

Considerations for Sedation In Dentistry
As the use of minimal and moderate sedation in dental practice has grown, new models, methodologies and guidelines have emerged.
As the use of minimal and moderate sedation in dental practice has grown, new models, methodologies and guidelines have emerged
Various techniques and methods have been employed over the years to decrease the pain and anxiety associated with dental care. While the majority of dental encounters do not require pharmacologic intervention, benefits with the administration of these agents have been observed. Sedation and general anesthesia administration are historically associated with pediatric behavioral management. Indeed, 70% of board-certified pediatric dentists administer some form of sedation, and approximately 60% would hire a dentist anesthesiologist if one were available.1 Recent years have also seen an increase in adult sedation administration in general practice, with an estimated 40% of general dentists in the U.S. offering some form of sedation.2 It has been suggested that the availability of pharmacologic intervention to dental patients impacts practice marketability and revenue.2,3
In addition, in-office sedation may benefit the health care system by producing a cost-effective alternative to dental care in the operating room environment.4,5 As business models and patient expectations shift, sedation is considered a critical component of dental practice.
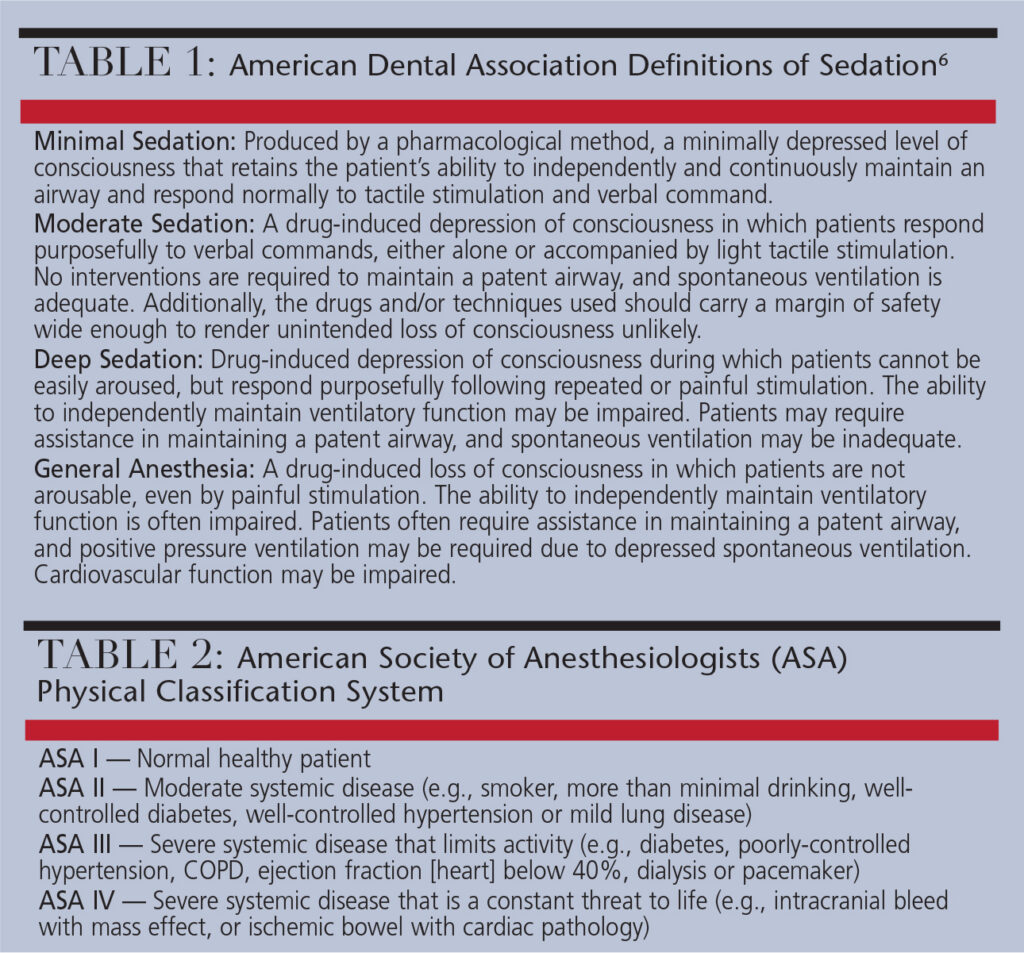
Excluding local anesthesia and analgesia, the two most common forms of pharmacologic management in dentistry are general anesthesia and sedation.4 As seen in Table 1, sedation is often divided into three modalities: minimal, moderate and deep sedation.6 Over the last 20 years, the use of minimal and moderate sedation in dental practice has grown significantly, and new models, methodologies and guidelines have emerged.
POLICY, GUIDELINES AND REGULATIONS
Sedation in dentistry has seen many variations in terms of administration, education and oversight. This fluctuation is a result of influences from individual providers and multifaceted organizations, as well as litigation processes and legislative action.7 Between 2006 and 2010, dental boards in the U.S. approved 65 sedation-related regulation changes to individual dental practice acts.7 During this period, on average, there were 13 changes each year. In comparison, from 1998 to 2005, the yearly average was less than two.
Correlation can be observed between regulatory alterations in the dental field and those occurring within overall health care. This period is associated with the growth of ambulatory surgical centers and procedural sedation,8 and a peak in the use of oral sedation for dental treatment.2 It also heralded the first Commission on Dental Accreditation and Accreditation Council for Graduate Medical Education accreditation of dental anesthesiology training programs,9 as well as new guidelines from the American Dental Association (ADA) and American Academy of Pediatric Dentistry (AAPD).10
The ADA’s and AAPD’s updated guidelines introduced definitions of levels of sedation, based on physiological parameters in place of descriptive terms, and statements utilizing route of administration (e.g., oral, rectal or intravenous, etc.) to describe anesthesia/sedation stage. The guidelines addressed sedation and general anesthesia in the office setting, and provided recommendations for hospital-based care. Through this process, patient indications for sedation were published and updated to aid practitioners in treatment planning.6,11
As seen in Table 2, the American Society of Anesthesiologists (ASA) Physical Classification System is a central part of an evaluation for sedation services. Most patients treated with conscious sedation in the dental office are categorized as ASA I or II patients.10,12 By comparison, ASA III and IV patients may have specific risks that require more focused care, and usually undergo treatment in a hospital and/or specialist environment.13
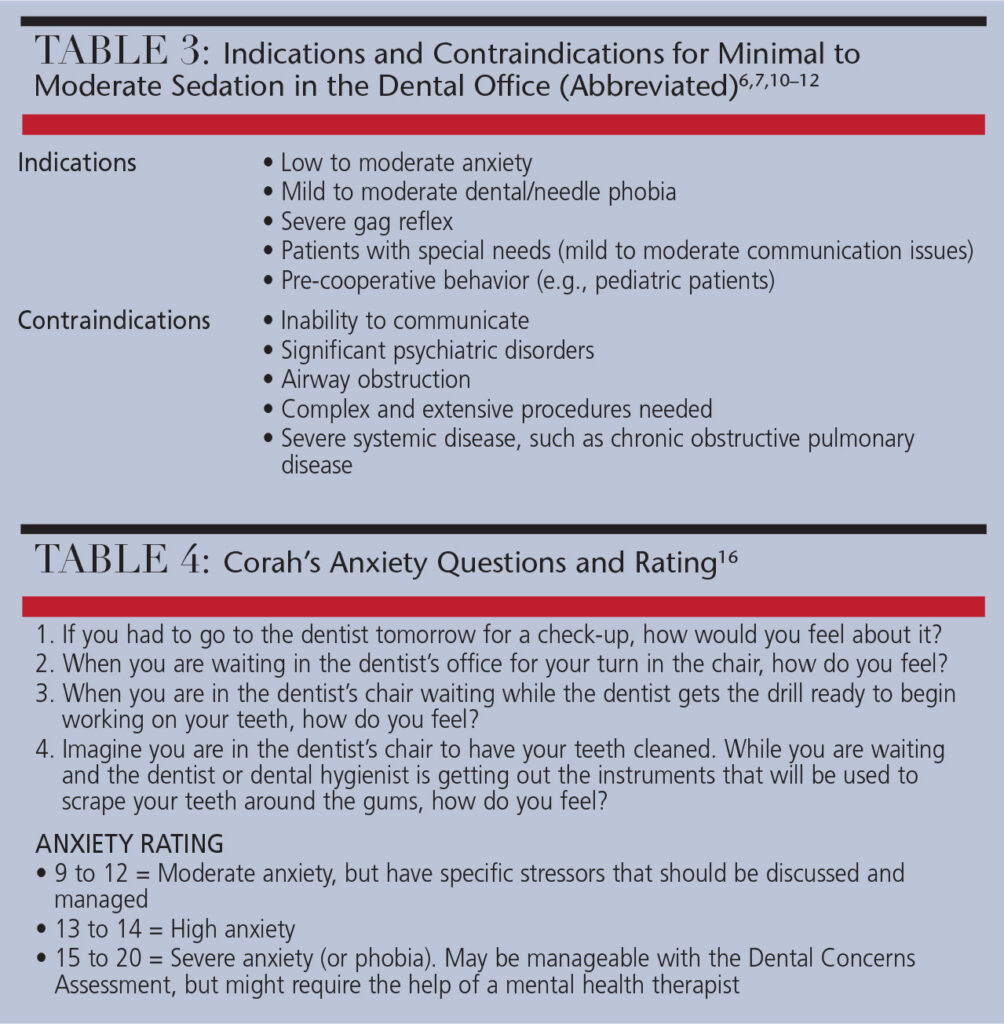
When a dental treatment plan includes sedation, patient-specific evaluations are necessary to mitigate risk. Deciding on the level of sedation or anesthesia necessary is generally based on patient characteristics, anticipated dental treatment, and provider experience.14 As seen in Table 3, proposed patient indications for sedation can be used to establish courses of treatment. Beyond indications, few tools are available to assist with treatment planning — and no consensus on the specific values of these scales has been achieved.15 In use for many years, Corah’s anxiety scale (Table 4) uses a series of four multiple-choice answers to determine a patient score. The score is then compared within three ranges: moderate, high and severe anxiety.16 Additionally, the Modified Dental Anxiety Scale is a popular scale in Europe that adds a situational platform to Corah’s scale.17 Clinicians can also use the Venham Picture Test, which has demonstrated utility by using pictures so children can self-report anxiety.18
key takeaways
- Research indicates that 70% of board-certified pediatric dentists administer some form of sedation.1 Recent years have also seen an increase in adult sedation in general practice, with an estimated 40% of general dentists offering some form of sedation.2
- This modality is typically divided into minimal, moderate and deep sedation.6
- Deciding on the level of sedation or anesthesia necessary is generally based on patient characteristics, anticipated dental treatment, and provider experience.14 In addition, patient-specific evaluations are needed to mitigate risk.
- Each treating dentist should verify the administration of sedation meets both professional standards and state practice regulations.
ROLES AND RESPONSIBILITIES
It is the responsibility of state boards of dentistry to regulate dental sedation and general anesthesia providers. Each dentist is certified to a particular level of sedation or general anesthesia, based on that dentist’s training. It is imperative to review the rules and regulations of the profession prior to providing sedation. This is an accepted modality of dentistry and, at times, a necessary tool to provide treatment. The practitioner must decide how he or she plans to address patient needs. The two pathways for consideration are outsourcing (referral to a specialist or hospital system for comprehensive care), or insourcing (independently obtaining the skill set or contracting with a third party). Ultimately, each treating dentist is responsible for the welfare of his or her patients, and should verify that the administration of sedation meets both professional standards and state practice regulations.
This responsibility remains with the treating dentist, regardless of the qualifications of a third-party contractor.7,10 Some states require dentists who provide sedation care via a contracted provider to meet specific continuing education requirements. The objective of these requirements is to have the dentist maintain a knowledge base that minimizes patient risk and provides peer accountability. It should be noted that only dentists who have completed an advanced course of education (meeting ADA standards) are qualified to administer deep sedation or general anesthesia.
PRACTICE CHARACTERISTICS
Throughout the U.S., there are regional and discipline-specific differences in the clinical practice of sedation.1,19 In an analysis of 717 U.S. dental anesthesia/sedation permit holders, oral surgery case types were most often associated with sedation services, followed by implant cases and pediatric dentistry.19 As seen in Figure 1, general dentists, endodontists and pediatric dentists were more likely to administer oral sedation, while oral and maxillofacial surgeons, dentist anesthesiologists and periodontists administered intravenous sedation most often. The majority of providers treated healthy patients, with ASA I individuals comprising 61% to 80% of respondent practitioners’ sedation schedules.19 Dentist and physician anesthesiologists were more likely to see ASA II and ASA III patients. No provider reported caring for an ASA IV patient. These findings correlate with earlier analyses, in which surveyed dentists did not desire to take on the risk of sedating medically complex individuals, due to concerns over possible litigation and/or poor outcomes.7,19,20
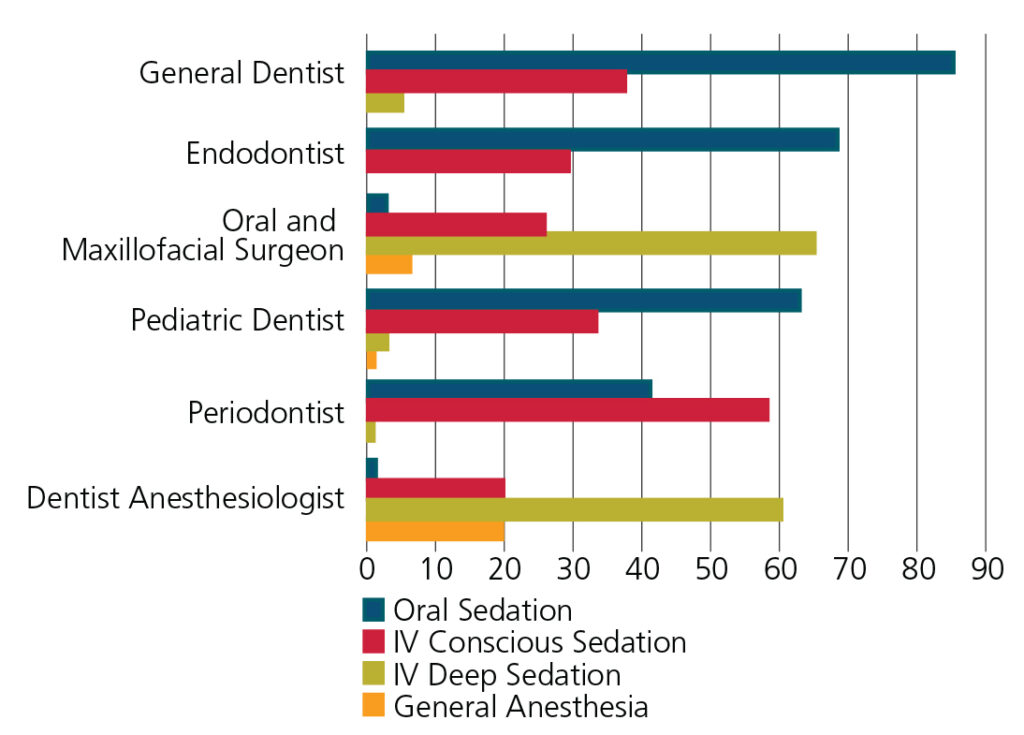
*Because the review was completed as separate categorical reports from surveyed dentists, totals of practice modalities may be more than 100%.
LOCAL ANESTHETIC AND SEDATION
Although sedation is a great tool to decrease patient anxiety, improve cooperation and provide a level of amnesia and analgesia, it does not completely eliminate the action potentials that result in pain response. Thus, the administration of a local anesthetic agent during sedation is needed for the bulk of dental treatment. Adding a buffering agent to dental anesthetic is one method of minimizing pain associated with local anesthesia. In addition, every practitioner should consider postoperative pain management, in which local anesthetic is the most common tool used to alleviate discomfort following dental care. Risks with multiple-drug administration should always be considered, however, and the patient should be continually monitored for potentially additive effects of local anesthetics with sedative agents.21
FUTURE CONSIDERATIONS
In an era of health care cost crises, opportunities to reduce the cost of care are needed.22 While cost comparisons between hospital-based anesthesia/sedation and dental office-based care are limited in literature, insights can be observed from some of the available analyses. Lee et al assessed societal costs of general anesthesia versus sedation in pediatric patients.4 The study reported that a family’s total income foregone (i.e., wages lost) due to pediatric dental treatment averaged $2698 for general anesthesia and $2203 for sedation.
A study comparing costs and time of care for ambulatory anesthesia services of healthy patients at a dental school versus a hospital was completed at Stony Brook University in New York.23 Compared to ambulatory care within a dental school, the investigators found that hospital-based care cost significantly more (13.2 times more, in fact), required more operating time (+47 minutes), and that patients spent more time in recovery (+132 minutes). While some studies show promising savings, additional research is needed to determine how demographics, patient medical status, procedure, protocols used, and provider quality/experience may influence outcomes.
A recent verdict from a U.S. District Court in Texas will likely impact sedation and general anesthesia business models.24 The court determined that dentists who do not practice one of the nine ADA specialties can advertise as specialists. In its decision, the court stated that the first amendment protected the rights of dentists who have earned credentials from bona fide credentialing boards. Dental anesthesiology is not considered one of the ADA specialties; therefore, this verdict opens up opportunities for dentist anesthesiologists to market more accurately in general, and more directly to consumers. The plaintiffs in the case included the American Academy of Implant Dentistry, American Society of Dental Anesthesiologists, American Academy of Oral Medicine, and American Academy of Orofacial Pain.
At presstime, the ADA is nearing completion of another update of its anesthesia guidelines. One proposed change is the mandatory use of capnography to monitor patients undergoing moderate and deeper levels of sedation.25 While pulse oximetry has been the standard for respiratory guidance and monitoring, it does not offer specific detail on ventilatory function.26 By providing data on carbon dioxide (CO2) levels during exhalation, the use of capnography allows earlier detection of respiratory compromise than pulse oximetry, and easier identification of hyper-/hypocapnia.26,27 That noted, concerns with the accuracy of sampling CO2 via nasal cannula have been stated by some dental professionals.27,28
Ultimately, sedation is an important component of comprehensive dental care. Growth in the use of this modality has been observed over the last two decades. While patient benefits have been reported, providers must weigh possible risks, as well. As the health care system and patient expectations evolve, our understanding of sedation and general anesthesia in dentistry will continue to mature.
REFERENCES
- Olabi NF, Jones JE, Saxen MA, et al. The use of office-based sedation and general anesthesia by board certified pediatric dentists practicing in the United States. Anesth Prog. 2012;59:12–17.
- Feck A, Silverman MD. Success with sedation: a profitability comparison of nitrous, oral, and IV sedation. Dent Economics. 2009;99:24–26.
- Jackstien J. The need and demand for anesthesia services in the United States, 2012. (Doctoral dissertation, The Ohio State University.)
- Lee JY, Vann WF, Roberts MW. A cost analysis of treating pediatric dental patients using general anesthesia versus conscious sedation. Anesth Prog. 2001;48:82–88.
- Gaulton TG, Shapiro FE, Urman RD. Administrative issues to ensure safe anesthesia care in the office-based setting. Current Opinion in Anesthesiology. 2013;26:692–697.
- American Dental Association. Guidelines for the Use of Sedation and General Anesthesia by Dentists, 2012. Available at: https://www.ada.org/~/media/ADA/About
%20the%20ADA/Files/anesthesia_use_guidelines.ashx. Accessed May 10, 2016. - Boynes SG. Dental Anesthesiology: A Guide to the Rules and Regulations of the United States of America. 5th ed. Chicago: No-No Orchard Publishing; 2011.
- Eichhorn V, Henzler D, Murphy MF. Standardizing care and monitoring for anesthesia or procedural sedation delivered outside the operating room. Current Opinion in Anesthesiology. 2010;23:494–499.
- Moore PA. Coda’s accreditation of graduate dental anesthesiology programs: a benefit to all dental education. Anesth Prog. 2008;55:71.
- Silva CC, Lavado C, Areias C, et al. Conscious sedation vs general anesthesia in pediatric dentistry — a review. Medical Express (Sao Paulo). 2015;2:M150104.
- American Academy of Pediatric Dentistry. Policy on use of deep sedation and general anesthesia in pediatric dental office. Pediatr Dent. 2008-2009;30(7Suppl):66:7.
- Boynes SG, Lewis CL, Moore PA, et al. Complications associated with anesthesia administered for dental treatment. Gen Dent. 2009;58:e20–25.
- Sury M. Sedation of children — perspectives across hospital specialties. SAAD Dig. 2013;29:60–63.
- Williams APF, Moles PJ. Sedation versus general anaesthesia for provision of dental treatment to patients younger than 18 years (Review). The Cochrane Library. 2015:9.
- Hunt O, McCurley N, Dempster M, et al. Patient anxiety and IV sedation in Northern Ireland. Br Dent J. 2011;210:55–57.
- Corah NL. Assessment of a dental anxiety scale. J Am Dent Assoc. 1978;97:816–819.
- Humphris GM, Freeman R, Campbell J, et al. Further evidence for the reliability and validity of the Modified Dental Anxiety Scale. Int J Dent. 2000;50:367–370.
- Venham LL, Gaulin-Kremer E. A self-report measure of situational anxiety for young children. Pediatr Dent. 1979;1:91–96.
- Boynes SG, Moore PA, Tan PM, et al. Practice characteristics among dental anesthesia providers in the United States. Anesth Prog. 2010;57:52–58.
- Adams AC. Access to deep sedation and general anaesthesia services for dental patients: A survey of Ontario dentists, 2015. (Doctoral dissertation, University of Toronto.)
- Dionne RA, Yagiela JA, Cote CJ, et al. Balancing efficacy and safety in the use of oral sedation in dental outpatients. J Am Dent Assoc. 2006;137:502–513.
- Kaplan RS and Porter ME. How to solve the cost crisis in health care. Harv Bus Rev. 2011;89:46–52.
- Rashewsky S, Parameswaran A, Sloane C, et al. Time and cost analysis: pediatric dental rehabilitation with general anesthesia in the office and the hospital settings. Anesth Prog. 2012;59:147–153.
- ADA News. Texas court ruling allows non-ADA recognized specialty dentists to advertise as specialists. February 1, 2016.
- American Dental Association Council on Dental Education and Licensure. Proposed revisions [anesthesia and sedation]. Available at: http://www.ada.org
/~/media/ADA/Education%20and%20Careers/Files/proposed_revisions-sedation_anesthesia_guidelines-2014.ashx. Accessed May 10, 2016. - McCarthy C, Brady P, O’Halloran KD, et al. Tetany during intravenous conscious sedation in dentistry resulting from hyperventilation induced hypocapnia. Anesth Prog. 2016;63:25–30.
- Iwasaki J, Vann Jr WF, Dilley DC, Anderson JA. An investigation of capnography and pulse oximetry as monitors of pediatric patients sedated for dental treatment. Pediatr Dent. 1989;11:111–117.
- Primosch RE, Buzzi IM, Jerrell G. Monitoring pediatric dental patients with nasal mask capnography. Pediatr Dent. 2000;22:120–124.
