
 PHOTO BY JONATHAN BORBA ON UNSPLASH
PHOTO BY JONATHAN BORBA ON UNSPLASH
Maintaining Palatal Comfort Following Gingival Grafting
Using a palatal stent and collagen wound dressing can help clinicians manage complications and postoperative pain from gingival grafting procedures.
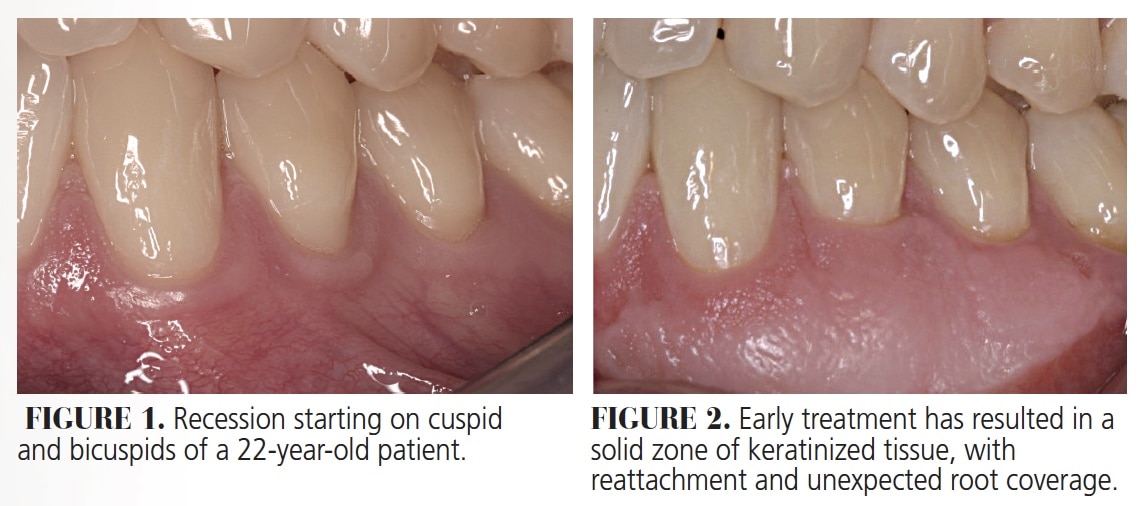
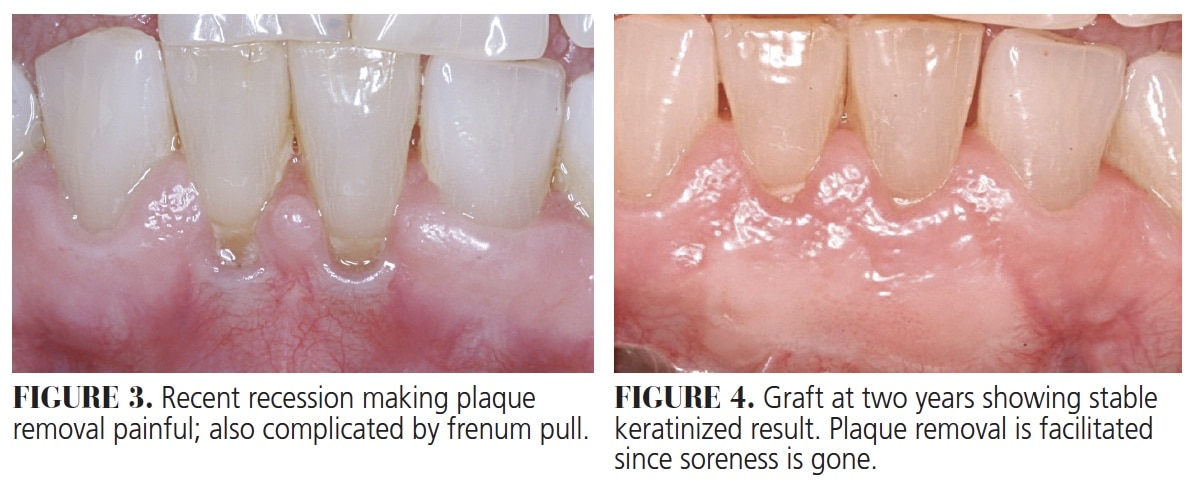
Gingival grafts have been used for decades to stop recession (Figure 1 and Figure 2), augment tissue to prevent recession around restorations1 (notably around recently placed restorations), and to facilitate brushing when the tissues are thin, sore and receding (Figure 3 and Figure 4). Originally reported by Sullivan and Atkins2 in 1968, these grafts remain effective and poplar today, but can be associated with postoperative pain and complications from an open palatal wound if not managed carefully.
At times, patients push back against a recommendation to undergo gingival grafting from the palate. Patients report having heard worrisome stories about painful experiences and difficulty eating due to discomfort from the palatal donor site. Complications have also been long reported, and should not be dismissed.3 The good news is that palatal discomfort no longer needs to be a reality. Clinicians can, with confidence, reassure patients that a comfortable experience is possible by using the straightforward approach described in this paper.
This technique has been reported by others and shows the benefits of using a palatal stent, plus a collagen wound dressing, to manage postoperative pain and complications following gingival grafting.4 Otherwise, reports have indicated that grafting can result in bleeding, pain and possibly slower-than-hoped-for healing.5 Consequently, when patients express objections and fear, some dentists are hesitant in recommending these procedures. When grafting is clinically indicated, the use of a palatal stent and collagen dressing will minimize the possibility of a periodontal dressing falling off the palate, exposing the wound and leaving patients unhappy.
Researchers at Gazi University in Turkey investigated several methods for managing palatal comfort,5 including use of an Essix retainer, collagen fleece and low-level laser therapy. The collagen (as used in their study) was held in place with sutures. Each approach was hypothesized to improve comfort and healing.
SUCCESSFUL STRATEGY
Another report of managing very large donor sites also involved palatal stents. The subjects in this study reported some discomfort, at times significant, but it was controlled with analgesic medication and the management strategy was deemed successful overall.6 The same authors followed with another report, this time using collagen dressing alone, also held in place by sutures. Analgesic medications helped the patients in this report, as well.7 The authors’ comments on the collagen membranes conceded that while its use increases cost, the expense may be justified to improve outcomes with large grafts from the palate.
There is evidence that using a layer of collagen at the donor site will enhance and speed the healing process. As reported by Shanmugam et al,8 the use of the collagen, held in place this time by an acrylic stent, improved patient comfort and allowed faster healing compared to simply covering the site with a periodontal dressing. The team also commented that histologic study showed the collagen-enhanced sites demonstrated more collagen formation in the healed site than in the dressing-only group.
The technique of combining a palatal covering with a collagen layer offers several benefits to the provider and patient. It virtually eliminates the chance for irritation from the tongue or other events during sleep that can result in a bleeding episode and an emergency call. It also increases comfort at mealtime since no food or tongue activity rubs on an open wound. In addition, patients have confidence the wound is protected as they go about their daily routines.4–8
CONNECTIVE TISSUE GRAFTS
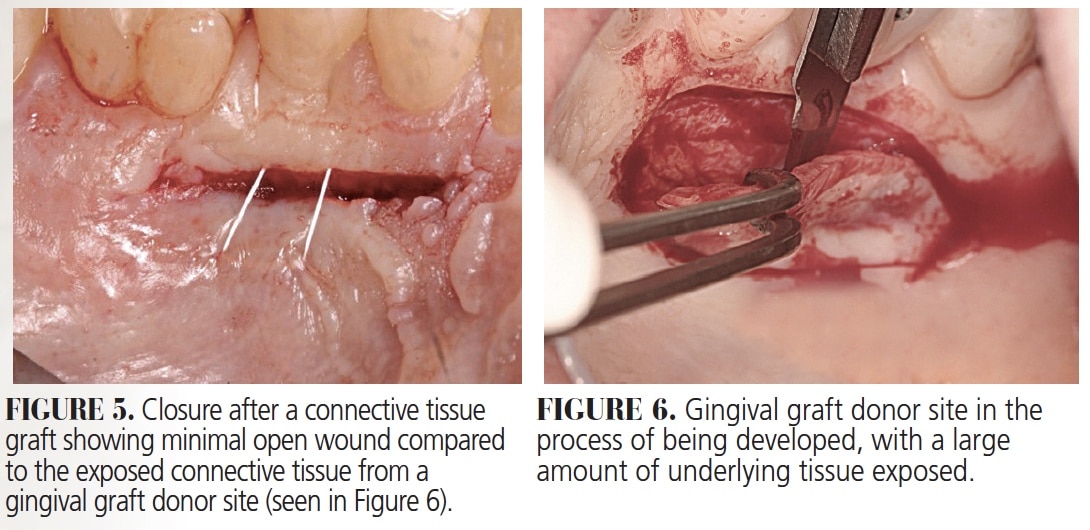
Another popular graft from the palate, the connective tissue graft (CTG), does not need this protection, as it is not typically associated with as much morbidity. This is because the donor tissue is taken from inside the palate in a trapdoor fashion, resulting in near primary closure of the palatal wound (Figure 5). As a result, patient comfort is much better (even with no palatal covering) compared to the large amount of exposed raw tissue from a gingival graft donor site (Figure 6). The CTG procedure is useful when root coverage is the goal. However, this is not the case with gingival grafts, which are considered successful if some root remains exposed (Figure 4) — even if full root coverage does sometimes occur (as seen in Figure 2).
In addition to patients pushing back, some clinicians question whether the more painful gingival graft procedure is outdated and should routinely be replaced with CTGs. Both types have their place. Gingival grafts are cited in the proceedings from the American Academy of Periodontology (AAP) regeneration workshop as the gold standard for tissue augmentation.9 Indications include stopping recession in nonesthetic areas, preventing recession around restorations when placed in areas of thin tissue (especially with intracrevicular margins),1,9 facilitating plaque control, as well as use during orthodontic movement in areas of thin biotype.9 On the other hand, CTGs (as noted) are the primary choice when root coverage is needed or desired.10
The same principles apply to dental implants, as it is the bone and stable tissue that are protected by a zone of keratinized tissue.
The AAP workshop publication offers a comprehensive literature review of both grafts that is not repeated in this article. Rather, this paper focuses on the management of palatal discomfort and healing. With the technique discussed here, the painful palate scenario is all but eliminated — and that is the main point.
HIGHLY PREDICTABLE OUTCOMES
In this age of advanced technology and high patient expectations, it can be useful for clinicians to support the benefits of gingival grafts, and express confidence the procedure can be both beneficial and comfortable. This will help alleviate patient concerns, because a gingival graft is one of the most predictable surgical procedures in periodontics.11
Providers who embrace this technique in gingival grafting can deliver more complete care, and patients can start telling positive stories instead of negative ones. By making a palatal stent out of a thin plastic vacuform material and covering the wound under the plastic with collagen, clinicians and patients can enjoy predictable, evidence-based results in both comfort and healing. The technique is as follows:
- Assure patients of the benefits (namely, increased comfort and diminished chance of postoperative bleeding) derived from the palatal stent.
- Take a maxillary impression at the consultation appointment and pour a model.
- Make a vacuform stent with 0.20-mm material prior to the surgical appointment.
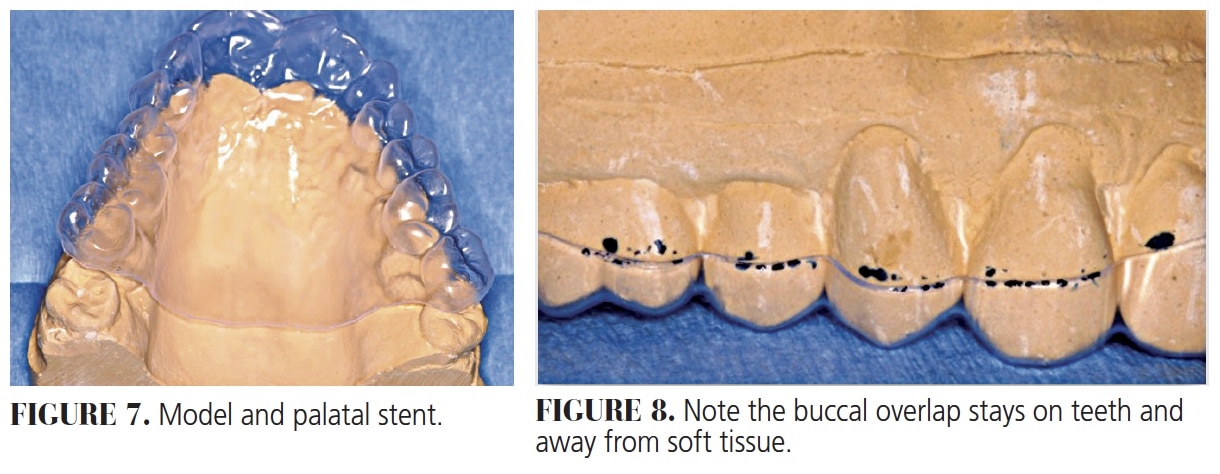
- Trim the plastic to avoid the soft palate, as with a denture, and trim to overlap on the buccal surfaces of teeth only 2 to 3 mm to stay off the soft tissues (Figure 7 and Figure 8). Trimming to avoid the soft palate will ensure the gag reflex will not come into play.
- At the surgical appointment, check the fit before starting the procedure to ensure the trimming was accurate.
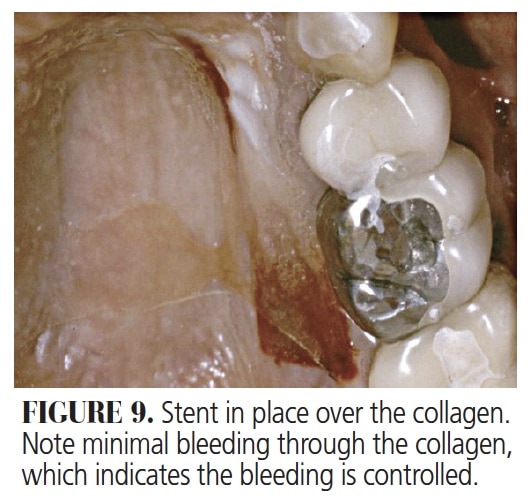
- After surgery, place two layers of the collagen material of choice over the donor site, and cover it with the stent. Make certain the stent contacts and gently holds the collagen in place (Figure 9).
Besides significantly less pain, a major benefit is that collagen will result in almost immediate clotting. Consequently, since the stent holds the collagen against the donor site, bleeding is visibly under control before the patient leaves the office. In addition, with the knowledge the collagen will remain in place overnight, clinicians can be confident they have eliminated one serious potential complication of a graft from the palate — namely, postoperative bleeding from the donor site.
 Postoperative instructions for the patient (which should always be given in writing) are:
Postoperative instructions for the patient (which should always be given in writing) are:
- Leave the stent in until the next morning.
- At that time, remove it and resume brushing and flossing as normal, but avoid the graft sites (both donor and recipient). Let the patient know it is OK if the collagen falls out.
- Leave the stent in full time for the first week, removing it only for brushing and flossing.
- After the first week, use the stent while eating and sleeping until feeling comfortable without it.
- At this point, the stent is only used for palatal comfort (if and when needed). It will not affect the outcome if used less frequently.
- If a second graft is planned, ask the patient to save the stent.
CONCLUSION
Discussing grafting techniques to help patients understand the benefits will result in greater acceptance, and higher levels of patient comfort, compliance and satisfaction. In turn, clinicians can improve patients’ periodontal health and achieve better restorative results by predictably preventing recession in areas where the gingiva may be thin.
A careful and thoughtful explanation of the approach described here should help overcome possible patient objections to gingival grafting. This method might also enhance relationships between general dentists and periodontists by sharing this technique tip if they are not already using it.
Key Takeaways
- Gingival grafts are used to stop recession and augment tissue to prevent recession around restorations,1 and to facilitate brushing when the tissue is thin, sore and receding.
- If not managed carefully, gingival grafts can be associated with complications and postoperative pain from the open palatal wound.
- The surgical approach described in this report uses a palatal stent and collagen wound dressing to improve patient comfort and minimize postsurgical complications.
- Although the use of collagen membranes increases treatment costs slightly, the expense may be justified to improve outcomes when harvesting grafts from the palate.
- Shanmugam et al8 reported the use of collagen, held in place by an acrylic stent, allowed faster healing compared to simply covering the site with a periodontal dressing.
- In addition, histologic study showed the collagen-enhanced sites demonstrated more collagen formation in the healed site than in the dressing-only study group.8
- This technique virtually eliminates the chance for irritation from the tongue or other events during sleep that can result in a bleeding episode and an emergency call from the patient.
- Discussing grafting techniques to help patients understand the benefits will result in greater acceptance and higher levels of patient comfort, compliance and satisfaction.
References
- Wennstrom J. Mucogingival therapy. Ann Periodontol. 1996;1:671–701.
- Sullivan HC, Atkins JH. Free autogenous gingival grafts. Principles of grafting. Periodontics. 1968;6:121–129.
- Brasher WJ, Rees TD, Boyce WA. Complications of free grafts of masticatory mucosa. J Periodontol. 1975;46:133–138.
- Nettem S, Nettemu SK, Singh VP, Nayak SU. Free gingival graft: an effective technique to create healthy keratinised gingiva. Indian J Menodent Allied Sci. 2018;6:30–34.
- Evaluation of the Effectiveness of Different Methods for Healing a Palatal Donor Site After Harvesting a Free Gingival Graft. Available at: https://clinicaltrials.gov/ ct2/show/NCT03567148. Accessed October 14, 2020.
- Berridge JP, Johnson TM, Lane JD, Miller PD. Focus on epithelialized palatal grafts. Part 1: Multiple adjacent recession defects in the mandibular anterior. Clin Adv Periodontics. 2018;8:160–166.
- Berridge JP, Johnson TM, Lane JD, Miller PD. Focus on epithelialized palatal grafts. Part 3: Methods to enhance patient comfort at palatal donor sites. Clin Adv Periodontics. 2019;9:177–184.
- Shanmugam M, Kumar TS, Arun KV, Arun R, Karthik SJ. Clinical and histological evaluation of two dressing materials in the healing of palatal wounds. J Indian Soc Periodontol. 2010;14:241–244.
- Kim DM, Neiva R. Periodontal soft tissue non-root coverage procedures: a systematic review from the AAP Regeneration Workshop. J Periodontol. 2015;86(Suppl 2):S56–S72.
- Chambrone L, Tatakis D. Periodontal soft tissue root coverage procedures: a systematic review from the AAP Regeneration Workshop. J Periodontol. 2015;86(Suppl 2):S8–S51.
- Hagorsky U, Bissada N. Clinical assessment of free gingiva graft effectiveness on the maintenance of periodontal health. J Periodontol. 1980;51:274–278.
From Decisions in Dentistry. November 2020;6(10): 10-12.
