

Managing Dental Patients With HIV
The dental team can play an important role in all phases of the human immunodeficiency virus (HIV) care continuum — from diagnosis to disease management.
The dental team can play an important role in all phases of the human immunodeficiency virus care continuum — from diagnosis to disease management
The authors have no commercial conflicts of interest to disclose.
This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the treatment cascade in human immunodeficiency
virus (HIV) infection. - Identify how the dental team can help patients with HIV
maintain their health. - Explain the basic tenets of treating patients with HIV.
- Detail the role that dental practices can play in HIV testing.
According to the CDC, 1.2 million individuals are living with HIV, and about 50,000 new cases are diagnosed each year in the U.S.1 Although the incidence of HIV is greatly reduced, for an infection that can be prevented, rates are still unacceptably high. The focus should be on prevention, early identification, and linkage and retention to primary care, which, by definition, includes oral health services. The dental team continues to be a vital component in each of these areas.2
HIV is a retrovirus that leads to immune deficiency in humans. It can be transmitted during sexual intercourse from an infected to an uninfected partner, when sharing equipment used to inject drugs, during pregnancy, labor and delivery, and through breastfeeding. Infection can also occur during exposure to the blood of an infected patient via needlestick or a splash to exposed mucous membranes. It is important to point out that 34 years into this pandemic, there have been no documented cases of HIV seroconversion from patient to dental health care worker after an exposure in the dental setting. There are numerous reasons why this has not occurred, including the implementation of standard precautions and post-exposure prophylaxis. While there is no vaccine or cure, effective treatment is available to control HIV, support the immune system and prolong life. Unlike the early days of the epidemic, HIV is now considered a chronic condition; however, HIV remains a serious medical concern. Prevention of new infections is a primary goal in the White House’s National AIDS Strategy and among public health authorities. The oral health care team can be an important part of this mission.
DISEASE MANAGEMENT
 The advances achieved in the medical management of HIV are remarkable. New classes of medications and combination therapies have enabled many individuals to achieve an undetectable HIV viral load and live long, fruitful lives. Undetectable viral load also greatly reduces the chances of transmission from an infected to an uninfected patient, which demonstrates the critical role that treatment plays in the prevention of new cases.3
The advances achieved in the medical management of HIV are remarkable. New classes of medications and combination therapies have enabled many individuals to achieve an undetectable HIV viral load and live long, fruitful lives. Undetectable viral load also greatly reduces the chances of transmission from an infected to an uninfected patient, which demonstrates the critical role that treatment plays in the prevention of new cases.3
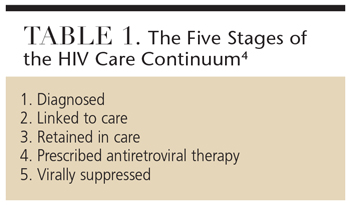
Current efforts to manage HIV infection use a concept called the “treatment cascade,” first described by Edward Gardner, MD, and colleagues to estimate awareness of infection, engagement and retention in care, receipt of antiretrovirals (ARVs), and viral suppression. The CDC suggests using this as a method for policymakers and providers to create systems to improve outcomes. Models of the HIV care continuum used by federal and state agencies to improve service delivery across the entire continuum consist of five stages (Table 1).4 The cascade begins with diagnosis; approximately 14% of infected Americans are unaware of their status.1,5 Each of these stages is an opportunity for the dental team to intervene and affect engagement in care.
The cascade provides a visual for these interventions. The vision for HIV prevention and care, as stated by the U.S. Department of Health and Human Services, is that “the United States will become a place where new HIV infections are rare and when they do occur, every person regardless of age, gender, race/ethnicity, sexual orientation, gender identity or socioeconomic circumstance, will have unfettered access to high quality, life-extending care, free from stigma and discrimination.”6 The dental team is vital to this vision.
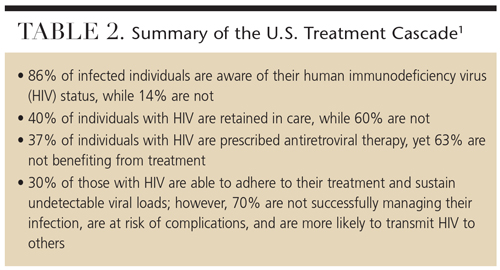 The fact that so many Americans remain unaware of their HIV status and so few individuals with HIV are virally suppressed is unacceptable. The oral health care team should be vigilant in recognizing oral manifestations that may be related to HIV infection, so they can link patients to appropriate care (Table 2).1
The fact that so many Americans remain unaware of their HIV status and so few individuals with HIV are virally suppressed is unacceptable. The oral health care team should be vigilant in recognizing oral manifestations that may be related to HIV infection, so they can link patients to appropriate care (Table 2).1
Over the past 34 years, significant advances have been made in HIV testing and treatment. Whereas in 1986 only one U.S. Food and Drug Administration-approved ARV was available, now there are 37, including combination medications. While in 1986 there was one class of drugs, today there are seven, with two more in clinical trials. These drug classes target the many opportunities HIV has to invade a cell, reproduce, depart the cell, and go on to infect other cells.7
COLLABORATION IS KEY
There are many opportunities for dental, medical, and support teams to collaborate to ensure patients with HIV are linked to medical and dental care, retained in care, and adhere to their prescribed treatment regimens. This is where the intersection of oral-systemic associations is important.
The dental team should advise patients to consent to communications across their health care teams. During the taking of a medical history, clinicians should find out the name of the patient’s medical provider. All health care team members have the opportunity to advise patients of the importance of retention in medical and dental health care.
The oral health care team has a unique opportunity during a health history intake or update to discuss a patient’s HIV care, including a discussion of medication use. Dental professionals can emphasize to patients the importance of adhering to their treatment regimens and discuss how this can promote oral health. With consent to contact medical and support teams, oral health professionals can communicate any oral issues or concerns. In turn, the medical and support teams can underscore the importance of routine oral health care and disclosure of status and medical concerns. Medical teams should inquire if their patients have a dentist of record and whether they’ve received professional oral health care. They should be prepared to refer, as needed.
Collaborating as a team will enhance patients’ health. In 2003, an expert panel of medical and dental educators released a report, “Improving the Oral Health Status of All Americans: Roles and Responsibilities of Academic Dental Institutions: the Report of the American Dental Education Association President’s Commission,” that asserts the shared responsibility of the dental and medical professions to ensure the oral health of the public.8 This recommendation supports the concept of creating a health home that incorporates medical and dental care to create a patient-centered approach to health.
The oral health care team can also help achieve an AIDS-free generation. In 2010, the White House released the National HIV/AIDS Strategy with three goals for 2015:9
- Reduce the number of people who become infected with HIV
- Increase access to care and optimize health outcomes for individuals with HIV/AIDS
- Decrease HIV-related health disparities
These strategies recognize that while progress has been made, not all people with HIV benefit equally from the gains made, and the burden of HIV infection varies greatly across states, race, ethnicity and gender.
ORAL HEALTH MANAGEMENT
There are several points to note when managing a patient with HIV/AIDS in the dental setting. The first concern is what lab values the office needs and the interval at which they should be made available. A measure of patients’ CD4, or Tcell count and viral load should be included in a referral and/or medical history, as most patients have these labs checked every six months. The cascade’s definition of retention is two medical visits at least three months apart within one year. Many patients will know their CD4 count and viral load information. Many asymptomatic patients with undetectable HIV viral load and CD4 counts greater than 300 cells/mm3 will have these labs taken on an annual basis.
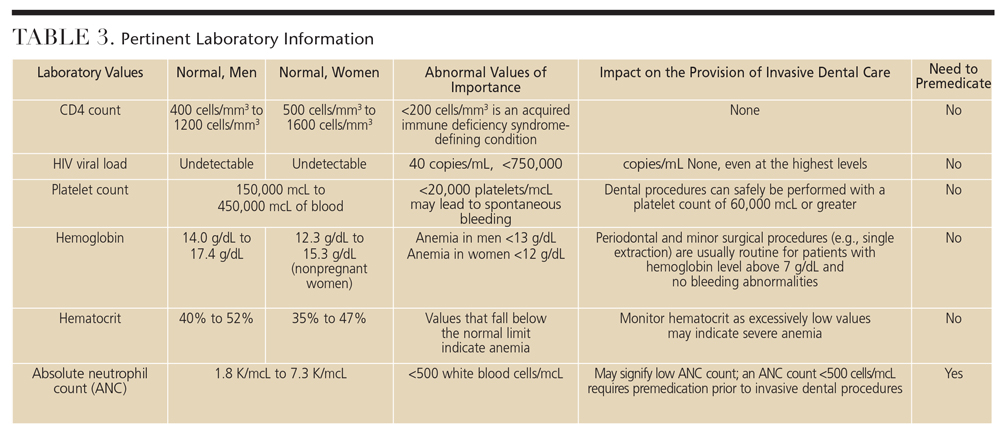 For symptomatic patients or individuals with a CD4 count less than 300 cells/mm3, the following labs should be collected: platelet count, absolute neutrophil count, CD4 count and HIV viral load (Table 3).2
For symptomatic patients or individuals with a CD4 count less than 300 cells/mm3, the following labs should be collected: platelet count, absolute neutrophil count, CD4 count and HIV viral load (Table 3).2
The second question dental professionals may ask is if patients with HIV/AIDS who have low CD4 counts or high viral loads need antibiotic premedication. Current recommendations suggest that no premedication is needed based on CD4 count or viral load. Evidence reveals that patients with low CD4 counts or high viral loads have similar complication rates compared to those without HIV/AIDS.10 The only time premedication is needed, based on lab values alone, is when the absolute neutrophil count is 500/mcL or less.11
It’s not uncommon for clinicians to question the safety of using high-speed handpieces or ultrasonic scalers when treating patients with HIV/AIDS. The CDC statement on aerosols and HIV defines aerosols as particles less than 10 microns in diameter that are capable of remaining airborne for extended periods. According to the CDC, “There is no clear evidence that powered dental and surgical instruments can generate aerosols containing infective bloodborne pathogens.” As long as dental professionals follow recommended infection prevention protocols to prevent pathogenic exposure, there are no safety concerns regarding the use of handpieces and ultrasonic scalers, and these devices should be used when indicated. HIV is a bloodborne, not an airborne, disease.
In general, the provision of oral health care services for patients with HIV/AIDS is not unlike those who are HIV negative. The delivery of care should remain the same unless there is another medical complication, such as uncontrolled diabetes, that affects treatment.
TESTING FOR HIV
Many individuals are unaware of their HIV status, providing the opportunity for the oral health care team to offer HIV screening. Several studies have revealed positive patient attitudes when asked if they would be willing to be screened for HIV infection in the dental setting.12–14 Research has demonstrated that when individuals are aware of their HIV-positive status, they are less likely to engage in behaviors that place themselves or others at risk.15 Also, early entry into care and treatment leads to better health outcomes. Oral health professionals may be among the first to notice signs and symptoms of HIV infection. This provides the opportunity to discuss the possibility of HIV exposure, HIV testing history, and whether the patient would consent to rapid testing for HIV.12–14
Since the advent of rapid HIV screening, many dental education facilities and public and private dental programs have initiated screening as a component of routine care. Testing for HIV has evolved since the first models were developed in the mid-1980s, when it was used to detect HIV antibodies and, if positive, results were confirmed with a Western blot test. These tests detected HIV, but could not determine when the infection occurred or for how long it had been present. The newest generation of screening can detect HIV sooner after infection than previous tests.16 In 2006, the CDC updated its recommendations for HIV testing, indicating that all individuals age 13 to 65 should be tested at least once.12 In 2014, the CDC released updated recommendations for labs in it publication, “Laboratory Testing for the Diagnosis of HIV Infection, Updated Recommendations.”
In a 2014 presentation by Howard Libman, MD, a professor of medicine at Harvard Medical School and director of the HIV Program in Healthcare Associates at Beth Israel Deaconess Medical Center in Boston, he emphasized that HIV has become a chronic, multisystem disease with a wide spectrum of manifestations. Approximately 30% of new cases are present in individuals age 50 or older, and the comorbidities at age 50 are similar to those experienced by someone 10 years older. Also, older patients are often tested and diagnosed late and have more advanced disease at diagnosis.17 It is estimated that, in 2015, half of all new HIV cases will be diagnosed in individuals age 50 or older.
CONCLUSION
The oral health care team is well positioned to be integrated into primary care practice. Oral health professionals can be a vital component in the recognition of and testing for medical conditions, such as HIV, in the dental setting. The federal Health Resources and Service Administration is focusing on this integration and has developed recommendations and resources to assist in this effort. There have been webinars and curricula established for primary care to integrate oral health care into their practices. Concurrently, oral health professionals can assist primary care through the recommendations proposed in this article.
Oral health professionals are challenged to consider the means by which dental practices can evolve into primary health care settings and offer the most integrated and comprehensive care available to patients.
References
- U.S. Centers for Disease Control and Prevention. Vital Signs: HIV Diagnosis, Care, and Treatment Among Persons Living with HIV — United States, 2011. Available at: http://www.cdc.gov/ mmwr/ preview/mmwrhtml/mm6347a5.htm. Accessed October 29, 2015.
- Reznik D, Bednarsh H. HIV and the dental team. Dimensions of Dental Hygiene. 2006;4(6):14–16.
- Cohen MS, McCauley M, Gamble TR. HIV treatment as prevention and HPTN 052. Curr Opin HIV AIDS. 2012,7:99– 105.
- U.S. Centers for Disease Control and Prevention. CDC Fact Sheet: HIV in the United States: The Stages of Care. Available at: cdc.gov/hiv/ pdf/ research_ mmp_stagesofcare.pdf. Accessed October 29, 2015.
- U.S. Centers for Disease Control and Prevention. National HIV Prevention Progress Report. Available at: http://www.cdc.gov/hiv/pdf/policies_Nati onalProgressReport_brief.pdf. Accessed October 29, 2015.
- U.S. Department of Health and Human Services. National HIV/AIDS Strategy Vision. Available at: https://www.aids.gov/federalresources/ national-hiv-aidsstrategy/ overview/. Accessed October 29, 2015.
- Monto A, Schooley RT, Lai JC, et al. Lessons from HIV therapy applied to viral hepatitis therapy: summary of a workshop. Am J Gastroenterol. 2010;105:989–1004.
- Haden NK, Catalanotto FA, Alexander CJ, et al. Improving the oral health status of all Americans: roles and responsibilities of academic dental institutions: the report of the ADEA President’s Commission. J Dent Educ. 2003;67:563–583.
- U.S. Department of Health and Human Services. National HIV/AIDS Strategy Implementation Progress Report 2011. Available at: aids.gov/pdf/2011- nhas-progress-report.pdf. Accessed October 29, 2015.
- Glick M, Abel SN, Muzyka BC, DeLorenzo M. Dental complications after treating patients with AIDS. J Am Dent Assoc. 1994;125:296–301.
- Jeske AH, Suchko GD; American Dental Association Council on Scientific Affairs and Division of Science; Journal of the American Dental Association. Lack of a scientific basis for routine discontinuation of oral anticoagulation therapy before dental treatment. J Am Dent Assoc. 2003;134:1492–1497.
- Deitz CA, Ablah E, Reznik D, et al. Patients’ attitudes about rapid oral HIV screening in an urban, free dental clinic. AIDS Patient Care STDs. 2008;22:205– 212.
- VanDevanter A, Combellick J, Hutchinson MK, Phelan J, Malamud D, Shelley D. A qualitative study of patients’ attitudes toward HIV testing in the dental setting. Nurs Res Pract. 2012;2012: 803169.
- Greenberg BL, Kantor ML, Jiang SS, Glick M. Patients’ attitudes toward screening for medical conditions in a dental setting. J Public Health Dent. 2012;72:28–35.
- Crepaz N1, Marks G. Serostatus disclosure, sexual communication and safer sex in HIV-positive men. AIDS Care. 2003;15:379–387.
- Branson BM, Handsfield HH, Lampe MA, et al. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recomm Rep. 2006;55:1–17.
- Cohen C. Overview of Current Issues in HIV and Aging. Presented at: 10th Annual National Conference on HIV/AIDS & Aging; September 26, 2014; Boston.


[…] Read more about managing dental patients with HIV at: https://decisionsindentistry.com/article/managing-dental-patients-with-hiv/ […]