

Behavior and Caries Management in Pediatric Dentistry
An examination of management techniques and variables that impact clinical decision-making in pediatric dentistry.
PURCHASE COURSE
This course was published in the October 2019 issue and expires October 2022. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the October 2019 issue and expires October 2022. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss modern strategies for disease and behavior management in pediatric dentistry.
- List various approaches to caries risk assessment and treatment planning when caring for this patient population.
- Explain the dynamic nature of the caries process, and the variables that affect the intersection between disease and behavior management in pediatric oral health care.
Behavior management is a cornerstone of treatment planning in pediatric dentistry. A child’s level of cooperation and ability to follow instructions from the dental team directly influence how well a restorative or surgical procedure can be performed and even what materials can be used. It is the clinician’s responsibility to safely and effectively guide the child’s behavior during all pediatric procedures. Conventional communication techniques should be employed at all times and might include demonstration via the tell-show-do approach, setting clear expectations for the child at each visit, and positive reinforcement.1 While these techniques work well for most children, when a child’s behavior or ability to cooperate is less than ideal, dentists must adapt their treatment to account for behavior management. Many pre-cooperative and highly anxious or fearful children require more advanced or invasive methods of behavior management, including pharmacological techniques, such as procedural sedation and general anesthesia.1
Pharmacologic behavior management introduces a new level of risk, which can be obviated by appropriately trained providers paying careful attention to preoperative assessment, emergency preparedness, intraoperative monitoring and postoperative evaluation.2,3 In light of new approaches to risk assessment, changing disease patterns, and the emphasis on nonsurgical management in pediatric dentistry, the amount of information influencing clinical decisions is greater than ever. This article will attempt to categorize the variables and pose a framework to navigate clinical decision-making at the intersection of behavior and disease management in pediatric dentistry.
Early childhood caries (ECC) is an age-defined diagnosis of caries in the primary dentition in children less than 6 years old.4 Even though its incidence and associated disparities have decreased,5 ECC still conveys considerable public health and financial burden for many families.6,7 Severe cases often require general anesthesia, with costs approaching $25,000 or more.6 Due to the complexity of the disease and factors affecting its presence (or absence), prevention is rarely as simple as practicing good oral hygiene or having frequent fluoride exposure.
One of the most widely used conceptual models for defining and diagnosing ECC illustrates its multiple levels of influence.8 Genetic predisposition, the oral microbiome, and individual health behaviors may be specific to a particular child, but the surrounding environment — including family and social supports, access to quality foods, or access to health care — also has a major influence on ECC and oral health disparities. More importantly, the model recognizes the time dynamic to the caries process, which complicates risk assessment and prognosis, as these will change as the balance of protective and risk factors ebbs and flows with time.8
Despite the availability of multiple caries risk assessment tools for pediatric patients, caries risk assessment remains an inexact science that is difficult to validate.9–13 Recently, Divaris14 identified deficiencies of the current models of caries risk assessment, calling into question two main issues: risk being a population parameter assigned to individuals, and the level at which ECC is diagnosed. First, ECC risk factors at the population level (i.e., groups) fail to translate to the individual level (i.e., a single person).15 For example, it is not uncommon to find patients who follow excellent preventive regimens, yet still experience disease. Conversely, some patients have highly cariogenic diets, poor hygiene and practice no preventive therapy, yet remain disease free.
When assigning risk, a dentist’s subjective assessment, intuition, and local context often serve as risk assessment tools.16 Without local context, however, such subjectivity renders the interpretation of caries risk across providers and other interested parties meaningless.14 In addition, clinical training frequently emphasizes diagnosis and treatment planning at the tooth and surface level (i.e., individual teeth and tooth surfaces). However, as currently defined, ECC is a person-level disease requiring person-level treatment. This distinction is important and forms the basis for this paper. Safe and compassionate treatment that can improve the oral health trajectory of a child, not a tooth, is the ultimate goal.
DISEASE MANAGEMENT
Surgical Treatment: Managing ECC traditionally includes surgical care via a combination of restorative, endodontic and surgical treatment, as indicated by clinical guidelines. Decision-making about restoration timing following caries diagnosis typically depends on clinical criteria of visible cavitation, clinical shadowing, or radiographic progression of a lesion into dentin.17–19 Only recently has caries risk entered the decision-making process,12 and even more recently dentists have acknowledged the disease process is dynamic — meaning it can progress or regress, depending on intraoral conditions.20 Since it is difficult to clinically determine caries activity at a single time point, active prevention and surveillance to monitor disease progression or regression are becoming more mainstream in pediatric dentistry.21
Once the dentist decides to restore a carious primary tooth after assessing disease progression, he or she must decide on which restorative material to use based on caries risk, lesion location and size, moisture control, clinical longevity needed, and, increasingly, esthetics. For small pit and fissure lesions, there is strong evidence for almost all restorative materials.17 However, for interproximal lesions, the evidence is more variable. Aside from amalgam, strong clinical trial evidence is missing for most materials used to restore interproximal lesions in the primary dentition.17 Composite resin and stainless steel crowns have been shown to have high success rates in retrospective studies,22,23 but few clinical trials validate these findings in the primary dentition.24–26 Regardless of material choice, the goal of restorative dentistry is to eliminate disease and restore form, function and esthetics.
Nonsurgical Treatment and Chronic Disease Management: On their own, dental restorations fail to arrest the caries process, especially for children with severe ECC.27,28 Following restoration, the plaque biofilm recolonizes and can reinitiate the caries process if no behavior change takes place.29 These findings emphasize the importance of diagnosing and treating ECC at the patient-level, rather than focusing exclusively on tooth-level interventions.
By understanding the dynamic caries process and focusing on patient-level treatment, dentists can leverage caries regression or arrest when planning pediatric therapy. Early childhood caries chronic disease management (ECC-CDM) takes advantage of this idea and embodies a paradigm shift driving dental interventions toward minimally invasive, nonsurgical treatments to control the disease before restoring form and function.30,31 Many treatments would fit under this nonsurgical umbrella, including active surveillance, silver diamine fluoride, glass ionomer restorations as interim therapeutic restorations, Hall Technique crowns, and frequent use of fluoride varnish.21,32 Often, nonsurgical treatments are provided for caries control in uncooperative children, those with complex medical histories, or in cases of severe disease in order to control the disease while allowing the child to age in a developmental way to a point where conventional surgical treatment can be safely rendered.21,30,31
An additional component of the ECC-CDM framework — and perhaps more important than any intervention the dentist provides — is actively engaging the child/parent/family from diagnosis through self-management and treatment. Combined with nonsurgical caries management techniques, family engagement creates a successful framework for managing ECC.30 Nonsurgical caries treatment requires health behavior changes to make a significant difference in caries activity in young children, because without it, the disease will progress.33 Cases of severe or progressive disease, especially in a child with medical complexity or pre-cooperative behavior, challenge clinicians to develop alternative treatment plans that may include pharmacologic behavior management.
ADVANCED BEHAVIOR MANAGEMENT
Professional guidelines exist to guide pediatric clinical assessments before, during and after procedural sedation.2 No sedation should ever be performed by untrained or ill-prepared providers. Before a child undergoes sedation, a careful medical status review is necessary to screen for medical issues that may alter the sedation regimen selection, or for sedation risk factors (e.g., obstructive sleep apnea, obesity or developmental disability) that may pose risk for adverse events during sedation.2 A primary concern during dental sedation is losing the protective airway reflex, which, if not corrected, can lead to apnea and eventual cardiovascular compromise.2 Providers must make adjustments to treatment recommendations, sedation regimens, or dental procedures to minimize this overall health risk. Consultations with pediatricians and anesthesiologists before procedural sedation are encouraged to identify additional medical risk factors. This team-based approach to care provides more information to influence treatment decisions concerning the child’s ability to medically tolerate the procedure and determine the appropriate venue for care.
INTERSECTION OF DISEASE AND BEHAVIOR MANAGEMENT
With the emergence of ECC-CDM as the contemporary caries management framework and emphasis on advanced behavior management in pediatric dentistry,34,35 clinicians must make a more global assessment of the child’s and family’s overall status and oral health needs when developing treatment recommendations. It may be easy to justify restorative treatment choices for a specific tooth based on caries extent or a preferred method of behavior management. However, a broader medical and dental risk assessment for the pediatric patient should remind clinicians to individualize treatment plans based on the child’s and family’s social context, health behaviors and disease severity.

context, they elected treatment under general anesthesia.
Recently, different authors published clinical decision-making aids to use when planning pediatric dental treatment.21,35 While one focuses on disease management and the other on behavior management, both attempt to bridge this intersection by reviewing the evidence and selection criteria for various treatment strategies. These timely algorithms serve as important discussion points with families, especially when considering the growth in treatment alternatives. In effect, the authors present decision-making guideposts for clinicians who navigate these issues on a daily basis.
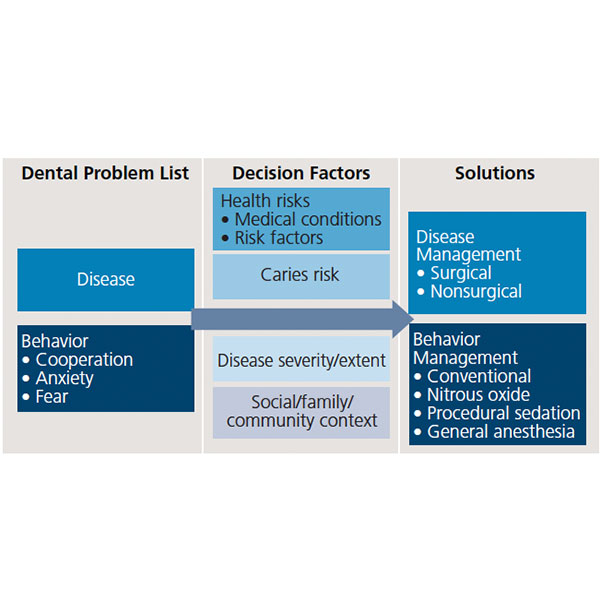
Another way to conceptualize how disease and behavior management intersect is presented in Table 1. Rather than offer another algorithm that tries to quantify and organize decision-making factors, this table poses a framework that allows clinicians to individualize treatment plans based on a particular child’s or family’s circumstances. The precise intersection between disease and behavior management can be highly variable and difficult to measure. For example, a particular child in a dental office may be warm and outgoing one day, and anxious and fearful the next. Likewise, two children with similar health status and caries pattern may demonstrate markedly different rates of caries progression. In a move toward precision dentistry, understanding the social, developmental, biological, and health behavior explanations for a clinical observation can lead to better-informed treatment decisions.36

silver diamine fluoride and conventional behavior management.
DIFFERENT APPROACHES
The following cases illustrate the decision-making framework presented in Table 1. In both instances, a comprehensive, informed-consent process occurred to outline multiple combinations of disease and behavior management alternatives, based on health risk, caries risk, disease extent and severity, and family context. The end product of restorative treatment was the same for both children, and both the children and parents were satisfied with the care they received. However, the path to treatment differed significantly.
In the first case (Figure 1), a 4-year-old presented for a second opinion regarding developing caries lesions. The child had severe asthma controlled with a daily steroid inhaler, as well as large tonsils obstructing nearly 75% of the oropharynx. The dental disease was confined to cervical lesions on the maxillary lateral incisors, and the examination was completed with great difficulty due to the child’s inability to cooperate, which also prohibited radiographs. After discussing the risks and benefits of nonsurgical versus surgical disease management, and conventional versus pharmacologic behavior management, the parents’ preferred option was treatment under general anesthesia. Upon radiographic evaluation in the operating room, lesions were identified only on the maxillary lateral incisors, which were restored with composite resin. No additional restorative treatment was indicated.
In the second case, a family with a 4-year-old traveled more than an hour for a second opinion. This child had no medical conditions or risk factors that would alter treatment recommendations. The dental disease was limited to one primary molar and maxillary central incisors, and the child demonstrated a high level of dental anxiety during the examination. The previous dentist provided options of dental treatment under general anesthesia or conscious sedation, and the family opted to pursue conscious sedation out of concerns for risk and cost. According to the parent, despite the completion of a stainless steel crown on the primary molar, the sedation visit proved a negative experience. As a second opinion, the clinical team discussed a wider variety of behavior and disease management options. After considering the risks and benefits of surgical versus nonsurgical disease management, and general anesthesia versus conventional behavior management, the family elected nonsurgical treatment with silver diamine fluoride (Figure 2). Nine months after the procedure, the family decided to pursue a more esthetic option for the child’s central incisors, so esthetic bonding was completed to remove the black stain from the silver diamine fluoride and restore a natural shade (Figure 3).

SUMMARY
A child’s behavior can complicate decision-making in pediatric dentistry. While various algorithms summarize the evidence and case selection criteria for different treatment strategies,21,35 this paper outlines a framework that considers context beyond the individual lesion or isolated observation of the child’s behavior.
Increasingly, clinical and nonclinical data and risk assessments are driving the profession toward precision dentistry.36 Two similar cases treated differently — but achieving similar clinical endpoints — were presented to illustrate various treatment approaches for navigating the intersection of disease and behavior management. Not all solutions are tolerated by all patients, but decision aids and frameworks exist to help providers find safe venues and alternatives for pediatric therapy. Adopting such an approach supports compassionate and effective care that will frame the dental experience in a positive way for children and their families.
REFERENCES
- Behavior Guidance for the pediatric dental Patient. Pediatr Dent 2017;39:246–259.
- Cote CJ, Wilson S, American Academy of Pediatrics, American Academy of Pediatric Dentistry. Guidelines for monitoring and management of pediatric patients before, during, and after sedation for diagnostic and therapeutic procedures: update 2016. Pediatr Dent. 2016;38:13–39.
- Meyer BD, Chen JW, Lee JY. Pharmacologic management for pediatric dental patients in the 21st century. Gen Dent. 2018;66:19–22.
- American Academy of Pediatric Dentistry. Policy on Early Childhood Caries (ECC):classifications, consequences, and preventive strategies. Pediatr Dent. 2017;39:59–61.
- Dye BA, Mitnik GL, Iafolla TJ, Vargas CM. Trends in dental caries in children and adolescents according to poverty status in the United States from 1999 through 2004 and from 2011 through 2014. J Am Dent Assoc. 2017;148:550–565.
- Bruen BK, Steinmetz E, Bysshe T, Glassman P, Ku L. Potentially preventable dental care in operating rooms for children enrolled in Medicaid. J Am Dent Assoc. 2016;147:702–708.
- Meyerhoefer CD, Panovska I, Manski RJ. Projections of dental care use through 2026: preventive care to increase while treatment will decline. Health Aff (Millwood). 2016;35:2183–2189.
- Fisher-Owens SA, Gansky SA, Platt LJ, et al. Influences on children’s oral health: a conceptual model. Pediatrics. 2007;120:e510–e520.
- Birpou E, Agouropoulos A, Twetman S, Kavvadia K. Validation of different cariogram settings and factor combinations in preschool children from areas with high caries risk. Int J Paediatr Dent. Feb. 8, 2019. Epub ahead of print.
- Christian B, Armstrong R, Calache H, Carpenter L, Gibbs L, Gussy M. A systematic review to assess the methodological quality of studies on measurement properties for caries risk assessment tools for young children. Int J Paediatr Dent. Nov. 9, 2018. Epub ahead of print..
- Featherstone JD, Chaffee BW. The evidence for caries management by risk assessment (CAMBRA). Adv Dent Res. 2018;29:9–14.
- Halasa-Rappel YA, Ng MW, Gaumer G, Banks DA. How useful are current caries risk assessment tools in informing the oral health care decision-making process? J Am Dent Assoc. 2019;150:91–102.
- Twetman S. Caries risk assessment in children: how accurate are we? Eur Arch Paediatr Dent. 2016;17:27–32.
- Divaris K. Predicting dental caries outcomes in children: a “risky” concept. J Dent Res. 2016;95:248–254.
- Gori GB. Individualized or population risks: what is the argument? Am J Public Health. 2001;91:1919.
- Disney JA, Abernathy JR, Graves RC, Mauriello SM, Bohannan HM, Zack DD. Comparative effectiveness of visual/tactile and simplified screening examinations in caries risk assessment. Community Dent Oral Epidemiol. 1992;20:326–332.
- American Academy of Pediatric Dentsitry. Pediatric restorative dentistry. Pediatr Dent. 2017;39:312–324.
- Bader JD, Shugars DA. Understanding dentists’ restorative treatment decisions. J Public Health Dent. 1992;52:102–110.
- Ismail AI, Sohn W, Tellez M, et al. The international caries detection and assessment system (ICDAS): an integrated system for measuring dental caries. Community Dent Oral Epidemiol. 2007;35:170–178.
- Fontana M, Gonzalez-Cabezas C. Evidence-based dentistry caries risk assessment and disease management. Dent Clin North Am. 2019;63:119–128.
- Canares G, Hsu KL, Dhar V, Katechia B. Evidence-based care pathways for management of early childhood caries. Gen Dent. 2018;66:24–28.
- Heintze SD, Rousson V. Clinical effectiveness of direct class II restorations — a meta-analysis. J Adhes Dent. 2012;14:407–431.
- Randall RC. Preformed metal crowns for primary and permanent molar teeth: review of the literature. Pediatr Dent. 2002;24:489–500.
- Atieh M. Stainless steel crown versus modified open-sandwich restorations for primary molars: a 2-year randomized clinical trial. Int J Paediatr Dent. 2008;18:325–332.
- Innes NP, Ricketts DN, Evans DJ. Preformed metal crowns for decayed primary molar teeth. Cochrane Database Syst Rev. 2007;1:CD005512.
- Fuks AB, Araujo FB, Osorio LB, Hadani PE, Pinto AS. Clinical and radiographic assessment of Class II esthetic restorations in primary molars. Pediatr Dent. 2000;22:479–485.
- Berkowitz RJ, Amante A, Kopycka-Kedzierawski DT, Billings RJ, Feng C. Dental caries recurrence following clinical treatment for severe early childhood caries. Pediatr Dent. 2011;33:510–514.
- Sheiham A. Impact of dental treatment on the incidence of dental caries in children and adults. Community Dent Oral Epidemiol. 1997;25:104–112.
- Wright JT, Cutter GR, Dasanayake AP, Stiles HM, Caufield PW. Effect of conventional dental restorative treatment on bacteria in saliva. Community Dent Oral Epidemiol. 1992;20:138–143.
- Ng MW, Ramos-Gomez F, Lieberman M, et al. Disease management of early childhood caries: ECC collaborative project. Int J Dent. 2014;2014:327801.
- Edelstein BL, Ng MW. Chronic disease management strategies of early childhood caries: support from the medical and dental literature. Pediatr Dent. 2015;37:281–287.
- Innes NP, Evans DJ, Stirrups DR. The Hall Technique; a randomized controlled clinical trial of a novel method of managing carious primary molars in general dental practice: acceptability of the technique and outcomes at 23 months. BMC Oral Health. 2007;7:18.
- Fung MHT, Duangthip D, Wong MC, Lo EC, Chu CH. Randomized clinical trial of 12% and 38% silver diamine fluoride treatment. J Dent Res. 2018;97:171–178.
- Lee H, Milgrom P, Huebner CE, et al. Ethics rounds: death after pediatric dental anesthesia: an avoidable tragedy? Pediatrics. 2017;140:pii:e20172370.
- Meyer BD, Lee JY, Thikkurissy S, Casamassimo PS, Vann WF, Jr. An algorithm-based approach for behavior and disease management in children. Pediatr Dent. 2018;40:89–92.
- Divaris K. Precision dentistry in early childhood: the central role of genomics. Dent Clin North Am. 2017;61:619–625.
From Decisions in Dentistry. October 2019;5(9):31—34.

