
A Brief Look at Ankyloglossia Treatment
Dental lasers provide significant benefits in the surgical approach to tongue-tie.
Ankyloglossia (AG), or tongue-tie, is a congenital condition characterized by an abnormally short, thickened, or tight lingual frenum that restricts tongue mobility.1 Consequences of anomalous lingual frena can include limited forward protrusion of the tongue or reduced lateral mobility.2 An emerging term, tethered oral tissues,3 encompasses all buccal-ties and tongue-ties.
Diagnosis and surgical treatment of AG have increased over the past few decades, even without a widely accepted diagnostic criterion.4 Some providers are recognizing AG in the first few days of life and performing procedures prior to going home. If AG is noted past infancy, the treatment options involve observation and language articulation therapy.5,6
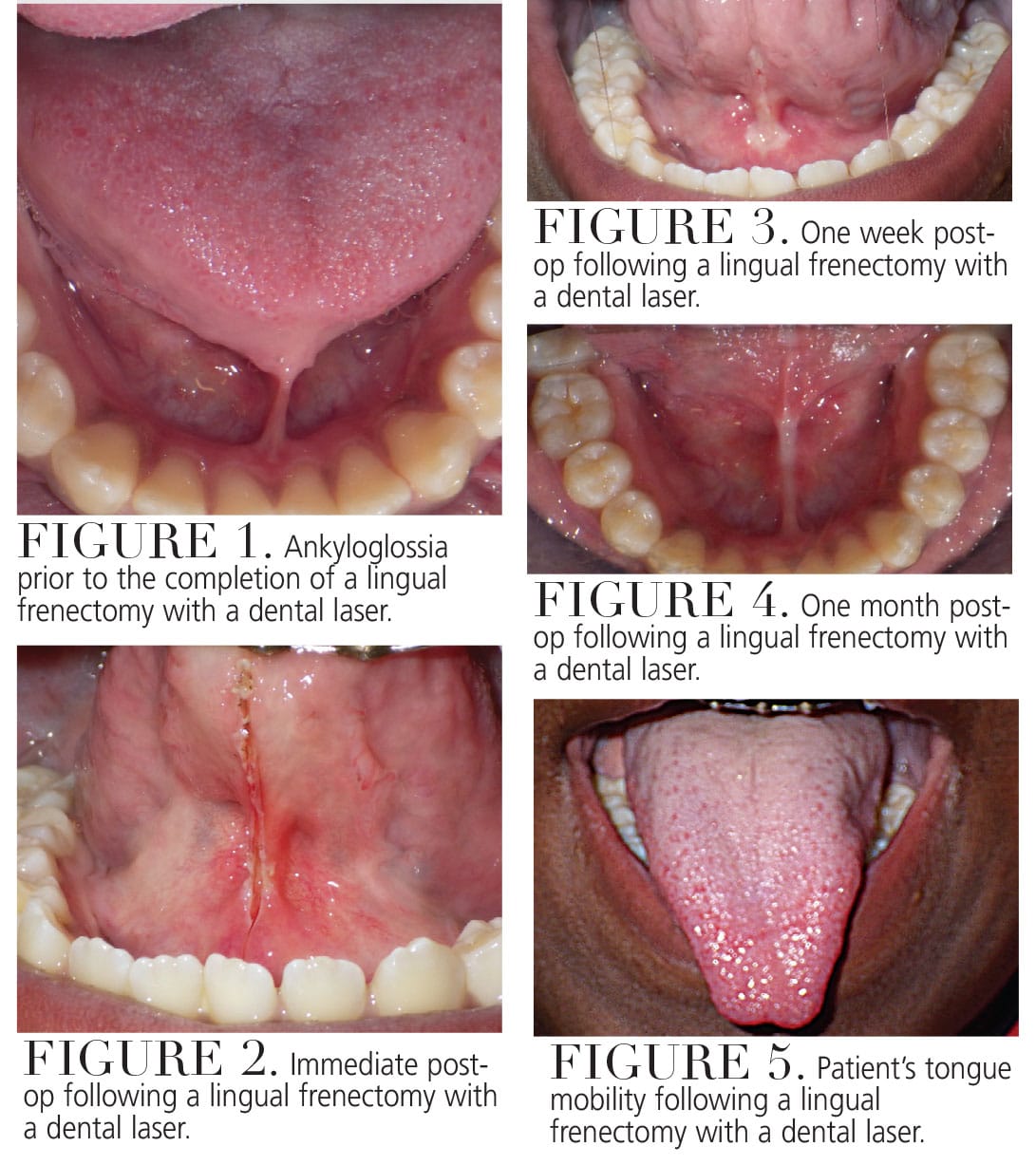
Before treatment is considered, questions should be asked to determine the need for a procedure. Does the tongue-tie need to be surgically removed for function that is more adequate? Is there a more conservative approach that can be taken? If both answers lead toward the need for a procedure, several different approaches can be taken. Figure 1 to Figure 5 show a patient’s attachment pre-procedure, directly after dental laser treatment, 1 week post-op, and 1-month post-op.
The primary treatment in infants is frenotomy, which is simply cutting the frenulum. Frenectomy is the complete excision of the frenulum; and frenuloplasty uses various methods to release the tongue-tie and correct its anatomy.5–8
There is not sufficient evidence to demonstrate which of the three main surgical techniques is the most effective.7 Infants with AG routinely have a frenotomy without local anesthesia, although topical anesthetic or a sucrose solution is highly recommended for pain control and to alleviate any parental concerns. Very little bleeding has been noted after the procedure. One study suggests all post-operative bleeding was controlled with 1 minute of pressure on the wound, and there was no delayed hemorrhage.2,7,9
Technique for performing a frenotomy includes holding the child in a supine position. The tongue is stabilized exposing the frenum. The frenum is then divided with small sterile scissors at its thinnest point.10 Dental lasers can also be used and offer the following advantages: excellent precision, less discomfort, shorter working time, and minimal to no bleeding.11,12
For patients with a thick and vascular frenum, a frenectomy is preferred. The procedure is similar to a frenotomy where the first incision cuts the upper aspect of the frenum and the second incision cuts the lower aspect close to the floor of the mouth.12 The more rarely used procedure is a frenulectomy, or frenuloplasty, which requires general anesthesia in infants and incorporates flap elevations or z-plasties.4
Complications after these procedures are rare.7,11,13 Hemorrhage may occur from severance of the lingual artery, recurrence of tie, lip injury, injury to Wharton’s duct, or the airway may be compromised from asphyxia caused by the released tongue falling back into the airway.7,11,13
Patients can be prescribed antibiotics, analgesics, and warm saline rinses to facilitate faster healing. Post-operative exercises for the tongue are key to establishing improvements in speech.1
References
- Madhusudhan KS. Untying the tongue-tie: a case report. Journal of International Medicine and Dentistry. 2017;4:72–75.
- Muldoon K, Gallagher L, McGuinness D, Smith V. Effect of frenotomy on breastfeeding variables in infants with ankyloglossia (tongue-tie): a prospective before and after cohort study. Biomed Chromatogr. 2017;17:373.
- Kotlow, L. TOTS- Tethered oral tissues: the assessment and diagnosis of the tongue and upper lip ties in breastfeeding. Oral Health. 2015;105:64.
- Walsh J, Tunkel D. Diagnosis and treatment of ankyloglossia in newborns and infants. JAMA. 2017;143:1032–1039.
- Belmehdi A, El Harti K, El Wady W. Ankyloglossia as an oral functional problem as its surgical management. Dental and Medical Problems. 2018;55:213–216.
- Manfro ARG, Manfro R, Bortoluzzi MC. Surgical treatment of ankyloglossia in babies–case report. Int J Oral Maxillofaci Surg. 2010;39:1130–1144.
- Suter V, Bornstein M. Ankyloglossia: facts and myths in diagnosis and treatment. J Periodontol. 2009;80:1204–1219.
- Kotlow LA. Oral diagnosis of abnormal frenum attachments in neonates and infants: evaluation and treatment of the maxillary and lingual frenum using the erbium: YAG laser. J Pediatr Dent. 2004;10:11–14.
- Segal L, Stephenson R, Dawes M, Feldman P. Prevalence, diagnosis, and treatment of ankyloglossia. Can Fam Physicians. 2007;53:1027–1033.
- Krol, D, Keels M. Oral Conditions. Pediatr Rev. 2007;28:15–22.
- Barot V, Vishnoi S, Chandran S, Bakutra G. Laser: The torch of freedom for ankyloglossia. Indian J Plast Surg. 2014:47:418–422.
- Junqueira M, Cunha N, Silva L, et al. Surgical techniques for the treatment of ankyloglossia in children: a case series. J Appl Oral Sci. 2014;22:241–248.
- Salah, K. Localized severe chronic periodontitis with frenal pull and ankyloglossia: a case report. Clin Dent. 2013;7:44–51.
From Decisions in Dentistry. March 2024; 10(2):20
