
 PROSTHESIS IMAGE COURTESY OF GLIDEWELL
PROSTHESIS IMAGE COURTESY OF GLIDEWELL
Immediate Implant Placement With Virtual Planning in the Esthetic Zone
Addressing the buccal gap dimension and applying the principles of the 10 keys will help ensure optimal esthetic outcomes with anterior implants.
Consumers now demand and expect same-day or next-day delivery of goods and services, and this is also true for patients seeking dental treatment. Fueled by extensive marketing, the rising popularity of immediate tooth replacement has led some clinicians to feel pressured into providing immediate implant placement and temporization. Simultaneously, patients expect near-perfect esthetic outcomes, with the final restoration appearing indistinguishable from the surrounding teeth. Without adequate patient selection, treatment planning, and setting realistic patient expectations, immediate implant placement and restoration can easily lead to esthetic and biological failures,1 along with patient disappointment, frustration or aggravation.

In 2017, Levine et al2 introduced the “10 keys,” an evidence-based treatment algorithm for successful and predictable placement of immediate implants in the esthetic zone. The updated 10 keys address the major pre-, peri- and postoperative aspects of immediate implant placement and temporization that promote optimal long-term esthetic and functional success. The 10 keys for successful esthetic-zone single immediate implants are as follows:
- Esthetic risk assessment
- Preoperative cone beam computed tomography (CBCT) assessment, with virtual surgical and restorative-driven treatment planning. Additionally, an appropriately sized and positioned implant is chosen to allow for a buccal gap > 2 mm
- Minimally traumatic tooth extraction, without flap reflection (if possible), with evaluation of the buccal and palatal plate status post-extraction (if there is any buccal height loss, other treatment options should be considered)
- Three dimensional implant placement in good available bone, positioned along the palatal wall with an anticipated buccal gap > 2 mm
- Use of a narrower, 3.3- to 4.3-mm-diameter implant allowing for a > 2-mm-wide buccal gap and good primary stability
- Bone grafting of the buccal gap with a low-substitution-rate bone material
- Buccal soft tissue grafting using a subepithelial connective tissue graft (CTG) or a volume-stable collagen matrix
- Immediate contour management of the soft tissue emergence profile using a customized healing abutment or temporary crown
- Use of a custom impression coping technique to duplicate the created transition zone
- Final restoration with a screw-retained crown (when possible)

To achieve optimal esthetic outcomes, all 10 keys must be followed in sequential order, and if one of the surgical keys is unable to be completed, immediate implant placement may be aborted. Otherwise, the long-term hard and soft tissue stability or esthetic outcome may be compromised to certain degree. The following case report describes the utilization of the 10 keys in the planning and execution of an immediate implant in the anterior esthetic zone. It aims to highlight the importance of following all 10 keys to optimize esthetics; also included are suggestions as to how the authors would treat this case today.
CASE REPORT
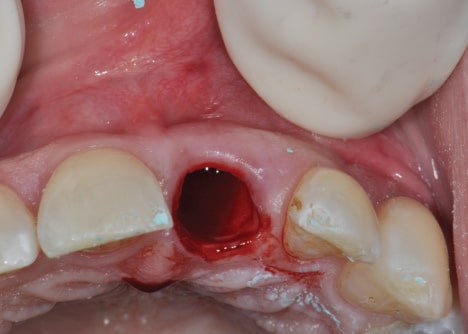
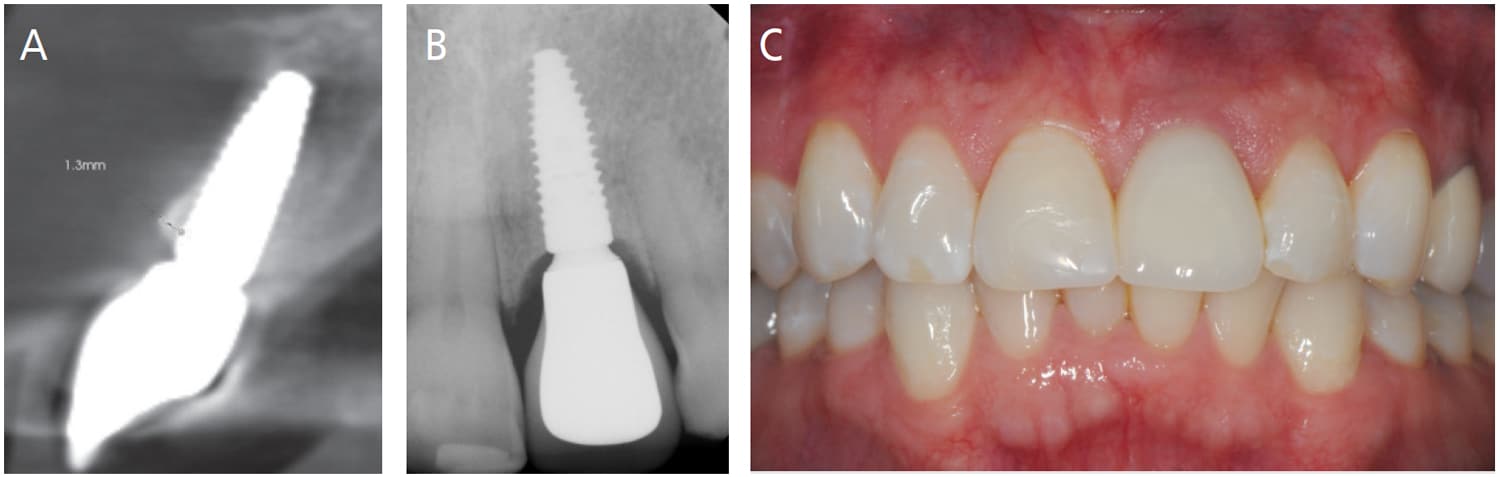
A 37-year-old healthy, nonsmoker male patient was referred by his prosthodontist to a periodontist following loss of the post-core-crown restoration on tooth #9 (Figures 1A and 1B). The patient reported seasonal allergies and acid reflux, and was taking esomeprazole (ASA II). Intraoral examination showed minor gingival inflammation of tooth #9; however, clinical probing depths were normal (≤ 3 mm). The mid-buccal fracture was near the osseous crest. No periodontal disease or caries were evident, and no parafunctional habits or tooth mobility were noted.
Several treatment options — including their advantages and disadvantages — were presented and discussed with the patient. As the adjacent teeth were unrestored, the patient elected to pursue dental implant replacement of tooth #9.
A preoperative esthetic risk assessment3 (Table 1) was completed (Key No. 1), and identified a thin buccal wall phenotype. Due to the low lip line and realistic expectations, the patient was classified as a medium esthetic risk. As the patient was being managed by an experienced multidisciplinary team, it was decided in consultation with the patient that an immediate implant and provisional crown could be delivered with optimal esthetic results — provided the additional nine keys were applied.
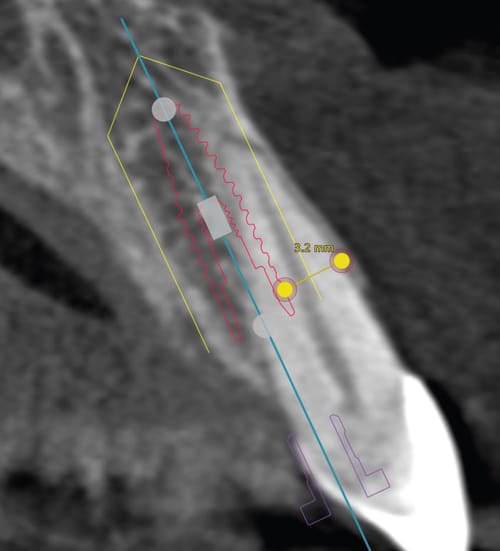
A CBCT image of the maxilla showed an intact, but thin, buccal plate on tooth #9 (Key No. 2). Apical and lingual bone were available to provide primary stability. Implant placement was planned digitally (Figure 2). A 4.1×12 mm bone-level tapered implant was planned in a palatal position, allowing a gap between the implant and buccal plate, and the implant shoulder was positioned 1 mm apical to the height of the buccal plate, ensuring adequate “running room” to create an ideal emergence profile4 in a screw-retained position.
Following appropriate anesthesia, the tooth was extracted with a flapless approach (Key No. 3; Figure 3). The socket was thoroughly curetted and irrigated to remove all soft tissue remnants. The buccal plate was confirmed intact, albeit thin. It is important to note that if the buccal plate was damaged, the risk for future esthetic complications significantly increases, and, as such, immediate implant placement would have been aborted. The decision would be either a ridge preservation procedure followed by late implant placement, or early implant placement at two months post-extraction to reduce the chance of an esthetic complication.
With the aid of an anatomically correct surgical guide, a regular-diameter implant (4.1 mm) was placed in a palatal position (Key nos. 4 and 5) and 1 mm below the height of the buccal plate. Excellent insertion torque (> 35 Newton centimeters) was achieved.

A full-thickness tunnel was created on the buccal aspect, and a CTG from the palate was inserted and stabilized with a resorbable suture to augment the soft tissue thickness (Key No. 7; Figure 4A). While it is important to follow the 10 keys in sequential order, Key nos. 6 and 7 are the exception, as once the buccal wall is preserved, the execution order of these two steps is up to the treating clinician. In this case, CTG was done prior to grafting for ease of surgical access and to ensure that graft particles were not included in the soft tissue space. The space between the buccal plate and implant was then grafted (Key No. 6) with a 50/50 mix of surgical-grade calcium sulphate and a mineralized allograft (Figure 4B).
An impression was made, and a tall healing abutment (5.5 mm width x 6.0 mm height) was placed. A lab-processed, screw-retained acrylic resin provisional restoration was fabricated by the prosthodontist and delivered the day after surgery (Key No. 8). Attention was given to the critical and subcritical contours, providing support to the healing soft tissue4 (Figures 5A through 5C). All occlusal contacts were removed in maximum intercuspation and excursive movements. After a three-month healing period, minor adjustments to the contours of the provisional restoration were made to appropriately mimic the adjacent tooth and its soft tissues facially and interproximally.

Due to patient factors, the temporary prosthesis was left in function for two years. Then, a final impression was completed utilizing the custom impression coping technique to allow for the duplication of the developed emergence contour in the final restoration (Key No. 9; Figure 6). A final screw-retained restoration was provided and inserted (Key No. 10).
Follow-up at five years (Figures 7A through 7C) demonstrates adequate pink and white esthetics; however, a slight grey hue was present in the midfacial gingival tissues. A CBCT scan demonstrated maintenance of the buccal bone in the coronal portion; however, remodeling was evident in the mid apical region that did not impact the esthetics and health of the implant.

DISCUSSION
What are the takeaways from this case? The purpose of the 10 keys is to provide a structured and evidence-based approach to immediate implant treatment, maximizing the long-term esthetic outcome.2,5,6 It is important to realize that all 10 keys should be sequentially followed; otherwise, a compromised outcome may occur. The following discussion outlines where improvements could be made based on current publications that our group is completing.
Use of the esthetic risk assessment tool is important in categorizing and assessing possible preoperative factors affecting long-term outcomes that may need to be addressed in the treatment planning phase. This assessment is also a valuable tool in educating the patient about the complexity of his or her personal anatomical situation, while helping to align the patient and practitioner’s final esthetic expectations prior to initiating treatment.
In this patient, it was important to identify the moderately thin and scalloped gingival phenotype. A thinner gingival phenotype is correlated with a thin buccal plate (< 1 mm),7 which was subsequently confirmed with CBCT analysis. This thin buccal plate can be problematic, as following tooth extraction, pronounced buccal bone and soft tissue loss occurs,8,9 amounting to bone loss of up to 7 mm in the vertical dimension at the mid buccal aspect,9 along with up to 50% of the ridge width.10 Placing an immediate implant, per se, does not prevent this bone loss from occurring.11,12 Ridge preservation by means of socket grafting, in conjunction with immediate implant placement, can counteract some of the effects.13 If not identified prior to surgery and adjusting the surgical plan accordingly (Key nos. 6 and 7), this could lead to major esthetic and long-term maintenance problems.
Assessment via CBCT scans and preoperative virtual planning allows for an appropriately sized and positioned implant to be chosen (Key No. 2), thus ensuring a > 2 mm buccal gap, adequate primary stability, and placement in the ideal position for a screw-retained restoration. It can also allow the practitioner to visualize the thickness of the buccal plate, and the need for any adjunctive soft and hard tissue grafting procedures to counteract the anticipated bone and soft tissue loss.
Key No. 5 states that a narrower-diameter implant should be used to allow for a > 2 mm gap between the implant and internal surface of the buccal plate. However, as shown on the preoperative CBCT scan (Figure 2), the implant size chosen (4.1×12 mm) was not ideal, allowing for only a 1.8 mm buccal gap at the implant shoulder. Ideally, a 3.3×12 mm implant should have been planned and placed instead (Figure 8). Selecting an implant size that allows for a > 2 mm grafted gap promotes buccal plate stability and counteracts the ridge reduction following extraction.12,14–16 A larger-diameter implant can obturate the socket, restricting the space to place the bone substitute and compromising the long-term viability of the buccal bone.14,15 Following resorption of the buccal plate, exposure of the implant may occur, leading to esthetic and possible long-term biologic challenges.
Levine et al17 (in preparation) evaluated the effect of the buccal gap dimension on the newly formed buccal bone following immediate implant placement in maxillary central incisors. All sites were treated with immediate implant placement and ridge preservation by means of socket grafting, using a xenograft. Assessment via CBCT 5±4 years following implant placement indicated that when the grafting gap dimension was > 2 mm, the thickness of the buccal bone was 1.9 mm; however, when it was ≤ 2 mm, it was significantly reduced to 0.5 mm. This could predispose to esthetic and biological complications in the future. Thus, this study concluded that, ideally, a > 2 mm wide buccal gap should be virtually planned and grafted to allow adequate buccal bone formation, promoting stability for the future.
While use of a CTG may compensate for soft tissue collapse in the most coronal portion of the gingival complex, it does not prevent loss of the buccal bone; consequently, combining a CTG with a bone graft is suggested.18 A recent systematic review by Seyssens et al19 indicated that although evidence in the literature was moderate, simultaneous placement of a CTG at the time of immediate implant placement contributes to the stability of the midfacial mucosa and should be considered in sites with a thin gingival biotype and a buccal bone thickness < 0.5 mm. Additionally, thickening of the mucosal tissue to 3 mm or greater is advantageous in masking the color of restorative materials utilized in the implant restoration, preventing graying of the tissue and improving esthetics.20
Levine et al21 (2021, accepted) evaluated the effect of a CTG following immediate implant placement and ridge preservation at maxillary central incisor sites. They found that although changes in mid buccal mucosal tissue height and buccal bone thickness over the implants did not vary if a CTG was completed or not, sites treated with a CTG exhibited significantly higher esthetic outcomes. In the current case, a CTG was performed in the coronal aspect, and although some graying of the mucosa was present, the graft positively impacted postoperative healing and esthetics. If the slight graying of the tissue was an esthetic concern for the patient, a second CTG could be placed to further thicken the tissue in the region of the thinner apical bone.
The buccal bone graft material aims to provide space maintenance and wound stability, allowing for bone growth rather than soft tissue. Using a low-substitution-rate graft material reduces the possibility of graft remodeling and resorption, increasing the probability of retaining the original ridge volume, and promoting greater bone stability.15 When used in combination with a CTG, the patient’s phenotype is shifted from thin to thick,5,22 promoting a more esthetic outcome. In this case, a 50/50 mix of calcium sulphate and a mineralized allograft was used. Calcium sulphate is considered to be a fast-resorbing material and can resorb in one to three months.23 This combination of graft materials, together with the small buccal grafting gap, could have led to less retention of buccal bone and graying of the mucosa. Today, a low substitution graft material (such as a xenograft) would be used to aid in reducing bone loss on the buccal aspect.13
CONCLUSION
Meticulous and systematic planning and clinical execution through use of the updated 10 keys can lead to favorable functional and esthetic results. While this case achieved acceptable esthetics for the patient, as outlined, it is important to closely follow all keys to ensure an optimal esthetic outcome.
References
- Tonetti MS, Cortellini P, Graziani F, et al. Immediate versus delayed implant placement after anterior single tooth extraction: the timing randomized controlled clinical trial. J Clin Periodontol. 2017;44:215–224.
- Levine RA, Ganeles J, Gonzaga L, et al. 10 Keys for successful esthetic-zone single immediate implants. Compend Contin Educ Dent. 2017;38:248–260.
- Chappuis V, Martin W. Implant Therapy in the Esthetic Zone — Current Treatment Modalities and Materials for Single-tooth Replacements. Vol 10. Batavia, Ill: Quintessence Publishing; 2017.
- Gonzalez-Martin O, Lee E, Weisgold A, Veltri M, Su H. Contour management of implant restorations for optimal emergence profiles: Guidelines for immediate and delayed provisional restorations. Int J Periodontics Restorative Dent. 2020;40:61–70.
- Levine RA, Ganeles J, Kan J, Fava PL. 10 keys for successful esthetic-zone single implants: importance of biotype conversion for lasting success. Compend Contin Educ Dent. 2018;39:522–530.
- Levine RA, Ganeles J, Wang P, et al. Application of the 10 keys for replacement of multiple teeth in the esthetic zone. Compend Contin Educ Dent. 2021;42:F1–F11.
- Cook D, Mealey B, Verrett R, et al. Relationship between clinical periodontal biotype and labial plate thickness: an in vivo study. Int J Periodontics Restorative Dent. 2011;31:345–354.
- Chen ST, Darby IB, Reynolds EC, Clement JG. Immediate implant placement postextraction without flap elevation. J Periodontol. 2009;80:163–172.
- Chappuis V, Engel O, Reyes M, Shahim K, Nolte LP, Buser D. Ridge alterations post-extraction in the esthetic zone: a 3D analysis with CBCT. J Dent Res. 2013;92(Suppl 12):195S–201S.
- Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 2003;23:313–323.
- Araujo MG, Sukekava F, Wennstrom JL, Lindhe J. Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog. J Clin Periodontol. 2005;32:645–652.
- Covani U, Cornelini R, Calvo-Guirado JL, Tonelli P, Barone A. Bone remodeling around implants placed in fresh extraction sockets. Int J Periodontics Restorative Dent. 2010;30:601–607.
- Zaki J, Yusuf N, El-Khadem A, Scholten R, Jenniskens K. Efficacy of bone-substitute materials use in immediate dental implant placement: A systematic review and meta-analysis. Clin Implant Dent Relat Res. 2021;23:506–519.
- Araujo MG, Sukekava F, Wennstrom JL, Lindhe J. Tissue modeling following implant placement in fresh extraction sockets. Clin Oral Implants Res. 2006;17:615–624.
- Rosa AC, da Rosa JC, Dias Pereira LA, Francischone CE, Sotto-Maior BS. Guidelines for selecting the implant diameter during immediate implant placement of a fresh extraction socket: a case series. Int J Periodontics Restorative Dent. 2016;36:401–407.
- Spray JR, Black CG, Morris HF, Ochi S. The influence of bone thickness on facial marginal bone response: stage 1 placement through stage 2 uncovering. Ann Periodontol. 2000;5:119–128.
- Levine RA, Dias DR, Wang P, Araujo MG. Effect of buccal gap dimension following immediate implant placement on the buccal bone wall: a retrospective CBCT analysis. In preparation. 2021.
- Jiang X, Di P, Ren S, Zhang Y, Lin Y. Hard and soft tissue alterations during the healing stage of immediate implant placement and provisionalization with or without connective tissue graft: A randomized clinical trial. J Clin Periodontol. 2020;47:1006–1015.
- Seyssens L, De Lat L, Cosyn J. Immediate implant placement with or without connective tissue graft: A systematic review and meta-analysis. J Clin Periodontol. 2021;48:284–301.
- Jung RE, Sailer I, Hammerle CH, Attin T, Schmidlin P. In vitro color changes of soft tissues caused by restorative materials. Int J Periodontics Restorative Dent. 2007;27:251–257.
- Levine RA, Dias DR, Wang P, Araujo MG. Effect of connective tissue graft following immediate implant placement on esthetic outcomes at maxillary central incisor sites: a long-term cohort study. Int J Periodontics Restorative Dent. Accepted for publication. 2021.
- Cabello G, Rioboo M, Fabrega JG. Immediate placement and restoration of implants in the aesthetic zone with a trimodal approach: soft tissue alterations and its relation to gingival biotype. Clin Oral Implants Res. 2013;24:1094–1100.
- Fernandez de Grado G, Keller L, Idoux-Gillet Y, et al. Bone substitutes: a review of their characteristics, clinical use, and perspectives for large bone defects management. J Tissue Eng. 2018;9:2041731418776819.
From Decisions in Dentistry. January 2022;8(1):9-12.
