
 FANGXIANUO/E+/GETTY IMAGES PLUS
FANGXIANUO/E+/GETTY IMAGES PLUS
Correcting Bilateral Ectopically Erupting First Molars
A case presentation documenting correction of bilateral ectopically erupting maxillary first permanent molars with elastomeric separators and disking.
Ectopic eruption of a first permanent molar reflects an abnormal mesioangular eruption path, resulting in root resorption of the adjacent second primary molar.1 This developmental disturbance has been most frequently reported in the maxillary molars and canines.2 The prevalence of ectopically erupting first permanent molars is approximately 3%, with little difference in the involvement of the quadrant. However, it has been suggested it occurs more frequently in the maxillary dental arch.3 The exact etiology is poorly recognized and has been associated with factors such as heredity, abnormal size of the first permanent molars, insufficient arch size, and abnormal angulation of the path of eruption.4–6
The literature classifies ectopic eruption of permanent molars as reversible or irreversible. In the reversible type, the ectopic molar spontaneously self-corrects. Additionally, the literature suggests that two-thirds of ectopically erupting permanent molars are reversible.2 In the irreversible type, if interceptive treatment is not provided in a timely manner, the molar remains impacted under the distal surface of the adjacent second primary molar, resulting in premature exfoliation of the latter and subsequent space loss for the eruption of the second bicuspid.2,7 In this clinical scenario, treatment to correct the ectopic eruption becomes costly and complex; such cases will also require more time to solve. Factors negatively associated with irreversible ectopic eruption have been reported that may require early intervention, including increased magnitude of impaction, increased resorption of the primary tooth, and bilateral involvement of the first permanent molar.8

Several techniques for correction have been proposed. Treatment depends on the severity of the impaction of the first permanent molar. For mild impactions, elastomeric orthodontic separators, brass ligature or helical springs can be used to wedge the first permanent molar distally.1,9 In cases of moderate to severe impactions, a distalizing appliance — such as the Humphrey or Halterman appliance — may be indicated.3 Additionally, more severe cases require more complex treatment, including potential extraction of the second primary molar, followed by the use of a space maintainer to prevent untoward tooth movement until the second premolar erupts.9 Disking of the distal surface of the second primary molar may be an alternative to treat the ectopic eruption of the permanent molar. This method might allow keeping the second primary molar while preserving space for the eruption of the second permanent bicuspid, thus reducing the time, cost and complexity of treatment. To the authors’ knowledge, no other case reports have been published using this method to allow the maxillary first permanent molars to erupt into occlusion with minimal space loss.
Therefore, the purpose of this case report is to demonstrate the correction of bilateral ectopically erupting maxillary first permanent molars using two simple, time- and cost-effective techniques involving elastomeric separators and disking of the adjacent second primary molar.
Case Description
A 7-year-old healthy female presented to the Department of Pediatric Dentistry and Community Health clinic at Rutgers School of Dental Medicine for routine dental care. Extraoral examination revealed a concave profile with Class III tendency. The intraoral examination noted that she had an early mixed dentition, with fully erupted mandibular first permanent molars and bilateral partially erupted maxillary first permanent molars, over-retained primary mandibular central incisors, and generalized mild crowding. Panoramic radiography revealed impaction and ectopic eruption of the permanent maxillary first molars, with the mesial part of their crowns impacted under the distal clinical crown of the second primary molars (Figure 1).
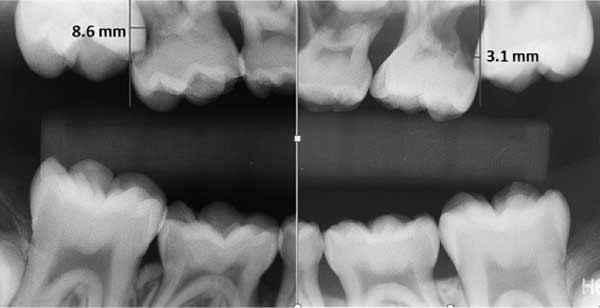
Clinically, the adjacent second primary molars did not exhibit any mobility, despite moderate root resorption. The patient reported no pain or discomfort related to the ectopic eruptions. No clinical signs or symptoms suggestive of pulpal damage of the second primary molars were evident. Based on the method reported by Barberia-Leache et al,2 the magnitude of impaction of the permanent maxillary right first molars was 8.6 mm, and 3.1 mm for the permanent maxillary left first molar (Figure 2). The patient was treatment planned for interproximal wedging using elastomeric separators, with the goal to distalize the permanent maxillary first molars. However, taking into consideration the magnitude of impaction was higher on the permanent maxillary right first molar, additional treatment was anticipated.
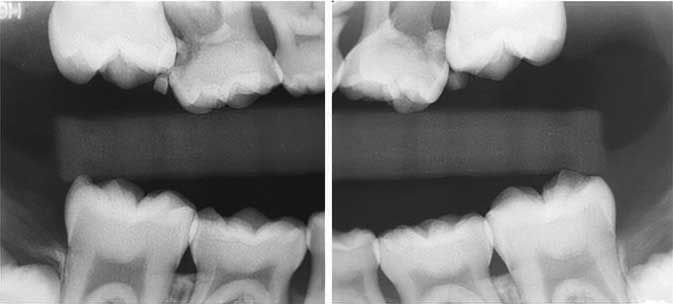
At the initial visit, single blue elastomeric separators with a diameter of 2.5 mm were stretched and placed mesial to the permanent maxillary first molars. The patient was rescheduled for follow-up in two weeks. At the follow-up visit, bitewing radiographs revealed mild distal movement of the permanent maxillary first molars (Figure 3). Due to the higher magnitude of impaction on the permanent maxillary right first molar, a decision was made to perform disking of the distal surface of the primary maxillary right second molar, with the goal of disengaging the mesial surface of the adjacent permanent maxillary right first molar. After the elastomeric separator on the upper right side was removed, approximately 36 mg of articaine hydrochloride 4% with 1:100,000 epinephrine was used for buccal infiltration of the primary maxillary right second molar. Disking was completed with a tapered, medium-grit diamond bur and the surface was polished with a flame finishing stone, followed by topical fluoride varnish application.
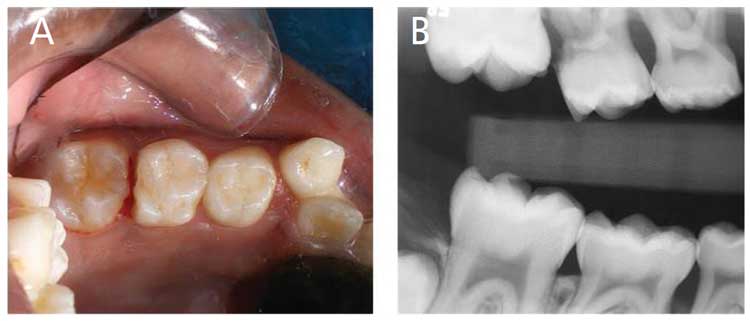
An intraoral photograph and a bitewing radiograph taken postoperatively revealed disengagement of the mesial aspect of the permanent maxillary right first molar (Figures 4A and 4B). The elastomeric separator on the left side was replaced and the patient was followed up at two-week intervals. After three months of follow-up — including the replacement of the elastomeric separator on the left side at two-week intervals — clinical and radiographic examination showed complete correction of the ectopically erupting permanent maxillary first molars (Figure 5 and Figure 6). No further treatment was advised, as the permanent maxillary first molars were erupting into occlusion.
Discussion
Ectopic eruption of the first permanent molar is a painless condition that frequently causes resorption of the adjacent second primary molar. As has been reported in previous studies, this case showed an increased magnitude of impaction, increased resorption of the primary maxillary second molars, and bilateral involvement of the permanent maxillary first molars requiring early intervention. Furthermore, according to previous studies, the majority of reversible ectopic eruption cases that self-correct occur by age 7.2,7,10 Based on this information, the current case was considered an irreversible ectopic eruption, and a decision was made to initiate interceptive intervention.
In a retrospective study involving the radiographs of 509 children, a higher frequency of ectopic eruption and an increased magnitude of impaction were observed on the right side of the arch.2 The authors measured the magnitude of permanent molar impaction by drawing a tangent line to the distal wall of the second primary molar perpendicular to its occlusal plane. The distance of the maximum mesial convexity of the first permanent molar was measured from the extension of the distal plane toward the apical region of the second primary molar. Based on this proposed method (and as previously noted), the magnitude of impaction of the permanent maxillary right first molar in the current case was 8.6 mm, and 3.1 mm for the permanent maxillary left first molar (Figure 2). Therefore, in accordance with the aforementioned retrospective study, the magnitude of impaction was higher on the right side and therefore required additional intervention involving disking of the adjacent second primary molar. The distal surface disking of the primary maxillary right second molar resulted in insignificant loss of arch length due to the utilization of leeway space.11,12 Similar to the current case, Duncan and Ashrafi13 reported a case of an ectopically erupting first permanent mandibular molar which was corrected within six months by reducing the distal surface of the primary mandibular second molars.

For cases with more severe impactions, orthodontic appliances are often proposed in the literature.3,14–16 Orthodontic appliances require laboratory time for fabrication, as well as patient cooperation and extended chairtime; in some cases, treatment can become expensive and complicated. Conversely, the disking method appears to be an underutilized treatment for correction of impacted molars. In this case report, the bilateral ectopic eruption of the maxillary molars was corrected in three months without additional cost, demonstrating that it was a time- and cost-effective treatment. Additionally, it was determined that the use of the elastomeric separator and disking of the primary maxillary right second molar allowed for the permanent maxillary first molar to change its ectopic mesial angulation to a more optimal upright position, with minimal loss of arch length. This improved chances for the permanent molar to erupt into a Class I or an end-to-end molar relationship. In this case, a Class I molar relationship was obtained on the left side, while an end-to-end molar relationship was observed on the right side. Considering the leeway space in the mandible, it was expected the mesial shift of the permanent mandibular right molar will allow a Class I molar relationship later.12
This case highlights the importance of preventing premature exfoliation of second primary molar, resulting in additional loss of arch length. The literature indicates that many patients with ectopic eruption of permanent molars require further orthodontic treatment due to a crowded permanent dentition.13,17–19 In this case, the patient was referred for further orthodontic evaluation to avoid a more complex orthodontic treatment if needed in the future.

Summary
When the benefits of early treatment are weighed against the consequences of untreated cases of ectopic eruption, it is suggested that treatment should be initiated as soon as the condition is diagnosed so as to allow a normal eruption pathway and prevent detrimental effects on a developing occlusion. Additionally, based on the findings of the current case report, it could be concluded that an ectopically erupting permanent molar with a magnitude ≤ 3.1 mm can benefit from interproximal wedging using an elastomeric separator; and, in cases with a larger magnitude of impaction, a combination of interproximal wedging with an elastomeric separator and disking of the primary maxillary second molar to allow eruption of the permanent maxillary first molars. More research — including a large sample size — is required to evaluate the effectiveness of various treatment modalities based on the magnitude of impaction.
Key Takeaways
- Ectopic eruption of a first permanent molar reflects an abnormal mesioangular path, leading to resorption of the adjacent second primary molar and potential loss of space for the eruption of the second permanent bicuspid.
- This manuscript presents a case report for the correction of bilateral, ectopically erupting maxillary first permanent molars using time- and cost-effective clinical techniques involving elastomeric separators and disking of the second primary molar.
- The literature classifies ectopic eruption of permanent molars as reversible or irreversible.
- The case described in this report was considered an irreversible ectopic eruption, and the decision was made to initiate interceptive intervention.
Acknowledgments
The authors thank Jorge Alonso Caceda and Gerald Guzy, DDS, for their time and assistance in reviewing this manuscript.
References
- Hirayama K, Chow MH. Correcting ectopic first permanent molars with metal or elastic separators. Pediatr Dent. 1992;14:342–344.
- Barberia-Leache E, Suarez-Clúa MC, Saavedra-Ontiveros D. Ectopic eruption of the maxillary first permanent molar: characteristics and occurrence in growing children. Angle Orthod. 2005;75:610–615.
- Yaseen SM, Naik S, Uloopi KS. Ectopic eruption — a review and case report. Contemp Clin Dent. 2011;2:3–7.
- Bjerklin K. Ectopic eruption of the maxillary first permanent molar. An epidemiological, familial, aetiological and longitudinal clinical study. Swed DenJ J Suppl. 1994;100:1–66.
- Pulver F. The etiology and prevalence of ectopic eruption of the maxillary first permanent molar. ASDC J Dent Child. 1968;35:138–146.
- Ambriss B, Moukarzel C, Noueiri B. Management of bilateral ectopically erupting maxillary molars: a case report. Int J Clin Pediatr Dent. 2019;12:153–156.
- Bjerklin K, Kurol J. Prevalence of ectopic eruption of the maxillary first permanent molar. Swed Dent J. 1981;5:29–34.
- Dabbagh B, Sigal MJ, Tompson BD, Titley K, Andrews P. Ectopic eruption of the permanent maxillary first molar: Predictive factors for irreversible outcome. Pediatr Dent. 2017;39:215–218.
- Kupietzky A. Correction of ectopic eruption of permanent molars utilizing the brass wire technique. Pediatr Dent. 2000;22:408–412.
- Kurol J, Bjerklin K. Resorption of maxillary second primary molars caused by ectopic eruption of the maxillary first permanent molar: a longitudinal and histological study. ASDC J Dent Child. 1982;49:273–279.
- Lin BP-J. Passive space management in children. Decisions in Dentistry. 2018;4(7):13–14,17–18.
- Andley Y, Saraf BG, Sheoran N, Nisha D. Too much too soon, rather than in too little too late: Orthodontic in mixed dentition. Int J Appl Dent Sci. 2019;5:374–381.
- Duncan WK, Ashrafi MH. Ectopic eruption of the mandibular first permanent molar. J Am Dent Assoc. 1981;102:651–654.
- Seehra J, Winchester L, DiBiase AT, Cobourne MT. Orthodontic management of ectopic maxillary first permanent molars: a case report. Aust Orthod J. 2011;27:57–62.
- Gehm S, Crespi PV. Management of ectopic eruption of permanent molars. Compend Contin Educ Dent. 1997;18:561–566,568–570.
- Halterman CW. A simple technique for the treatment of ectopically erupting permanent first molars. J Am Dent Assoc. 1982;105:1031–1033.
- Sharma PS, Rypel TS. Ectopic eruption of permanent molars and their management (I). Quintessence Int Dent Dig. 1978;9:47–52.
- Young DH. Ectopic eruption of the first permanent molar. J Dent Child. 1957;24:153–162.
- O’Meara WF. Ectopic eruption pattern in selected permanent teeth. J Dent Res. 1962;41:607–616.
From Decisions in Dentistry. November 2021;7(11)8,10,12.
