

Dental Pain Management Strategies
An exploration of anesthetic adjuncts as a means to improve patient comfort during therapy.
An exploration of local anesthetic adjuncts as a means to improve patient comfort during therapy
For many patients, the concept of dental pain is a true fear.1–3 While pain and anxiety management in dentistry has greatly evolved through the use of behavior modification and nitrous oxide, as well as oral and intravenous sedatives, local anesthesia remains the backbone of the profession.4 Patient comfort before, during and after a dental procedure is an essential component of care, and understanding the available armamentarium is critical in determining which method or methods are best for the patient and practitioner. Fortunately, advances in the profession have improved local anesthesia delivery.5,6 In light of these developments, this article will explore various approaches and strategies for anesthesia delivery that will enhance patient comfort.
Amide anesthetics are the main tool used for localized pain management in dentistry. Anesthetic agents manufactured for the dental profession are available in plain form, but, more commonly, are combined with vasoconstrictors, keeping the anesthetic localized at its deposition site, thus maximizing longevity of perceived numbness.5
Perhaps the most common tool for dental pain management is a 2% lidocaine hydrochloride (HCl) solution with 1:100,000 epinephrine. A cartridge with up to 1.8 ml of 2% lidocaine with 1:100,000 epinephrine provides duration of approximately 60 to 90 minutes when using an injection block technique for pulpal anesthesia.7 Any cartridge may contain 1.8 ml of solution, but the average volume is 1.76 ml and recommendations to calculate dosage should err on the higher volume for safety purposes.8
Other anesthetic solutions with higher doses (3% or 4%) can be used without vasoconstrictors. These plain solutions have a pH of 5.9 (compared with to an anesthetic-with-vasoconstrictor solution’s 3.5 pH).9 Plain solutions are generally helpful for basic dental procedures on individuals who are sensitive to vasoconstrictor agents.10
Recently, 4% articaine HCl with epinephrine is gaining popularity due to its efficacy when used with the infiltration technique, particularly in the maxilla.11 This 4% articaine solution is unique, as it is an amide and ester hybrid-class anesthetic.12,13 The presence of a thiophene ring within the molecule (instead of a benzene ring) improves lipid solubility.14 The dental profession has also seen progress in endodontic “hot teeth” instances in which 2% solution with epinephrine is provided in a mandibular block, followed with supplemental 4% articaine HCl and 1:200,000 epinephrine buccal and lingual infiltrations in the mandible.15
RETRACTION AND PATIENT COMFORT
Preliminary evidence has started to surface in the literature describing the use of a mouth mirror as a comfortable alternative to using a finger for retraction prior to injection.16 Considering the risk of needlestick injury when a finger is used for retraction,17,18 employing fingerless retraction helps clinicians avoid unnecessary exposure.19

Patient comfort during local anesthesia delivery is an important aspect of care, and it is in the practitioner’s best interest to consider using a technique that will improve the patient experience. For example, prior to administering a local anesthetic drug, drying the injection site with gauze and applying a topical anesthetic for at least 60 seconds will improve patient comfort through peripheral numbing of the tissue prior to the actual injection.20
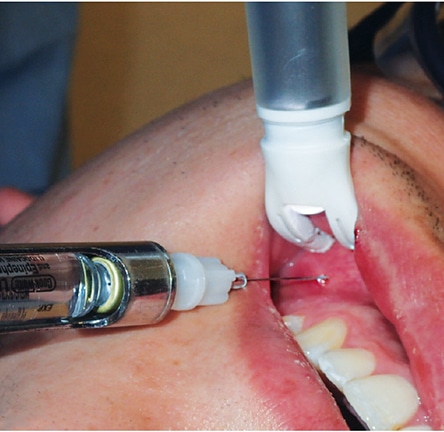
In 2008, the U.S. Food and Drug Administration (FDA) approved a mixing pen device to help exchange sodium bicarbonate with anesthetic in the cartridge (Figure 1). This device provided one of the first opportunities to buffer anesthetic for dental procedures. By altering the pH of anesthetic solution from acidic to neutral, a buffered anesthetic reduces pain perception during delivery.21–23 This device uses an anesthetic cartridge and sodium bicarbonate vial that are inserted into the mixing pen, and the clinician presses a button to activate a measured solution exchange.23 Another buffering system employs a multiuse anesthetic vial, sodium bicarbonate syringe, and disposable syringes with haptic feedback. When all components are in place and primed, the buffered solution is extracted using the haptic syringe (Figure 2) and a needle is added for delivery.

As proposed by Melzack and Wall,24 gate control theory describes how alpha-beta nerve fibers transmit information from vibration and touch receptors of the skin, stimulating inhibitory interneurons in the spinal cord. These neurons aid in the pain signal reduction to C fibers from the skin to the second-order neurons that cross the spinal cord midline and ascend to the brain.24,25 Therefore, adding an oscillating vibratory stimulus to the tissue prior to injection may reduce the perceived discomfort of needle puncture.
A rechargeable device that makes use of the gate control theory features disposable tips and LED lighting to illuminate the injection site (Figure 3). It applies intermittent oscillating vibrations to stimulate and distract nerve cells from needle insertion. This minimizes patient perception of pain, as the oscillations continue even after the injection is delivered.26
Another technique for reducing discomfort and improving ergonomics is computer controlled local anesthesia delivery (Figure 4). This technology controls the rate of delivery via a computer and foot pedal. Some systems help alleviate patient apprehension by avoiding the appearance of a traditional syringe. One system, for example, uses a disposable handpiece that dispenses anesthetic using a foot pedal and voice commands to regulate flow rate through the handpiece.27

local anesthesia delivery unit.
NEEDLELESS NASAL DELIVERY
Indicated for regional anesthesia when performing restorative procedures on teeth #4 through #13 and A through J in patients weighing 40 kilograms (88 pounds) or more, the most recent FDA-approved advance in anesthesia delivery is a needleless, intranasal spray consisting of tetracaine HCl (6 mg) and oxymetazoline HCl (0.1 mg) combined in a single-use 0.2-ml sprayer. In a 2016 study, Hersh et al28 administered the spray into patients’ nostrils ipsilateral to the tooth being treated. They concluded this form of delivery provides an effective, needleless alternative for obtaining maxillary pulpal anesthesia on premolars, canines and incisors.
REVERSAL OF SOFT-TISSUE ANESTHESIA
Clinicians should also be cognizant of managing patients’ postoperative comfort. Phentolamine mesylate helps reverse the action of the vasoconstrictor used earlier in the dental appointment. Delivered toward the end of the procedure, this agent reduces the chance of postoperative injury due to prolonged numbness (cheek biting, for example), as it returns the patient to baseline more quickly than if a reversal agent was not used.29–31
CONCLUSION
Anesthesia delivery methods continue to evolve and the armamentarium for pain management is larger than ever. It is important for clinicians to be knowledgeable about the various tools available to manage pain. Remaining abreast of the latest developments and adjuncts in this area is not only key to patient comfort and satisfaction, it is also a practice builder.
KEY TAKEAWAYS
- Patient comfort during local anesthesia delivery is an important aspect of care, and it is in the practitioner’s best interest to consider using a technique that will improve the patient experience.
- Advances have improved local anesthesia delivery, and understanding the pain management armamentarium is critical to determining which method or methods are best for the patient and practitioner.
- A 4% articaine hydrochloride with epinephrine solution — an amide and ester hybrid-class anesthetic — is gaining popularity due to its efficacy when used with the infiltration technique, particularly in the maxilla.11–13
- Considering the risk of needlestick injury,17,18 employing fingerless retraction helps clinicians avoid unnecessary exposure.19
- Local anesthetic adjuncts can enhance patient comfort during dental treatment.
- Remaining abreast of the latest developments and adjuncts for pain management is key to patient satisfaction — and is also a practice builder.
References
- American Dental Association survey. Influences on dental visits. ADA News. 1998;11:4.
- Crawford S, Nissen L, Wong S, Dowling E. Quantification of patient fears regarding dental injections and patient perceptions of a local noninjectable anesthetic gel. Compend Contin Educ Dent. 2005:26(Suppl 1):11–14.
- Berggren U, Meynert G. Dental fear and avoidance: causes, symptoms, and consequences. J Am Dent Assoc. 1984:109:247–251.
- Malamed SF. Pain and anxiety control in dentistry. J Calif Dent Assoc. 1993;2:35–38.
- Hawkins JM, Moore PA. Local anesthesia: advances in agents and techniques. Dental Clinics. 2002:46:719–732.
- Deepika A, Chandrasekhar R, Vinay C, Uloopi K, Rao V. Effectiveness of two flavored topical anesthetic agents in reducing injection pain in children: a comparative study. J Clin Pediatr Dent. 2012;37:15–18.
- Haas DA. An update on local anesthetics in dentistry. J Can Dent Assoc. 2002;68:546–552.
- Becker DE, Reed KL. Local anesthetics: review of pharmacological considerations. Anesth Prog. 2012;59:90–102.
- Malamed SF. Buffering local anesthetics in dentistry. The Pulse. 2011;44:7–9.
- Malamed SF. Handbook of Local Anesthesia. 6th ed. St. Louis: Elsevier; 2014:52–75.
- Srinivasan N1, Kavitha M, Loganathan CS, Padmini G. Comparison of anesthetic efficacy of 4% articaine and 2% lidocaine for maxillary buccal infiltration in patients with irreversible pulpitis. Oral Surg Oral Med Oral Path Oral Radiol Endod. 2009; 107:133–136.
- Malamed SF, Gagnon S, Leblanc D. Efficacy of articaine: a new amide local anesthetic. J Am Dent Assoc. 2000;131:635–642.
- Bataineh AB, Alwarafi MA. Patient’s pain perception during mandibular molar extraction with articaine: a comparison study between infiltration and inferior alveolar nerve block. Clinical Oral Investig. 2016;20:2241–2250.
- Lima JL, Dias-Ribeiro E, Ferreira-Rocha J, et al. Comparison of buccal infiltration of 4 % articaine with 1:100,000 and 1:200,000 epinephrine for extraction of maxillary third molars with pericoronitis: a pilot study. Anesth Prog. 2013;60:42–46.
- Haase A, Reader A, Nusstein J, Beck M, Drum M. Comparing anesthetic efficacy of articaine versus lidocaine as a supplemental buccal infiltration of the mandibular first molar after an inferior alveolar nerve block. J Am Dent Assoc. 2008;139:1228–1235.
- Fa BA, Cuny E. Preliminary evidence supports modification of retraction technique to prevent needlestick injuries. Anesth Prog. 2016;63:192–196.
- Makary MA, Al-Attar A, Holzmueller CG, et al. Needlestick injuries among surgeons in training. N Engl J Med. 2007;356:2693–2699.
- David HT, Aminzadeh KK, Kae AH, Radomsky SC. Instrument retraction to avoid needle-stick injuries during intraoral local anesthesia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103:e11–e13.
- Alvear Fa B, Gupta S, Bhattacharyya M. Operator preference of retraction method during anesthesia delivery. Stoma Edu J. 2016;3:10–15.
- Ogle, OE, Mahjoubi G. Local anesthesia: agents, techniques, and complications. Dent Clin North Am. 2012;56:133–148.
- Masoud S, Khademi A, Baghaei B, Noormohammadi H. Effect of sodium bicarbonate–buffered lidocaine on the success of inferior alveolar nerve block for teeth with symptomatic irreversible pulpitis: A prospective, randomized double-blind study. J Endod. 2015;41:33–35.
- Davies RJ. Buffering the pain of local anaesthetics: a systematic review. Emerg Med (Fremantle). 2003;15:81–88.
- Malamed SF, Tavana S, Falkel M. Faster onset and more comfortable injection with alkalinized 2% lidocaine with epinephrine 1:100,000. Comp Contin Educ Dent. 2013;34:10–20.
- Melzack R, Wall PD. Pain mechanisms: a new theory. Science.1965;150:971–979.
- Dickenson AH. Gate control theory of pain stands the test of time. Br J Anaesth. 2002;88:755–757.
- Ching D, Finkelman M, Loo CY. Effect of the DentalVibe injection system on pain during local anesthesia injections in adolescent patients. Pediatr Dent. 2014;36:51–55.
- Thoppe-Dhamodhara YK, Asokan S, John BJ, Pollachi-Ramakrishnan G, Ramachandran P, Vilvanathan P. Cartridge syringe vs computer controlled local anesthetic delivery system: Pain related behaviour over two sequential visits — a randomized controlled trial. J Clin Exp Dent. 2015;7:e513–e518.
- Hersh EV, Pinto A, Saraghi M, et al. Double-masked, randomized, placebo-controlled study to evaluate the efficacy and tolerability of intranasal K305 (3% tetracaine plus 0.05% oxymetazoline) in anesthetizing maxillary teeth. J Am Dent Assoc. 2016;147:278–287.
- Hersh EV, Moore PA, Papas AS, et al. Reversal of soft-tissue local anesthesia with phentolamine mesylate in adolescents and adults. J Am Dent Assoc. 2008;139:1080–1093.
- Tavares M, Goodson JM, Studen-Pavlovich D, et al. Reversal of soft-tissue local anesthesia with phentolamine mesylate in pediatric patients. J Am Dent Assoc. 2008;139:1095–1104.
- Hersh EV, Lindemeyer RG. Phentolamine mesylate for accelerating recovery from lip and tongue anesthesia. Dent Clin North Am. 2010;54:631–642.
The authors have no commercial conflicts of interest to disclose.
Featured Image by MSTROZ/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. June 2017;3(6):16—18,21.
