

Clinical Decisions When Using Universal Adhesives
A review of the scenarios encountered with the use of these agents, and the evidence supporting a case-appropriate choice.
A review of the scenarios encountered with the use of these agents, and the evidence supporting a case-appropriate choice
Recently, manufacturers have introduced single-bottle adhesive systems that can be used in self-etch and total-etch modes. Commonly referred to as universal adhesives, these products can pose potentially confusing scenarios in daily practice; consequently, this article will examine evidence that will help support appropriate clinical decision-making.
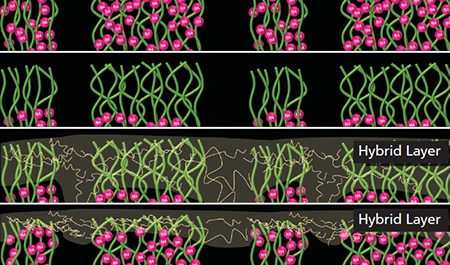
Current techniques used for bonding to tooth structure are the result of incremental scientific discoveries.1 In the 1950s, the work of Buonocore et al2 demonstrated that acid etching tooth structure prior to the application of an adhesive improved the bond to enamel by removing the smear layer and dissolving hydroxyapatite mineral, thereby creating surface texture that aided retention. It was not until the 1980s that Nakabayashi et al3 reported the concept of a hybrid layer. This discovery demonstrated that an effective bond could be formed to dentin by infiltrating resin into demineralized collagen fibrils (Figure 1). As a result, total-etching enamel and dentin gained clinical acceptance. In the 1990s, Kanca4 popularized the “wet bonding” technique, which is based on the premise that bonding to dentin is best achieved when the dentin is left moist in order to prevent desiccation of the demineralized dentin layer. The residual wetness of the dentin, however, required a balance between dentin that was “too wet” (with residual water separating components of the adhesive), and dentin that was “too dry” (leading to collapse of collagen fibrils).5
The technique sensitivity attributed to residual dentin wetness is avoided with the use of self-etching adhesives. These products employ acidic resin monomers that are capable of partially or completely dissolving the smear layer, demineralizing collagen, and bonding to calcium in tooth structure. Self-etching avoids the possibility of desiccating collagen fibrils, as the collagen fibrils are demineralized and infiltrated with resin in the same clinical step. Another proposed advantage of self-etch adhesives is they lead to less postoperative sensitivity, as they do not require application of phosphoric acid on dentin. Most clinical studies, however, report no difference in postoperative sensitivity with total-etch or self-etch adhesives.6
Total-etch and self-etch adhesives have both been offered in one-bottle and two-bottle systems. Generally, the first step in two-bottle systems employs the hydrophilic monomer hydroxylethyl methacrylate (HEMA) containing a primer that penetrates the water-rich dentin prior to application of a more hydrophobic layer of resin adhesive. Single-bottle adhesives combine HEMA into the adhesive, leading to a single, more hydrophilic adhesive layer. Hydrophilicity is beneficial in the short term, as it allows infiltration into dentin. That noted, the long-term disadvantage of a hydrophilic adhesive layer is that it will attract water from dentinal tubules, leading to hydrolytic degradation of the bond.7 Clinically, most single-bottle total-etch and self-etch systems have lower reported clinical success than two-bottle systems that have a separate hydrophobic bonding agent.8
DISTINCT FORMULATIONS
The recently introduced single-bottle universal adhesive systems that can be used in self-etch and total-etch modes feature formulations that differentiate these agents from previous single-bottle self-etching or total-etching adhesives. The acidic monomer 10-methacryloyloxydecyl dihydrogen phosphate (10-MDP), which had been used by one self-etching adhesive system for years, was added to many other materials when the patent expired.9 This 10-MDP monomer has been shown to form a more effective and stable bond to tooth structure than the acidic monomers used previously, such as 4-methacryloxyethyl trimellitic acid (4-MET) and 2-methacryloxyethyl phenyl hydrogen phosphate (Phenyl-P).10 Additionally, 10-MDP has a relatively long carbon chain (alkylene group) to maintain a balance between hydrophobic and hydrophilic properties, which may improve long-term bond stability.11 Manufacturers have also made claims that universal adhesives can be used as primers for ceramic restorations, and that some are compatible with dual-cure and self-cure buildups and cements. The foregoing has led to confusion in some operatories as to the appropriate use of these materials; thus the need to examine the evidence that will support clinical decision-making.
Should dentin and/or enamel be etched with phosphoric acid prior to bonding?
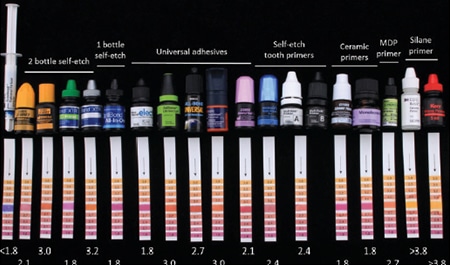
Although manufacturers state that universal adhesives can be used in a self-etch or total-etch mode, a conscientious clinician would want to know which mode will provide a stronger and longer-lasting bond. Laboratory research studies involving several universal adhesives have reported superior bond strength to enamel when it is etched with phosphoric acid.12,13 In comparison to previous self-etch adhesives, the poor performance of universal adhesives in bonding to enamel in a self-etch mode is likely due to the higher pH of universal adhesives (Figure 2). Because they are less acidic, they cannot provide the surface roughness needed for bonding to enamel. Some improvement in the bond to enamel in the self-etch mode was reported when the adhesive was vigorously scrubbed into the enamel.14 Laboratory data does not provide conclusive evidence for which mode performs better with dentin. A selective enamel etching technique has been proposed in which the phosphoric acid is only applied to enamel, and rinsed off without etching dentin.
Two randomized controlled clinical studies evaluated a universal adhesive used with different etching modes. One showed similar performance of the material using total-etch and selective-etch techniques, but inferior performance with the self-etch technique.15 The other study (in which two of the authors served as investigators) reported better marginal adaptation when the adhesive was used in a total-etch mode, rather than a self-etch mode.16
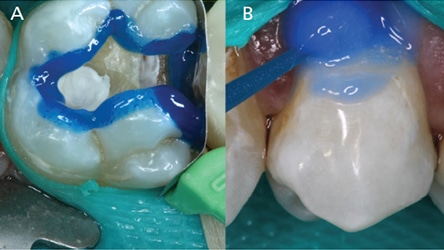
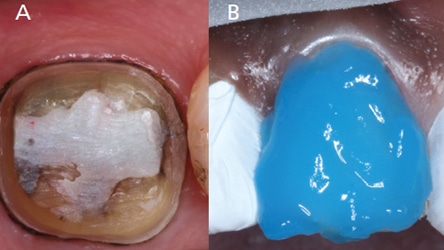
Based on the laboratory and clinical studies, etching enamel with phosphoric acid prior to application of a universal adhesive will provide a more reliable bond. The authors recommend a total- or selective-etch technique for routine direct restorations involving enamel and dentin (Figures 3A and 3B). For cases involving predominantly dentin, such as crown preparations, a self-etch technique may be used (Figures 4A and 4B). For cases involving predominantly enamel, such as veneers or diastema closures, phosphoric acid etching is compulsory (Figures 4A and 4B). A total-etch technique would also be preferred for bonding to sclerotic dentin (Figures 3A and 3B).
Should a universal adhesive be used with a self- or dual-cured buildup or cement?
Although universal adhesives are typically on the higher end of the pH spectrum of self-etching adhesives, they are still relatively acidic (Figure 2). A common problem of any one-step self-etching adhesive is they will leave an acidic surface following application to tooth structure. This acidic surface will interfere with the amine-based chemical reaction used to cure self-cured or dual-cured resins.17 In other words, application of an acidic universal adhesive to tooth structure can prevent curing of a self-cured resin cement or buildup material placed on top of it. In some cases, this may cause debonding of a buildup, post or fixed restoration.
There are two methods to avoid this possible failure. The first is to use a dual-cure activator with the universal adhesive. This activator is typically sold with the universal adhesive and can be mixed in a 1:1 ratio with the adhesive. It contains arylsulfinate salts that will make the adhesives compatible with dual-cure and self-cure resin cements.18 However, it will not make the adhesive itself dual cure. Some universal adhesives are reported to have a high enough pH that the dual-cure activator is not needed. The second method is to use amine-free buildup materials and cements, which are unaffected by the acidity of the adhesives. Manufacturers have specific recommendations for the use of universal adhesives with self-cure or dual-cure materials that must be followed.
Should the adhesive be light cured prior to using a resin cement?
When universal adhesives are used as tooth primers with resin cements, the clinician must choose whether to light cure the adhesive prior to cementing the fixed restoration. For some products, manufacturers recommend light curing the adhesive prior to applying the cement. In this case, it is important to air thin the adhesive prior to light curing in order to prevent a thick adhesive film that would prevent complete crown seating. Some materials do not require light curing of the adhesive, as there is a chemical initiator for the adhesive in its corresponding cement that chemically cures the adhesive upon contact with the cement. However, a laboratory study reported higher bond strength for an adhesive when the optional light cure was performed prior to cementation than when the chemical-contact cure acted alone.19 In the case of post cementation, chemical initiation of the adhesive by contact with the cement is beneficial, as light curing the adhesive in the post space is difficult due to physical constraints. In addition, it can potentially prevent complete seating of the post.
Should a universal adhesive be used as a primer when bonding to zirconia?
Another advantage of adding 10-MDP to universal adhesives is that this monomer can also bond to zirconia. In fact, it is the monomer used in most primers indicated for bonding to zirconia. Laboratory studies have shown that some universal adhesives are effective primers for bonding to zirconia (Figure 5).20,21 Not all manufacturers recommend using their universal adhesive as a zirconia primer, however. Some universal adhesives do not use the monomer 10-MDP, consequently, they should not be used as a zirconia primer.

restorations.
Should a universal adhesive be used as a primer for glass-based ceramics?
Some universals adhesives have added silane, the molecule used as a primer for glass-based ceramics, such as lithium disilicate or porcelain. Bond strength testing has shown these universal adhesives are not the best primers for lithium disilicate.22 Either the acidity of the adhesive or interactions with the other monomers in the adhesive render the silane ineffective. When bonding to glass ceramics, a separate silane primer is recommended after hydrofluoric acid etching.
How do the handling properties of different universal adhesives compare?
Slight differences in composition of various universal adhesives can affect their handling properties. For example, some universal adhesives are dispensed as a thick liquid, whereas others are dispensed as a thin clear liquid (Figure 6). One difference is that some contain an ethanol solvent, while others contain an acetone solvent. The authors evaporated the solvents from two adhesive products, and the one with the thicker consistency contained around 70-weight-percent residual filler and monomer, whereas the thinner adhesive contained around 40%. This information is relevant to the clinician, as a laboratory study reported that an adhesive with a thinner consistency required two coats of adhesive to achieve its highest bond strength, whereas the more viscous adhesive achieved its highest bond strength with a single coat.23 On the other hand, low-viscosity adhesives may be beneficial if the clinician chooses to light cure the adhesive under an indirect restoration. In this case, a low-viscosity adhesive would be less likely to result in a thick film that prevented complete seating of the restoration.

others are less viscous or “thin” (right).
If the clinician chooses to perform a selective-etch technique, the handling properties of the phosphoric acid can also affect the success of the procedure. Some phosphoric acids are more viscous and can be applied to the enamel only; other formulations of phosphoric acid are runnier, which is beneficial for a total-etch technique (Figure 7).

the left) are advantageous for the selective-etch technique, whereas less
viscous etchants (e.g., the two on the right) are advantageous when
using the total-etch technique.
SUMMARY
There are several generalizations that apply for universal adhesives. Enamel should be etched with phosphoric acid prior to application of a universal adhesive. A dual-cure activator should be mixed with the universal adhesive if it is to be used in combination with an amine-containing cement or buildup material The highest bonds are achieved if the universal adhesive is light cured prior to cementation of a fixed restoration, however, the adhesive should be adequately thinned prior to curing. While universal adhesives containing 10-MDP can be effective primers for zirconia, they are not the most effective primers for glass-based ceramics. Thicker adhesives can be applied in a single coat for direct restoration, and thinner adhesives may produce a thinner film under indirect restorations.
As the foregoing discussion demonstrates, operators who keep abreast of the literature are in the best position to make sound, evidence-based decisions regarding the use of universal adhesives.
KEY TAKEAWAYS
- Single-bottle universal adhesive systems that can be used in self-etch and total-etch modes are formulated differently than previous single-bottle self-etch or total-etch adhesives.
- A proposed advantage of self-etch adhesives is they lead to less postoperative sensitivity, as they do not require application of phosphoric acid on dentin. Most clinical studies, however, report no difference in postoperative sensitivity with total-etch or self-etch adhesives.6
- Clinically, most single-bottle total-etch and self-etch systems have lower reported clinical success than two-bottle systems that have a separate hydrophobic bonding agent.8
- Laboratory studies involving several universal adhesives have reported superior bond strength to enamel when it is etched with phosphoric acid.12,13
- Application of an acidic universal adhesive to tooth structure can prevent curing of a self-cured resin cement or buildup material placed on top of it.
- The highest bonds are achieved if the universal adhesive is light cured prior to cementation of a fixed restoration; however, the adhesive should be adequately thinned prior to curing.
- Thicker universal adhesives can be applied in a single coat for direct restorations, while thinner adhesives will produce a thinner film under indirect restorations.
REFERENCES
- Pashley DH. The evolution of dentin bonding. Dent Today. 2003;22: 112–114,116,118–119.
- Buonocore MG. A simple method of increasing the adhesion of acrylic filling materials to enamel surfaces. J Dent Res. 1955;34:849–853.
- Nakabayashi N, Kojima K, Masuhara E. The promotion of adhesion by the infiltration of monomers into tooth substrates. J Biomed Mater Res. 1982;16:265–273.
- Kanca J 3rd. Improved bond strength through acid etching of dentin and bonding to wet dentin surfaces. J Am Dent Assoc. 1992;123:35–43.
- Tay FR, Gwinnett AJ, Wei SH. Micromorphological spectrum from overdrying to overwetting acid-conditioned dentin in water-free, acetone based, single-bottle primers/adhesives. Dent Mater. 1996;12:236–244.
- Reis A, Dourado Loguercio A, Schroeder M, Luque-Martinez I, Masterson D, Cople Maia L. Does the adhesive strategy influence the post-operative sensitivity in adult patients with posterior resin composite restorations? A systematic review and meta-analysis. Dent Mater. 2015;31:1052–1067.
- Tay FR, Pashley DH. Water treeing-a potential mechanism for degradation of dentin adhesives. Am J Dent. 2003;16:6–12.
- Peumans M, De Munck J, Mine A, Van Meerbeek B. Clinical effectiveness of contemporary adhesives for the restoration of non-carious cervical lesions. A systematic review. Dent Mater. 2014;30:1089–1103.
- Alex G. Universal adhesives: the next evolution in adhesive dentistry? Compend Contin Educ Dent. 2015;36:15–26.
- Yoshida Y, Inoue S. Chemical analyses in dental adhesive technology. Jap Dent Sci Rev. 2012;48:141–152.
- Suh BI. Principles of Adhesive Dentistry: A Theoretical and Clinical Guide for Dentists. Newtown, Pa: Aegis Publications LLC; 2013.
- de Goes MF, Shinohara MS, Freitas MS. Performance of a new one-step multi-mode adhesive on etched vs non-etched enamel on bond strength and interfacial morphology. J Adhes Dent. 2014;16:243–250.
- Takamizawa T, Barkmeier WW, Tsujimoto A, et al. Influence of pre-etching times on fatigue strength of self-etch adhesives to enamel. J Adhes Dent. 2016;18:501–511.
- Cardenas AM, Siqueira F, Rocha J, et al. Influence of conditioning time of universal adhesives on adhesive properties and enamel-etching pattern. Oper Dent. 2016;41:481–490.
- Lawson NC, Robles A, Fu CC, Lin CP, Sawlani K, Burgess JO. Two-year clinical trial of a universal adhesive in total-etch and self-etch mode in non-carious cervical lesions. J Dent. 2015;43:1229–1234.
- Loguercio AD, de Paula EA, Hass V, Luque-Martinez I, Reis A, Perdigão J. A new universal simplified adhesive: 36-month randomized double-blind clinical trial. J Dent. 2015;43:1083–1092.
- Suh BI, Feng L, Pashley DH, Tay FR. Factors contributing to the incompatibility between simplified-step adhesives and chemically-cured or dual-cured composites. Part III. Effect of acidic resin monomers. J Adhes Dent. 2003;5:267–282.
- Gutiérrez MF, Sutil E, Malaquias P, et al. Effect of self-curing activators and curing protocols on adhesive properties of universal adhesives bonded to dual-cured composites. Dent Mater. 2017;33:775–787.
- Lührs AK, Pongprueksa P, De Munck J, Geurtsen W, Van Meerbeek B. Curing mode affects bond strength of adhesively luted composite CAD/CAM restorations to dentin. Dent Mater. 2014 ;30:281–291.
- Zhao L, Jian YT, Wang XD, Zhao K. Bond strength of primer/cement systems to zirconia subjected to artificial aging. J Prosthet Dent. 2016 Nov;116:790–796.
- Passia N, Mitsias M, Lehmann F, Kern M. Bond strength of a new generation of universal bonding systems to zirconia ceramic. J Mech Behav Biomed Mater. 2016;62:268–274.
- Passia N, Lehmann F, Freitag-Wolf S, Kern M. Tensile bond strength of different universal adhesive systems to lithium disilicate ceramic. J Am Dent Assoc. 2015;146:729–734.
- Chang BJ, Lawson NC, Burgess JO. Effect of adhesive coats and solvents on bond strength. J Dent Res. 2015;94(Spec Issue A):3385.
The authors have no commercial conflicts of interest to disclose.
Featured Image by Monty Rakusen / Cultur / Getty Images Plus
From Decisions in Dentistry. November 2017;3(11):24–28.
