

Clinical Applications: Cone Beam Computed Tomography in Dentistry
An overview of the application and interpretation of three-dimensional radiographic imaging by dental providers
An overview of the application and interpretation of three-dimensional radiographic imaging by dental providers
EDITOR’S NOTE:
The diagnostic utility of cone beam computed tomography is making this imaging modality an increasingly common part of general and specialty oral health care. Due to the nature of this clinical overview, this article has not undergone peer review.
‘The delivery of health care has proceeded for decades with a blind spot: Diagnostic errors — inaccurate or delayed diagnoses — persist throughout all settings of care and continue to harm an unacceptable number of patients. Despite the pervasiveness of diagnostic errors and risk for serious patient harm, these errors have been largely unappreciated within the quality and patient safety movements in health care. Without a dedicated focus on improving diagnosis, these errors will likely worsen as the delivery of health care and the diagnostic process continue to increase in complexity.”1 This passage from Improving Diagnosis in Health Care, a report from the National Academies of Sciences, Engineering and Medicine, underscores the notion that oral and maxillofacial radiology is both an art and a science. Art is defined as a skill acquired by experience, study or observation, while science is a technique that is tested through scientific methods.
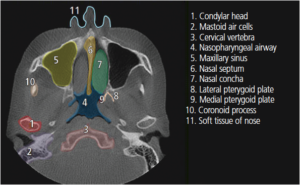
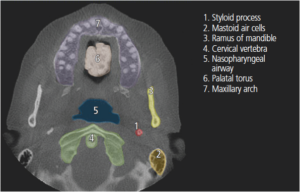
In terms of dental diagnoses, the science of dental radiology requires sophisticated equipment to produce an X-ray image, while the principles of geometry allow the acquisition of accurate images with minimal distortion (e.g., use of the paralleling technique). Once an image has been produced, the art of dental radiology comes into play. Accurate interpretation of a dental radiograph involves the application of the observer’s knowledge, cognitive skills and accumulated experience. This article will describe basic applications for cone beam computed tomography (CBCT), and highlight basic anatomical landmarks found on different planes in CBCT images (Figure 1 through Figure 4, pages 28 and 31).2 This understanding will help reduce unnecessary exposure to patients, while improving the diagnostic information available to clinicians.2

DENTAL IMPLANTS
Implants have become ubiquitous for tooth replacement, and CBCT scans offer implantologists and restorative dentists invaluable pre- and postsurgical information. Some of the benefits include accurate localization of the inferior alveolar canal, cross-sectional visualization of the contours of the alveolar ridge, and the ability to accurately measure the height and width of the alveolus. Additionally, use of presurgical treatment planning software and fabrication of a surgical guide provide critical information for assessing proper site selection and implant placement.
OSSEOUS PATHOLOGY
Three-dimensional (3D) CBCT views of osseous pathology can greatly assist treatment planning, particularly when oral surgery may be involved. For example, bucco-lingual expansion of the mandibular ramus may be assessed from a CBCT scan, which would be impossible to accurately view on a conventional two-dimensional (2D) panoramic image. Localization of anomalies, such as a sialolith or Stafne bone cyst, can easily be diagnosed on sagittal and axial CBCT views.

TEMPOROMANDIBULAR JOINT DISORDERS
Temporomandibular joint disorders may be related to osseous changes in the temporomandibular joint. Whereas visualization of these changes was often impossible with prior imaging techniques, CBCT scans of the temporomandibular joint will help reveal degenerative and neoplastic changes in the region. Combining the CBCT scan with 3D reconstruction imaging software allows the practitioner to more precisely evaluate condylar changes. However, a clinician must also consider that actual patient treatment for these osseous changes may not be altered simply with better imaging.
IMPACTIONS
In impaction cases, 3D CBCT images that reveal tooth-to-tooth and tooth-to-anatomic structure relationships can be extremely helpful in treatment planning and therapy. While clinicians performing a routine dental extraction may not benefit from a CBCT scan, such imaging could be beneficial for localizing impacted teeth. For example, extractions of impacted mandibular third molars often are complicated by their proximity to the inferior alveolar canal. Relying on a conventional 2D panoramic image or intraoral periapical image may inadequately relate the impacted tooth to the canal. Cross-sectional views will more accurately relate the position of the two objects to one another. In addition, the clinician will obtain supplemental information as to whether a buccal or lingual approach would allow best access to the tooth.
ORTHODONTICS
Use of CBCT imaging can supplement cephalographic and panoramic images for orthodontic treatment planning, but it should not be standard protocol for all patients. A CBCT scan is particularly useful when it may be impossible for a clinician to visualize the positional relationships of unerupted teeth using traditional 2D images. Multiplanar images from CBCT scans will supply much more detailed relational information that clinicians will find critical for treatment success.
ENDODONTICS
In endodontics, CBCT imaging is useful for locating accessory canals, fractures and localization of apical pathology. For example, a periapical image may reveal a radiolucent lesion that appears to envelope multiple roots — however, a cross-sectional image may reveal the radiolucency is actually attached to only a single root, which would alter the treatment plan. The application of a CBCT unit designed to image a single quadrant with a small field of view (e.g., 5 centimeters) is ideally suited for endodontic procedures. Compared to other scans, it will reduce overall scatter radiation and expose the patient to significantly less radiation.
CONCLUSION
While reduced radiation exposure from CBCT versus medical computed tomography is a plus, it is important to realize CBCT scanning results in significantly more radiation exposure than conventional dental imaging. Consequently, CBCT scans should only be taken when traditional imaging is inadequate to assess a patient’s oral health or treatment outcome.2 Fortunately, when considering the multitude of applications for advanced 3D imaging, oral health professionals can consult any number of clinical guidelines designed to support the judicious use of CBCT scanning.

KEY TAKEAWAYS
- Three-dimensional cone beam computed tomography (CBCT) offers implantologists invaluable pre- and postsurgical information, including accurate localization of the inferior alveolar canal, cross-sectional visualization of the contours of the alveolar ridge, and the ability to accurately measure the height and width of the alveolus.
- Cone beam scans of the temporomandibular joint will help reveal degenerative and neoplastic changes in the region, thus aiding diagnosis and treatment planning.
- In impaction cases, CBCT images can reveal tooth-to-tooth and tooth-to-anatomic structure relationships that will be helpful in case presentations and therapy.
- Use of CBCT imaging can supplement cephalographic and panoramic images for orthodontic treatment planning, but it should not be standard protocol for all patients.
- The application of a CBCT unit designed to image a single quadrant with a small field of view (e.g., 5 centimeters) is ideally suited for endodontic procedures.
- Because CBCT imaging results in significantly more radiation exposure than two-dimensional radiographs, CBCT scans should only be taken when traditional imaging is inadequate to assess a patient’s oral health or treatment outcome.2
Guidelines for Cone Beam Imaging
Here is a partial list of professional guidelines available to assist clinicians who are considering cone beam computed tomography.
- U.S. Food and Drug Administration — Dental Cone Beam Computed Tomography, fda.gov/Radiation-Emitting Products/RadiationEmittingProductsandProcedures/MedicalImaging/MedicalX-Rays/ucm315011.htm
- Information for Dental Professionals, fda.gov/Radiation-EmittingProducts/RadiationEmittingProductsandProcedures/MedicalImaging/MedicalX-Rays/ucm315011.htm#professionals
- American College of Radiology, Radiological Society of North America, American Society of Radiologic Technologists, and the American Association of Physicists in Medicine — Image Wisely, radiologyinfo.org/en/downloads/index.cfm#resource-ImageWisely
- Alliance for Radiation Safety in Pediatric Imaging — Image Gently, radiologyinfo.org/en/downloads/index.cfm#resource-ImageGently
- American Dental Association Council on Scientific Affairs and U.S. Food and Drug Administration — Dental Radiographic Examinations Recommendations for Patient Selection and Limiting Radiation Exposure, ada.org/en/~/media/ADA/Publications/ADANews/Files/Dental_Radiographic_Examinations_2012
- American Association of Endodontists and American Academy of Oral and Maxillofacial Radiology Joint Position Statement — Use of Cone Beam Computed Tomography in Endodontics, aae.org/ uploaded files/clinical_ resources/ guidelines_and_position statements/cbct statement_2015update.pdf American Academy of Oral and Maxillofacial Radiology — Position statement of the American Academy of Oral and Maxillofacial Radiology on selection criteria for the use of radiology in dental implantology, with an emphasis on cone beam computed tomography, ncbi.nlm.nih.gov/pubmed/22668710
- Radiological Society of North America’s and the American College of Radiology — Patient information, radiologyinfo.org/en/info.cfm?pg=dentalconect
REFERENCES
- National Academies of Sciences, Engineering, and Medicine. 2015. Improving Diagnosis in Health Care. Available at: nationalacademies.org/hmd/Reports/2015/Improving-Diagnosis-in-Healthcare.aspx. Accessed November 27, 2017.
- Hubar JS. Fundamentals of Oral and Maxillofacial Radiology. Hoboken, NJ: Wiley Blackwell; 2017.
The authors have no commercial conflicts of interest to disclose.
FEATURED IMAGE:CASH14/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. January 2018;4(1):26-28,31.
