

Guest Editorial: Isolation in Endodontics
Despite the many advantages of dental dams, they are often underutilized in endodontic and restorative procedures.
Despite the many advantages of dental dams, they are often underutilized in endodontic and restorative procedures
In a paper published in the Journal of the American Dental Association, the authors note that only 44% of respondents reported using dental dams all of the time during root canal treatment.1 Another article cited only 60% usage among general practitioners surveyed.2 These numbers may not surprise endodontists or educators who have been treating patients and teaching endodontics for years. In fact, a 1967 publication indicated that merely 7% of respondents used dental dams for endodontic treatment.3

COURTESY AUSTRALIAN ENDODONTIC JOURNAL
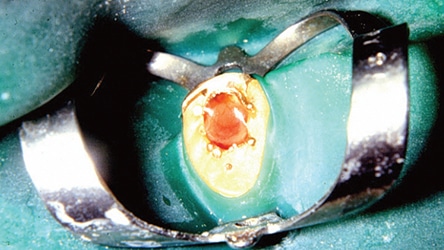
While there are any number of rationalizations for not using a dental dam for patient care, much less endodontic treatment,4 what some clinicians fail to consider are the innumerable benefits — and not just for endodontic therapy, but also for restorative treatment. These include protection from aspiration and swallowing of instruments5 (Figure 1), burs, solutions, restorative materials, debris and particulates. Besides providing isolation and moisture control (thus reducing airborne pathogens), dams improve access to and visualization of the treatment site. They also aid tongue and cheek management while improving patient comfort and enhancing clinical efficiency.
Initially made available to dentistry, royalty free, by Sanford C. Barnum, DDS, in 1862, today’s dental dams are listed by the U.S. Food and Drug Administration as Class 1 medical devices.6 The use of dams for endodontic treatment is defined as the standard of care by the American Association of Endodontists.7 Even so, marginal use of dental dams remains a concern in dental practice — even though every dental school in the United States teaches use of the dental dam.
DENTAL DAMS IN PERSPECTIVE
Too often in the teaching clinic, dental dam placement seems to take on the burden of a comprehensive treatment plan, and unnecessary time is spent to achieve a perfection that is not needed. Voltaire popularized the aphorism “Perfect is the enemy of good” in 1770. This was hardly unique, as the concept was also espoused by others, including Aristotle and Confucius.8
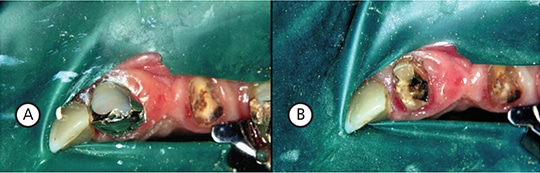
My approach to using dental dams came as a general practitioner as I was developing an interest in endodontics. Having spent a day in the office of an endodontist who would later become my graduate mentor, I saw that, contrary to most textbook recommendations, he would routinely isolate more than one tooth (Figures 2A through 2D). I emulated his technique and was soon routinely applying dams for restorative procedures, including crown and abutment preps — and, of course, endodontic therapy. With increased frequency came increased proficiency and efficiency.

FIGURE 2C COURTESY IVAN NEDELTCHEV, DDS; FIGURE 2D COURTESY DALAL AL AMIR, BDS
In placing a dam for a simple restoration, a fast-acting anesthetic would be used, followed by isolation, placement of the saliva ejector, and, almost immediately, initiation of the preparation. With the proper use of a dam, vision of the operating field, tongue blockage and cheek retraction are no longer issues.
It is common for dental schools to teach a high degree of precision when it comes to placing dental dams. Stamps are often used to guide hole placement (a technique in which small holes are punched to optimize the creation of a seal around teeth) and the dam may be inverted around the teeth with specialized instruments to facilitate the seal. Commonly, the dam clamp is placed on the tooth first and the rubber dam stretched over the bow of the clamp and adapted to the teeth. Technique-wise, this can prove challenging.
CLINICAL APPROACH TO PLACEMENT
Dental dams are available in various thicknesses and colors (and, of course, in rubber and non-latex materials). Generally, heavy or extra heavy material is used in schools, and some practitioners choose heavy materials to help retract soft tissues. Others prefer thin and light-colored (or white) dams as being easiest to work with. Fresh rubber dam material does not tear, and limited quantities should be ordered and stored in a refrigerator. It is worth the extra cost to avoid chairside aggravation. Care needs to be taken regarding latex allergies, so non-latex dams should be available; these can be made from polyethylene, polyvinylchloride or nitrile.

When placing a dental dam, clamps are retained by engaging the tooth below the height of contour. Clamps should be selected that have wings and most closely approximate the size of the tooth (Figure 3). Although clamp designations vary among manufacturers, the basic armamentarium should consist of winged clamps, butterfly-type clamps for anterior teeth, universal premolar clamps and molar clamps. As expertise develops, the practitioner may accumulate a broader inventory of clamp styles. Some situations require ingenuity. During emergency visits, for example, where crown lengthening is not possible, the alveolus is sometimes clamped (Figure 4); other times, slots are used for placement (Figures 5A and 5B).
crown on the canine and eventual treatment.
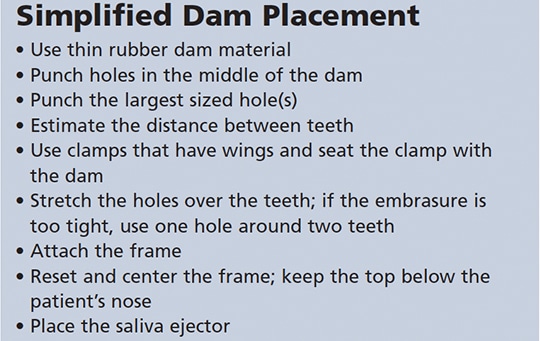
Using a dam punch and the largest sized hole makes placing the holes over teeth easier and helps minimize tearing, especially if using fresh dam material (Figure 6). Punch the hole(s) in the middle of the dam. If using field isolation, punch multiple holes approximately 5 mm apart and in an arc (if appropriate). Placing the bow of the clamp through the hole and engaging the clamp wings eliminates the need for floss on the clamp because the clamp is always outside the dam. When clamps fail, the bow usually breaks; therefore, unless both sides of the clamp have floss, this practice can be considered unwarranted.

Use a plastic frame if performing endodontic therapy (or stainless steel frame for restorative treatment), and (1) place the clamp and dam, isolate the tooth (or teeth), and attach the frame; or (2) place the clamp/dam/frame, isolate the teeth and adjust the frame (Figure 7). If a tooth is tight, place one hole over two teeth, or simply cut the strip between two holes and place over two teeth. A single hole can be stretched over two teeth, as well. Manufacturers also offer alternative combinations of dam frames, shapes, materials and formulations that may suit an operator’s preference (Figure 8).

unit, and adjusted. The use of floss is optional.

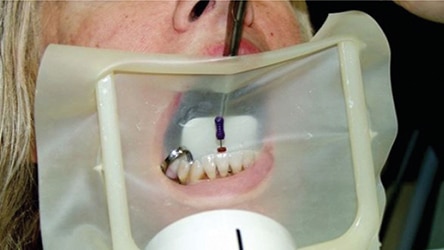
Rearrange the dam on the frame so it is comfortable for the patient and provides the access needed for the procedure. Folding the top of the dam and keeping it below the patient’s nose is preferable to cutting the material around the nose (Figure 9). Place the saliva ejector and/or give the patient control over its placement and use; with a properly placed dam, the saliva ejector will not get in the way. If the dam interferes when managing gingival margins, cut it (as the dam is there to help and not hinder).
The key point is that isolation with a dam is significantly better than if not using one. In addition, if leakage is detected, putties and caulks are available to quickly improve the seal.
CONCLUSION
In summary, a dental dam facilitates treatment and provides a host of clinical benefits that enhance patient safety and improve outcomes. Whether used for restorative or endodontic therapy, dams aid visualization and help protect patients from swallowing instruments or materials; they also provide isolation, moisture control and tissue management. Although an overwhelming wealth of information is available in books, articles and on the Internet about dam technique, by beginning with a simplified approach an operator will soon become more sophisticated and facile in their use. And while there is no single best way to use a dental dam, there is a wrong way — not using one in the first place.
REFERENCES
- Anabtawi MF, Gilbert GH, Bauer MR, et al. Rubber dam use during root canal treatment: findings from The Dental Practice-Based Research Network. J Am Dent Assoc. 2013;144:179–186.
- Savani GM, Sabbah W, Sedgley CM, Whitten B. Current trends in endodontic treatment by general dental practitioners: Report of a United States national survey. J Endod. 2014;40:618–624.
- Going RE, Sawinski VJ. Frequency of use of the rubber dam: a survey. J Am Dent Assoc. 1967;75:158–166.
- Hill EE, Rubel BS. Do dental educators need to improve their approach to teaching rubber dam use? J Dent Educ. 2008;72:1177–1181.
- Silva RF, Martins EC, Prado FB, Júnior JR, Júnior ED. Endoscopic removal of an endodontic file accidentally swallowed: clinical and legal approaches. Aust Endod J. 2011;37:76–78.
- U.S. Food and Drug Administration. Code of Federal Regulations Title 21. Available at: accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=872.6300. Accessed May 4, 2017.
- American Association of Endodontists. AAE position statement: dental dams. Available at: aae.org/uploadedfiles/clinical_resources/guidelines_and_position_statements/dentaldamstatement.pdf. Accessed May 4, 2017.
- Ben-Shahar T. The Pursuit of Perfect: How to Stop Chasing Perfection and Start Living a Richer, Happier Life. New York: McGraw Hill Professional; 2009.
From Decisions in Dentistry. June 2017;3(6):12—14.
