s behaviors and interpersonal relationships. Like other chronic diseases, addiction often involves cycles of relapse and remission. Without treatment or engagement in recovery efforts, addiction is progressive and can result in disability or premature death.1
As with most chronic illnesses, 40% to 70% of a person’s risk for developing an SUD is genetic,2 but numerous environmental factors interact to modify risk, such as being raised in a home in which the parents or relatives used alcohol or drugs,3,4 or living in neighborhoods and going to schools with a high prevalence of alcohol and/or drug misuse.3,5,6
The good news is that addiction is a treatable chronic disease involving complex interactions among brain circuits, genetics, the environment, and an individual’s life experiences. Individuals with addiction use substances or engage in behaviors that become compulsive; fortunately, prevention efforts and treatment approaches are generally as successful as those developed for other chronic diseases.1
Substance Use By Dentists
Some dentists use specific drug groups to deal with stressors and pain. These include alcohol, opiates, benzodiazepine, illicit drugs and nitrous oxide. According to data, alcohol is the drug of choice for 37% of dentists with substance abuse problems, while 31% use opioids, 10% consume street drugs, and 5% abuse nitrous oxide.7 According to the U.S. Substance Abuse and Mental Health Services Administration, at least 100,000 medical professionals struggle with an SUD.8 Understandably, this disorder occurs across all demographics and professions. Healthcare professionals, including dentists, are no exception, with estimates that 10% to 15% of healthcare providers experience SUDs.9 In 2020, there were 201,117 licensed dentists in the United States.10 This would represent approximately 20,000 to 30,000 dentists with SUDs, or one in every six to 10 dentists.
One of the most uncomfortable situations a dentist can experience is when he or she knows of a colleague who is suspected of abusing alcohol and/or drugs. However, it is clear what the concerned dentist’s ethical duty is in this setting. The American Dental Association’s (ADA) Principles of Ethics and Code of Professional Conduct states that practitioners have an ethical obligation and responsibility to report colleagues who are suspected of being impaired.11 Often, peer assistance committees (available through the ADA and local or state dental boards) may be able to help those who need an evaluation and potentially receive treatment in lieu of discipline.
Factors Behind Substance Absuse
The enjoyment of working with patients who are in need of preventive, restorative and reconstructive care can give purpose and direction to a dentist’s life. However, the stressors associated with dentistry can be taxing if a healthy work-life balance is not achieved. Unfortunately, some dentists turn to excessive alcohol and/or drug use to alleviate this stress. Contributing factors that may lead to SUD include being isolated in practice, having access to controlled substances, dealing with perfectionistic and/or obsessive-compulsive tendencies, not effectively managing time and stress (which may lead to burnout), living with untreated or undertreated depression, and the individual’s genetic vulnerabilities to addiction.
The reasons dentists use drugs and/or alcohol for relief may be related to a study that reported the primary reasons physicians in a PHP misused prescription drugs were to manage physical pain, emotional/psychiatric distress, and/or stressful situations.12 The were also used for recreational purposes or to avoid withdrawal symptoms.12
Stress and Depression
Researchers have found that about half of individuals who experience an SUD during their lives will also experience a co-occurring mental disorder, and vice versa. Co-occurring disorders can include stress/anxiety disorders, depression, attention-deficit hyperactivity disorder, bipolar disorder, personality disorders and schizophrenia, among others.13
Stressors in dentistry can include managing a solo practice, missed appointments, patient dissatisfaction with treatment, insurance problems, encroachment and regulations of government or oversight agencies, and the lack of quiet time (such as not having work breaks).14–16
As a group, dentists may also gravitate toward perfectionistic tendencies, which may make for precise restorations, but lead to disappointments in life and practice. Dentists should view mistakes as opportunities for growth, and their dental career as a journey; meaning, they should accept failures and learn from them while remaining humble and teachable in order to make the changes necessary to achieve excellence, not perfection.17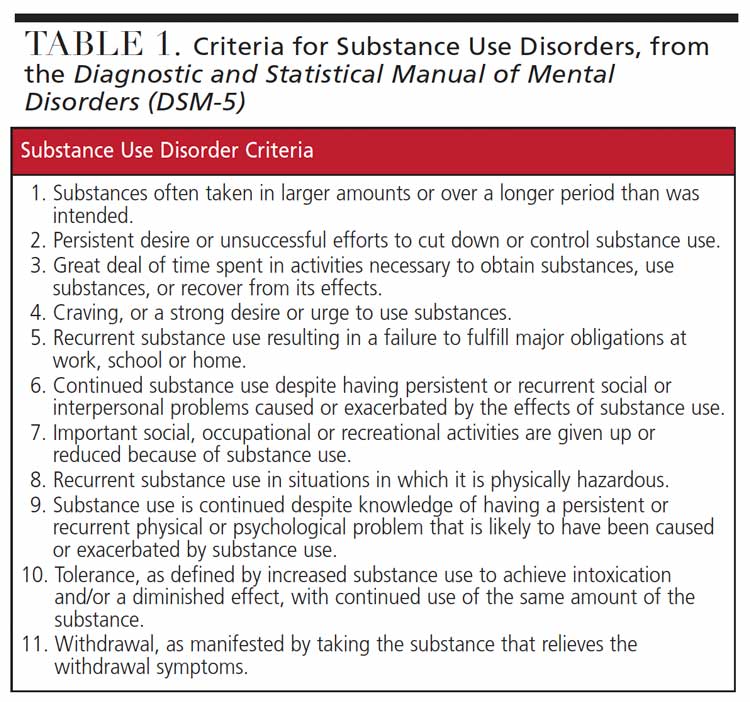
Burnout
Maslach et al18 addressed these stressors in their research surrounding burnout and how workplace conditions may lead to this condition. One area that is often difficult to manage is work-life balance.19 The authors identified six major job mismatches that may lead to burnout and potential substance use, including work overload, lack of control, insufficient reward, breakdown of community, absence of fairness, and conflicting values. In the dental office, these issues must be addressed in order to reduce the daily stressors of practice. Furthermore, if the actual source of the stressors is not addressed, nothing will change. It is important to realize that in most cases it is not the individual, but, rather, the work environment that leads to burnout and potential substance abuse.20,21
Poor scheduling is a major trigger for stress in the dental office that may lead to frustration, burnout, and eventual substance abuse. In a study of salaried primary care dentists, the most common work-related stressors included time constraints or patient scheduling (26.5%), challenging or anxious patients (26.0%), poor managerial skills or support (21.4%), administrative burdens (13.5%), excessive workload (12.5%), and staffing issues (11.8%).22
Research has linked burnout and substance use in physicians to “broken relationships, problematic alcohol use, and suicidal ideation.”20 As compared to the general population, multiple studies have found a significantly higher risk of alcohol use disorder, as well as a much greater risk of suicide in physicians experiencing burnout. One such study found that, compared to the general public, male surgeons were 13.9% more likely and female surgeons 25.6% more likely to develop an alcohol abuse disorder. The authors attributed these increased risks to higher levels of burnout and depression.21 It is not unreasonable to expect dentists to exhibit similar issues and outcomes, especially in light of the ADA Wellness Survey that reveals some potentially disturbing and destructive behaviors.23
Suicide
Each year, 300 to 400 U.S. physicians commit suicide;24 comparatively, dentists represent about 80 suicide deaths annually in the U.S.25 The U.S. Centers for Disease Control and Prevention (CDC) ranks the healthcare profession as No. 11 among the top 30 jobs for suicide probability.25 The CDC notes that professions with high suicide rates may see greater risks because of job-related isolation and demands, stressful work environments, work-home imbalance, financial pressures, and access to lethal means.14–16 More than 90% of suicides are associated with depression and other mental illnesses or SUDs. Most suicidal individuals are depressed and have a high risk of harming themselves; in dentistry, this is exacerbated by providers who isolate, will not seek help, and/or have poor management skills.15,26–28
While dentistry has long had the image of having the highest suicide rate of any profession, research indicates a lack of substantial evidence to support this claim. Alexander14 found that such analyses were flawed by the use of hearsay, public perceptions, assumptions, and outdated information. Furthermore, he asserts there is no consistent statistical evidence to prove that dentists are suicide prone; in fact, most reliable evidence suggests the opposite.14 Reports that dentists have high suicide rates often do not take into account the scientific weight of:
- Underreporting due to the stigma of guilt, shame and religious implications
- Demographic variables
- Previous psychiatric comorbidities before becoming a dentist
- Stressors unrelated to work
- Genetics/heredity14
Advocacy and Resources
In 1974, the American Medical Association acknowledged physician impairment from alcoholism and drug dependence. With the advice and consent of the American Medical Association and Federation of State Medical Boards, plans were launched for the development of therapeutic alternatives in lieu of automatic discipline of physicians who needed assistance. By 1980, all but three medical societies in the United States had authorized or implemented PHPs. In 1987, the American Medical Association called all drug addictions diseases.29 From these models, dental PHPs emerged and are now available in all 50 states.30
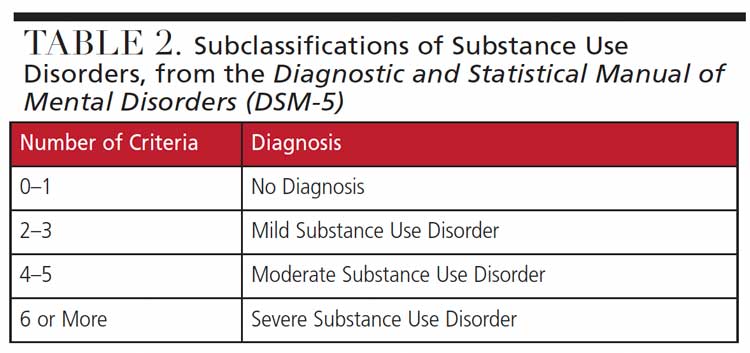
In general, if a clinician suspects a problem with substance use, an initial evaluation and diagnosis are made by mental health professionals who work in the field of addiction. They will help determine the degree of care (if necessary) to help the dentist establish abstinence and begin recovery efforts (Table 1 and Table 2).
If a dentist has been diagnosed with an SUD, he or she may be assisted by a healthcare recovery program. Such efforts are based on the physician model of a five-year contract with monitoring. Physician recovery appears to occur independently of the professional specialty or substance of abuse. Most PHPs will continue to monitor the provider and offer periodic drug screening, support groups, and ongoing treatment, if necessary.31 Similarly, if the dentist is compliant with treatment recommendations, these programs offer advocacy before state boards, insurance companies, and other official organizations. As noted, operators in every state have access to dental programs based on the PHP model that help clinicians navigate and monitor progress through the recovery process. This model is considered the gold standard of care, and long-term studies show 78% of participants had no positive test for either alcohol or drugs over the five-year period of intensive monitoring. Furthermore, this five-year posttreatment follow-up demonstrates 72% of participating physicians continued to practice.31 These figures underscore there is hope, support, and a future for anyone in dentistry who takes the first step to reach out. The ADA, local or state dental societies, and state healthcare programs offer assistance to help providers address and successfully manage SUDs.
Conclusion
In closing, SUDs should be viewed as a dilemma rather than a problem with a simple solution. A dilemma implies the answers are found by developing a strategy to address the underlying issues. A plan to treat an SUD may consist of an evaluation, possible treatment, and ongoing, long-term recovery efforts. In today’s practice environment, there has never been a better time for a dentist to ask for, and receive, help with substance abuse and mental health issues.
References
- American Society of Addiction Medicine. Definition of Addiction. Available at: https://www.asam.org/Quality-Science/definition-of-addiction. Accessed September 7, 2021.
- Goldman D, Oroszi G, Ducci F. The genetics of addictions: uncovering the genes. Nat Rev Gen. 2005;6:521–532.
- Hawkins JD, Catalano RF, Miller JY. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: implications for substance abuse prevention. Psychol Bull. 1992;112:64–105.
- Kilpatrick DG, Acierno R, Saunders B, et al. Risk factors for adolescent substance abuse and dependence: data from a national sample. J Consult Clin Psychol. 2000;68:19–30.
- Mayberry ML, Espelage DL, Koenig B. Multilevel modeling of direct effects and interactions of peers, parents, school, and community influences on adolescent substance use. J Youth Adolesc. 2009;38:1038–1049.
- Marschall-Lévesque S, Castellanos-Ryan N, Vitaro F, Séguin JR. Moderators of the association between peer and target adolescent substance use. Addictive Beh. 2014;39:48–70.
- Curtis EK. When Dentists Do Drugs: A Prescription for Prevention. Available at: https://www.dentistwellbeing.com/pdf/DentistsDoDrugs.pdf. Accessed September 7, 2021.
- Bush DM, Lipari RN. Substance use and substance use disorder by industry. Substance Abuse and Mental Health Services Administration. Center for Behavioral Health Statistics and Quality. 2015.
- Baldisseri MR. Impaired healthcare professional. Care Med. 2007;35(Suppl 2):S106–S116.
- American Dental Association Health Policy Institute. Supply of Dentists in the U.S.: 2001–2020. Available at: https://www.ada.org/en/science-research/health-policy-institute/dental-statistics/workforce. Accessed September 7, 2021.
- American Dental Association. The Principles of Ethics and Code of Conduct. Available at: https://www.ada.org/en/about-the-ada/principles-of-ethics-code-of-professional-conduct. Accessed September 7, 2021.
- Merlo LJ, Supachoke S, Cummings SM, Cottler LB. Reasons for misuse of prescription medication among physicians undergoing monitoring by a physician health program. J Addict Med. 2013;7:349–353.
- National Institute of Mental Health. Substance Use and Co-Occurring Mental Disorders. Available at: https://www.nimh.nih.gov/health/topics/substance-use-and-mental-health. Accessed September 7, 2021.
- Alexander RE. Stress-related suicide by dentists and other health care workers. Fact or folklore? J Am Dent Assoc. 2001;132:786–794.
- Stein GM. Challenging the myth of the suicide-prone dentist. Northwest Dent. 2004;83:35–38.
- Fung EY, Lange BM. Impact of drug abuse/dependence on dentists. Gen Dent. 2011;59:356–359.
- Curran T, Hill AP. Perfectionism is increasing over time: A meta-analysis of birth cohort differences from 1989 to 2016. Psychol Bull. 2019;145:410–429.
- Maslach C, Jackson SE, Leiter MP. Maslach Burnout Inventory Manual. 3rd ed. Palo Alto, Calif: Consulting Psychologists Press; 1996.
- Kalliath T, Brough P. Work-life balance: A review of the meaning of the balance construct. J Management Org. 2008;14:323–327.
- Oreskovich MR, Kaups KL, Balch CM, et al. Prevalence of alcohol use disorders among American surgeons. Arch Surg. 2012;147:168–174.
- Shanafelt TD, Boone S, Tan L, et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012;172:1377–1385.
- Kemp M, Edwards H. Sources of Work-Related Stress Among Salaried Primary Care Dentists in the UK. Available at: https://bda.org/about-the-bda/campaigns/Documents/Sources%20of%20stress%20among%20salaried%20dentists.pdf. Accessed September 7, 2021.
- American Dental Association. ADA Wellness Survey — 2015. Available at: https://success.ada.org/en/wellness/ada-wellness-survey-2015. Accessed September 7, 2021.
- Anderson P. Physicians Experience Highest Suicide Rate of Any Profession. Available at: https://www.medscape.com/viewarticle/896257. Accessed September 7, 2021.
- Gawe R. Suicide and Dentistry: Myths, Realities, and Prevention. Available at: https://www.dentistrytoday.com/news/todays-dental-news/item/1098-suicide-and-dentistry-myths-realities-and-prevention. Accessed September 7, 2021.
- Maletic V, Robinson M, Oakes T, Iyengar S, Ball SG, Russell J. Neurobiology of depression: An integrated view of key findings. Int J Clin Pract. 2007;61:2030–2040.
- Belmaker RH, Agam G. Major depressive disorder. N Engl J Med. 2008;358:55–68.
- Paykel ES. Basic concepts of depression. Dialogues Clin Neurosci. 2008;10:279–289.
- The sick physician. Impairment by psychiatric disorders, including alcoholism and drug dependence. JAMA. 1973;223:684–687.
- American Dental Association. Dental Well Being Handbook. Available at: https://ebusiness.ada.org/productcatalog/2311/Center-for-Professional-Success/Dental-Well-Being-Handbook/CPS_LV010. Accessed September 7, 2021.
- McLellan AT, Skipper GS, Campbell M, DuPont RL. Five year outcomes in a cohort of physicians treated for substance use disorder in the United States. BMJ. 2008;337:a2038.
From Decisions in Dentistry. October 2021;7(10):32-35.

