
 FATIDO/E+/GETTY IMAGES PLUS
FATIDO/E+/GETTY IMAGES PLUS
Coronavirus Transmission In the Dental Setting
Oral health professionals should remain up-to-date on the coronavirus, and clinical measures to prevent its transmission in the dental setting.
PURCHASE COURSE
This course was published in the April 2020 issue and expires April 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the April 2020 issue and expires April 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe the nature of coronaviruses, the types of illnesses they cause, and routes of transmission.
- Discuss the estimated incubation period for 2019 novel coronavirus (COVID-19), and risk factors for various patient populations.
- Explain appropriate clinical responses to the COVID-19 pandemic, and what oral health professionals can do to prevent its spread in the dental setting.
INTRODUCTION
The 2019 novel coronavirus, which manifests as COVID-19, is described as the defining global health crisis of our time. The most recent disease to be classified by the World Health Organization as a pandemic, COVID-19 joins cholera, bubonic plague, smallpox and influenza as among the most brutal killers in history. As researchers work to develop pharmaceutical interventions for COVID-19, valiant efforts are being made worldwide to prevent or reduce transmission. Health care professionals are facing unprecedented circumstances related to patient care and growing concern about this deadly disease; for example, the American Dental Association recommends that dental practices nationwide postpone elective procedures to slow its spread.
This article reviews the emergence, transmission pathways and symptoms of COVID-19, and also provides clinical strategies to help mitigate the pandemic. As a dental professional and educator, I am confident this article will guide dental teams in complying with best practices and providing care in accordance with U.S. Centers for Disease Control and Prevention guidelines, ultimately protecting patients, staff and the community at large.
—Leann Keefer, RDH, BSEd, MSM
Director, Clinical Services
Crosstex International
By providing care in accordance with recommended asepsis guidelines, dental teams can protect patients and staff and help slow the COVID-19 pandemic
In late 2019, an outbreak of atypical pneumonia of unknown cause presented in Wuhan in China’s Hubei Province. Upon investigation, the confirmed cases were linked to a Wuhan market where wild animals, including marmots, birds, rabbits, bats and snakes, were being traded illegally.1 On December 31, 2019, the World Health Organization (WHO) was notified of this outbreak by authorities in China. Virological testing disclosed a novel coronavirus in these patients, and, within a few weeks, WHO tentatively named it as 2019 novel coronavirus (2019-nCoV).2
On February 11, 2020, the International Committee on Taxonomy of Viruses announced the new name of the virus as severe acute respiratory syndrome coronavirus, or SARS-CoV-2.3 This was chosen due to the virus being genetically related to the coronavirus responsible for the SARS outbreak in 2003.3 On the same day, WHO named the new disease COVID-19, following guidelines previously developed with the World Organization for Animal Health and Food and Agricultural Organization of the United Nations.3 Regardless of the nomenclature, this fast-spreading disease poses a global health risk. Consequently, dental teams should remain up-to-date on its presentation, and clinical measures to prevent its transmission in the dental setting.
Coronaviruses (CoV) are a large family of viruses that cause illness ranging from respiratory infections (including the common cold to flu-like or pneumonia symptoms), as well as gastrointestinal symptoms — all which may or may not appear and range in severity.4 Middle East respiratory syndrome (MERS-CoV) and SARS-CoV outbreaks continue to occur globally.4 A novel coronavirus (nCoV) is a new strain that has not been previously identified in humans, and is considered a zoonotic disease that spreads from animals to humans. Further investigations determined the source of SARS-CoV transmission was from civet cats to humans and MERS-CoV from dromedary camels to humans.4 Although the specific source of COVID-19 has not been identified, bats and pangolins are currently implicated. As a novel coronavirus, the information scientists have gathered about it may change as researchers and the medical community continue to learn how the virus behaves.5
The U.S. Centers for Disease Control and Prevention (CDC) reinforced the need for clinicians to be watchful for exposure to COVID-19, not only with patients who are returning travelers from areas with high incidence of the disease, but also with individuals who have come in contact with those infected.6 Given the nature of oral health care and disease transmission, dental teams need to stay abreast of this rapidly evolving public health threat.
TRANSMISSION
Cases of COVID-19 continue to spread globally. As of April 9, 2020, more than 1.5 million cases had been reported worldwide, with 89,877 deaths.7,8 The disease has spread via travel from China to at least 177 countries, with evidence of sustained transmission on six continents.8 As of April 9, 2020, the United States had more than 395,000 confirmed cases across all 50 states, with 12,754 deaths.7,9,10
Chinese officials confirmed the COVID-19 outbreak was associated with the Huanan Seafood Market, a “wet market” in Wuhan.11 Wet markets sell live fish and animals, and have a history of transmitting viruses. Typically, purchases are immediately slaughtered on site, which can cause particles of infectious bacteria or viruses to become aerosolized and transmit from animals to people.11 Investigators suspect that someone purchased contaminated meat, became sick before or after consuming it, and spread the infection to others.12 Though the virus can spread by consuming infected animals, it can also spread through coughing, sneezing and close contact with an infected person or an object carrying the virus.12
According to CDC officials, it may be possible to contract COVID-19 by touching a surface or object that has the virus on it and then touching the mouth, nose or possibly eyes, but this is not a confirmed primary mode of transmission.12 With most respiratory viruses, people are typically considered most contagious when they present with acute symptoms.12 Presently, it is not clear how contagious those infected with the virus are during the incubation period; however, there have been reports of transmission in individuals who show no signs or symptoms of the disease.13
SIGNS, SYMPTOMS AND PREVENTION
Signs and symptoms of COVID-19 are similar to other respiratory illnesses, and can include runny nose, sore throat, fever, cough, shortness of breath, and breathing difficulties. In more advanced cases, infections can lead to pneumonia, severe acute respiratory syndrome, kidney failure and death.4,14 Because the symptoms of the coronavirus are similar to that of other common respiratory infections (such as a cold or flu), a definitive diagnosis can only be made with a laboratory test.4,14
The severity of symptoms in confirmed cases has ranged from no or mild symptoms to severe.15 The incubation period — as reported by the CDC at presstime — is between two to 14 days from exposure to the occurrence of disease signs and symptoms.15 By comparison, WHO estimates that incubation ranges between one and 12.5 days, with a median of five to six days.14 The estimates for the incubation period for COVID-19 are based on previous observations with other coronavirus diseases, such as SARS and MERS.14,15
The elderly and individuals who present with preexisting medical conditions, such as heart disease, high blood pressure, cancer, diabetes or lung conditions, seem to experience more serious complications.15 At this time, there is no research regarding the susceptibility of pregnant women to the virus, and no evidence to suggest children are at increased risk.16
On January 30, 2020, WHO classified the rapidly spreading outbreak as a Public Health Emergency of International Concern,5,17 and on March 11 WHO declared it a pandemic. In response to the outbreak, the CDC has partnered with health officials and health care systems to reduce the impact of the virus and reinforce infection prevention principles. The CDC is using a 2017 Morbidity and Mortality Weekly Report as a blueprint for community interventions and adapting it to COVID-19.18,19 With no vaccine available to prevent coronavirus disease, the CDC recommends everyday preventive actions to halt the spread of respiratory diseases, including COVID-19 (Table 1).20
RESOURCES FOR CLINICIANS
The CDC maintains a comprehensive site for health care professionals that includes preparedness resources to assist providers, clinics and hospitals when managing patients with potential or confirmed cases of COVID-19. These assets include a flowchart to help identify and assess patients who may be ill with, or who may have been exposed to the disease.21
The CDC also offers a clinical criteria form to guide evaluation for individuals under investigation for COVID-19 based on what is known about MERS-CoV and SARS-CoV.22 In the event a person under investigation for COVID-19 presents in dental practice, clinicians should immediately notify the appropriate infection prevention personnel at their health care facility, as well as local and state health departments.22
The American Dental Association (ADA) and American Dental Hygienists’ Association have issued statements and provided resources related to COVID-19.23,24 As of presstime, each organization also recommends that oral health professionals postpone elective and nonemergency procedures, but remain available for dental emergencies that are considered “potentially life threatening,” according to the ADA.23,24 Once active practice resumes, it will be more important than ever for dental settings to follow standard precautions and infection control, as outlined in the CDC’s Guidelines for Infection Control in Dental Health-Care Settings — 2003.25
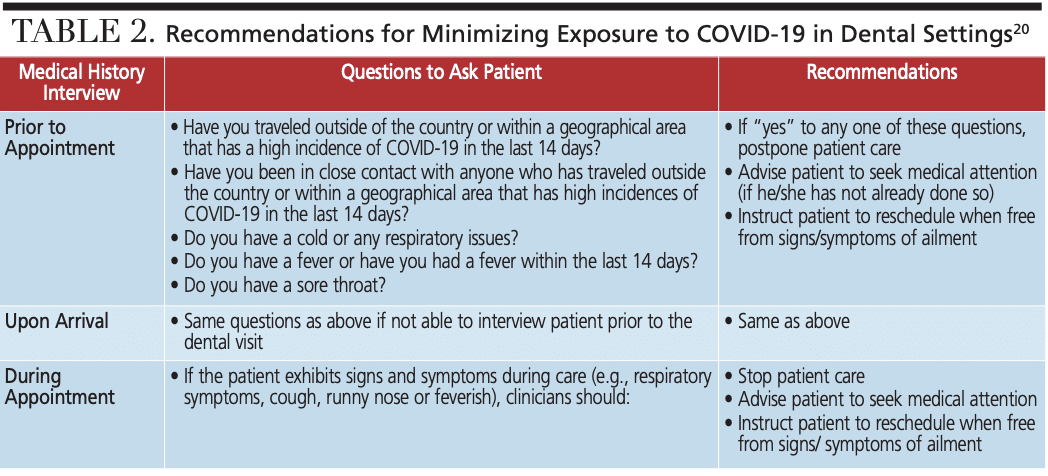
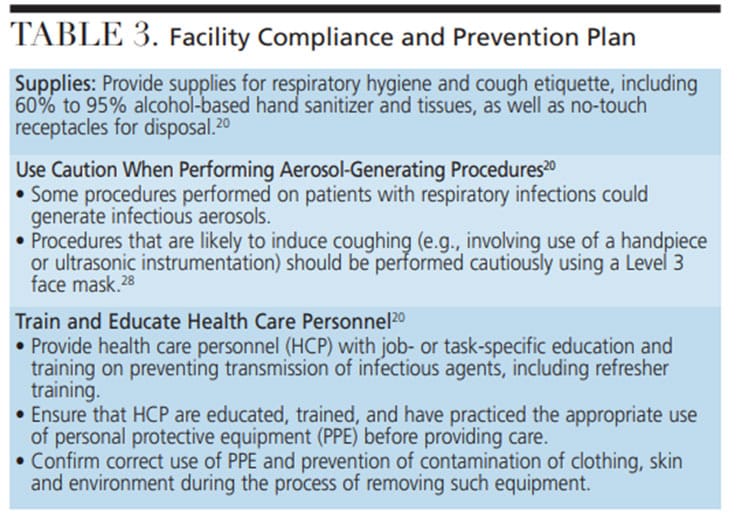
Dental health care personnel (DHCP) who are in contact with patients, and whose responsibilities include cleaning and disinfecting, handling contaminated supplies or equipment, and who work in proximity to potentially contaminated surfaces, should diligently follow all infection prevention procedures.20 To prevent infections from spreading during health care delivery, an effective asepsis protocol — including administrative rules, engineering controls, environmental hygiene, correct work practices, and appropriate use of personal protective equipment (PPE) — is essential. The CDC provides infection control guidance for health care settings.20 These are basic rationale and techniques familiar to DHCP for exposure control, including hand hygiene. Recommendations for minimizing exposure to COVID-19 in the dental setting (Table 2) include taking a comprehensive medical history, and implementing a facility compliance and prevention plan (Table 3). A recent literature review on coronaviruses, including SARS, MERS and endemic human coronaviruses, revealed that each can remain on surfaces — such as metal, glass or plastic — for up to nine days. Surface disinfectant protocols with 62% to 71% ethanol (rubbing) alcohol, 0.5% hydrogen peroxide, or 0.1% sodium hypochlorite (bleach) can inactivate the viruses within 60 seconds of contact time.26
PERSONAL PROTECTIVE EQUIPMENT
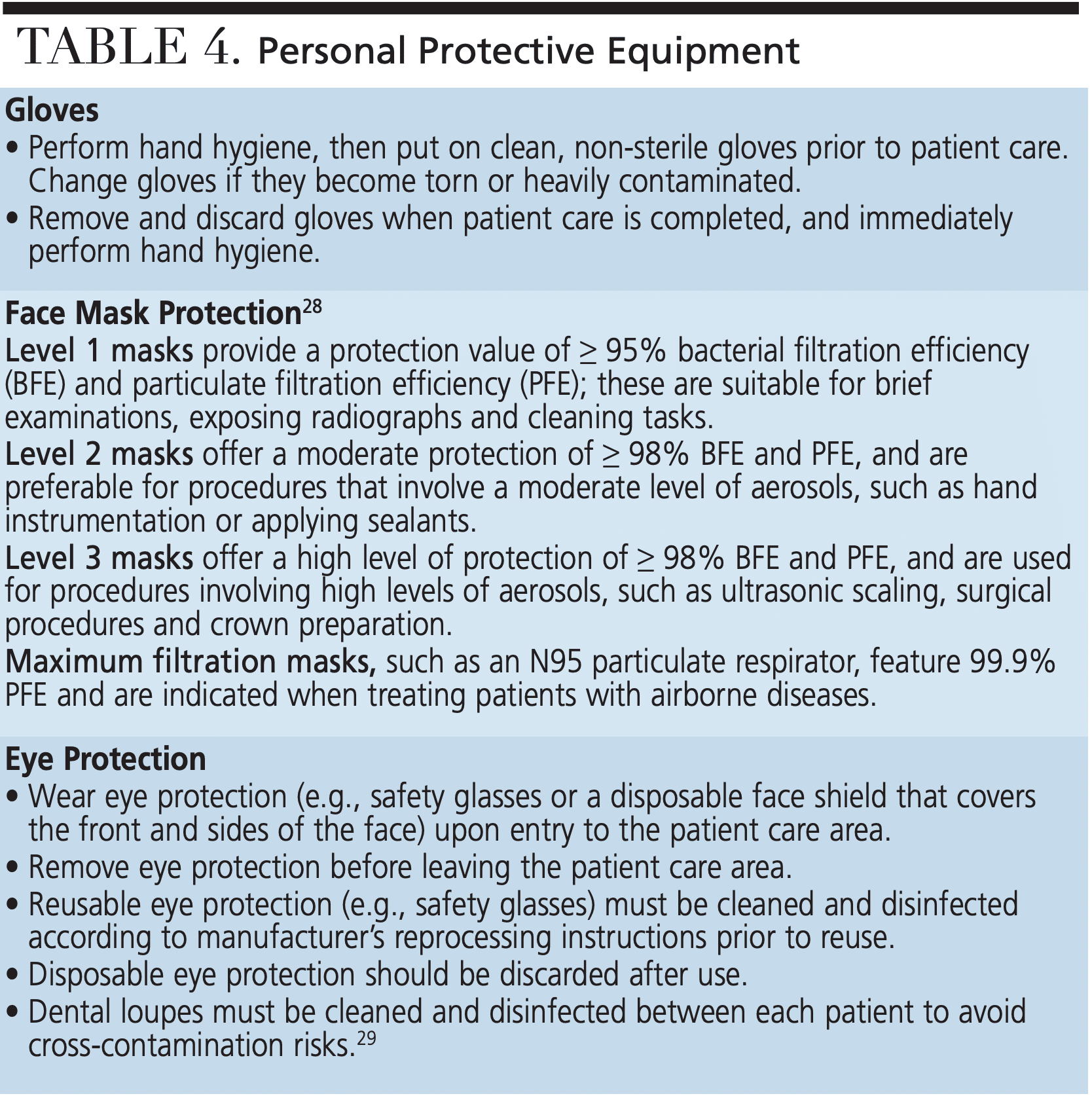
The CDC’s Guidelines for Infection Control in Dental Health-Care Settings — 2003 discuss the use of PPE to prevent potentially infectious splash, spatter and aerosols generated during rinsing, or when using handpieces and other devices (such as ultrasonic units).25 Employers should select appropriate PPE and provide it to DHCP in accordance with the Occupational Safety and Health Administration’s PPE standards (29 CFR 1910 Subpart 1).27 Dental teams must receive training and demonstrate an understanding of when to use PPE; what PPE is necessary; how to properly don, use and doff PPE to prevent self-contamination; how to properly dispose of or disinfect and maintain PPE; and the limitations of protective equipment (Table 4).28,29
Dental face masks are an important physical barrier to fluids and particulate matter and are worn during procedures that involve possible aerosols, splash or spatter.28 According to the U.S. Food and Drug Administration, a surgical face mask covers the user’s nose and mouth, and is labeled as a surgical, laser, isolation, dental or medical procedure mask (with or without a face shield).30 There are multiple levels of mask protection for DHCP, each identified according to bacterial filtration and particulate filtration efficiency levels that correspond to the demands of a given dental procedure.28 Health care and institutional settings use respirators that are at least as protective as an N95 respirator before entry into the patient care area. Oral health professionals working in facilities with high infectious disease transmission potential, such as hospitals, long-term care facilities, and dental care units located in these type of settings, may warrant use of an N95 respirator.
SUMMARY
All health care personnel need to be prepared for, and remain informed about, COVID-19, its ongoing status and updates, and preventive measures to avoid disease transmission. Oral health professionals have a responsibility to be knowledgeable about infectious diseases. Providers should also be prepared to reassure patients their clinic adheres to the highest standards of infection control. By maintaining a standard of care that is in accordance with CDC guidelines, dental teams can effectively contribute to disease prevention and help slow the coronavirus pandemic.
REFERENCES
- House of Lords Library Briefings. Parliament of the United Kingdom. Coronavirus: A Public Health Emergency. Available at: http://researchbriefings.files.parliament.uk/documents/LLN-2020-0049/LLN-2020-0049.pdf. Accessed April 6, 2020.
- Chan JF, Kok K, Zhu Z, et al. Genomic characterization of the 2019 novel human pathogenic coronavirus isolated from a patient with atypical pneumonia after visiting Wuhan. Emerg Microbes Infect. 2020;9:221–236.
- World Health Organization. Naming the Coronavirus Disease (COVID-19) and the Virus That Causes It. Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it. Accessed April 6, 2020.
- World Health Organization. Coronavirus. Available at: https://www.who.int/health-topics/coronavirus. Accessed April 6, 2020.
- World Health Organization. Coronavirus Disease 2019 (COVID-19) Outbreak. Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019. Accessed April 6, 2020.
- Bajema KL, Oster AM, McGovern OL, et al. Persons evaluated for 2019 novel coronavirus-United States. MMWR Morb Mortal Wkly Rep. 2020;69:166–170.
- COVID-19 Coronavirus Outbreak. Coronavirus Cases. Availabe at: https://www.worldometers.info/coronavirus/. Accessed April 9, 2020.
- Coronavirus Map: Tracking the Global Outbreak. Available at: https:// www.nytimes.com/interactive/2020/world/coronavirus-maps.html. Accessed April 9, 2020.
- U.S. Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19). World Map Global Map. Available at: https://www.cdc.gov/ coronavirus/2019-ncov/locations-confirmed-cases.html#map. Accessed April 9, 2020.
- U.S. Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19). Cases in U.S. Available at: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html. Accessed April 9, 2020.
- Landon E. COVID-19: What We Know So Far About the 2019 Novel Coronavirus. Available at: https://www.uchicagomedicine.org/forefront/prevention-and-screening-articles/wuhan-coronavirus. Accessed April 6, 2020.
- U.S. Centers for Disease Control and Prevention. How COVID-19 Spreads. Available at: https://www.cdc.gov/coronavirus/2019-ncov/about/transmission.html. Accessed April 6, 2020.
- Pappas S. If You Have the Coronavirus, How Long Before Symptoms Show Up? Available at: https://www.livescience.com/coronavirus-incubation-period-when-symptoms-appear.html. Accessed April 6, 2020.
- World Health Organization. Q&A on Coronaviruses (COVID-19). Available at: https://www.who.int/news-room/q-a-detail/q-a-coronaviruses. Accessed April 6, 2020.
- U.S. Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19) Symptoms. Available at: https://www.cdc.gov/coronavirus/2019-ncov/about/symptoms.html. Accessed April 6, 2020.
- U.S. Centers for Disease Control and Prevention. Information on COVID-19 and Pregnant Women and Children. Available at: https://www.cdc.gov/coronavirus/2019-ncov/specific-groups/pregnant-women-and-children.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fspecific-groups%2Fpregnant-women.html. Accessed April 6, 2020.
- U.S. Department of State, Bureau of Consular Affairs. People’s Republic of China International Travel Information. Available at: https://travel.state.gov/content/travel/en/international-travel/International-Travel-Country-Information-Pages/China.html. Accessed April 6, 2020.
- US Centers for Disease Control and Prevention. Transcript for CDC Telebriefing: Update on COVID-19, Friday, February 21, 2020. Available at: https://www.cdc.gov/media/releases/2020/t0221-cdc-telebriefing-covid-19.html. Accessed April 6, 2020.
- Qualls N, Levitt A, Kanade N, et al. Community mitigation guidelines to prevent pandemic influenza — United States, 2017. MMWR Recomm Rep. 2017;66:1–34.
- U.S. Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19) Steps to Prevent Illness. Available at: https://www.cdc.gov/coronavirus/2019-ncov/about/prevention-treatment.html. Accessed April 6, 2020.
- U.S. Centers for Disease Control and Prevention. Flowchart to Identify and Assess 2019 Novel Coronavirus. Available at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/2019-nCoV-identify-assess-flowchart-508.pdf. Accessed April 6, 2020.
- U.S. Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19) Evaluating and Reporting Persons Under Investigation (PUI). Available at: https://www.cdc.gov/coronavirus/2019-nCoV/hcp/clinical-criteria.html. Accessed April 6, 2020.
- American Dental Association. ADA develops guidance on dental emergency, nonemergency care. Available at: https://www.ada.org/en/publications/ada-news/2020-archive/march/ada-develops-guidance-on-dental-emergency-nonemergency-care. Accessed April 6, 2020.
- American Dental Hygienists’ Association. ADHA COVID-19 Updates for Dental Hygienists. Available at: https://www.adha.org/covid19. Accessed April 6, 2020.
- U.S. Centers for Disease Control and Prevention. MMWR Recommendations and Reports. Guidelines for Infection Control in Dental Health-Care Settings — 2003. Available at: https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5217a1.htm. Accessed April 6, 2020.
- Kampf G, Todt D, Pfaender S, Steinmann E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J Hosp Infect. 2020;104:246–251.
27 - U.S. Department of Labor. Occupational Safety and Health Administration. Personal Protective Equipment Standard 29 CFR 1910 Subpart 1. Available at: https://www.osha.gov/SLTC/personalprotectiveequipment/standards.html. Accessed April 6, 2020.
- Garland KV. What level of mask should dental hygienists use? Dimensions of Dental Hygiene. 2018;16(6):46
- Zwicker DH, Price RB, Carr L, Li YH. Disinfection of dental loupes: a pilot study. J Am Dent Assoc. 2019;150:689–694.
- U.S. Food and Drug Administration. N95 Respirators and Surgical Masks (Face Masks). Available at: https://www.fda.gov/medical-devices/personal-protective-equipment-infection-control/n95-respirators-and-surgical-masks-face-masks. Accessed April 6, 2020.
The authors have no commercial conflicts of interest to disclose.
From Decisions in Dentistry. April 2020;6(4):27–28,31–33.

