
Supporting Success in Implant Therapy
Due to the technique’s high success rate, dental implant therapy is an increasingly popular option to replace missing teeth. As is the case in all dental procedures, dental implants are not risk free.
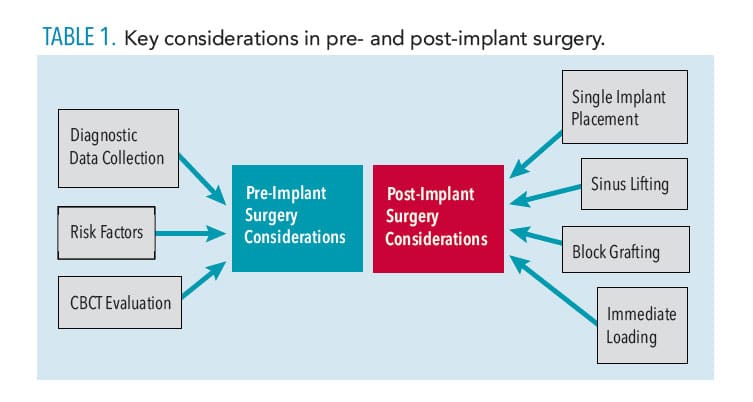
Due to the technique’s high success rate, dental implant therapy is an increasingly popular option to replace missing teeth. As is the case in all dental procedures, dental implants are not risk free. Prior to beginning implant therapy, a full assessment should be completed, including but not limited to taking a detailed patient history and consulting with specialists in order to formulate a comprehensive treatment plan. Planning for prosthetically and surgically driven implant placement with the use of a diagnostic wax up and surgical guide supports optimal implant treatment planning. Diagnostic images—such as cone-beam computed tomography (CBCT)—have become the gold standard for evaluating potential surgical sites. Post-surgical complications—although rare—can occur, and every effort should be made to avoid them, or, if prevention is impossible, monitor closely. This edition of the American Academy of Periodontology’s “The Team Approach” E-Newsletter will provide clinicians with the key elements required both pre- and post-implant placement to achieve the best possible outcomes.
Diagnostic Data Collection
A thorough medical and dental history that includes the patient’s current and previous medication usage and any allergies is fundamentally important to successfully planning any surgical procedure. Patients with certain medical conditions, such as diabetes, hypertension, and osteoporosis, and those taking medications, such as antihypertensives, bisphosphonates, selective serotonin reuptake inhibitors, and proton pump inhibitors, require a more in-depth evaluation in order to determine risks posed by surgery.1–8 Following this discussion, clinical data are captured through radiographic and clinical assessment. Radiographic data should be collected via a combination of full-mouth radiographs, panoramic radiographs, and/or CBCT as recommended by the European Academy of Osseointegration and the Academy of Osseointegration, while remaining conscious of the ALARA (as low as reasonably achieved) principle.9,10 Clinical assessment consists of a full periodontal charting, soft tissue evaluation (gingival biotype and adequacy of attached keratinized gingiva), status of existing restorations (caries risk and etiology of missing teeth), occlusion evaluation, temporomandibular joint evaluation, and oral cancer screening.11–18
Whether the clinician is the sole provider for implant therapy or the surgeon/restorative dentist, the restorative phase should be considered at this time. To aid in the restorative process, photographs should be taken of the patient’s full face, with smile, frontal, and lateral reviews with teeth in occlusion and resting, as well as occlusal views (referenced on photographs at implant assessment). Impressions and bite registration should be sent to the lab for diagnostic cast fabrication and a radiographic template, which will be used for the CBCT scan. Also, the tooth shade, shape, and size of the restoration can be determined at this time.
Risk Factors
Several risk factors can contribute to the success and failure of implant surgery. These can be divided into general risk factors, esthetic risk factors, and occlusion risk factors. General risk factors include: compromised medical condition, smoking, presence of periodontal diseases, small jaw opening, poor oral hygiene, vertical bone resorption, reduced vertical distance between bone crest and opposing tooth, and chronic lesions distant from proposed implant site.8,19–21 Esthetic risk factors include: high maxillary or low mandibular gingival smile line; thin gingiva, causing high possibility of recession; poor oral hygiene; papillae of adjacent teeth (if long and thin, complete regeneration is difficult to achieve); position of interdental contact (contact < 5 mm from bone margin, regeneration takes place in practically all cases, but chances decrease as the distance increases); existence of adjacent implant (difficult to achieve papillary regeneration between two implants because of absence of bony septum); and vertical bone resorption (leading to deep implant placement and more difficult papillary regeneration).22–24 Occlusion risk factors include: bruxism, clenching, tongue thrusting, tongue size, optical implant positioning (improper position or angulation leading to bone and soft tissue loss), unbalanced occlusion, and posterior bite collapse.25–28
Cone-Beam Computed Tomography Evaluation
Effective assessment of a CBCT scan depends on the proposed implant placement in either the maxilla or mandible. With a mandibular implant placement, the evaluation of the inferior alveolar nerve, mental nerve, and incisive mandibular canal for their respective positions, paths, and diameter is important.29 The anatomy of the alveolar ridge/bone should be assessed for potential undercuts (crestal ridge irregularities, suborbital, submandibular fossa, subdigastric fossa).30 Any possible pathologies in the bone or the nerve canals should be evaluated in addition to any root remnants at the proposed implant site(s).31 Finally, evaluating the alveolar dimensions in both height and width for single or multiple implants is necessary. With a maxilla implant placement, the location of the incisive foramen and the greater palatine artery must be determined.32 The distance available for implant placement under the sinus floor and nasal floor and the potential existence and location of septa or soft tissue pathologies in the sinus should be considered.33
Post-Implant Surgery Considerations
After the implant surgery for a single or multiple implants, comprehensive and thorough post-operative instructions should be provided. If appropriate, medications should be prescribed (antibiotics, analgesics, and chlorhexidine rinse) with directions.34 Patients should be advised to avoid sucking liquid through a straw and smoking.35 They should be informed that swelling, pain, and ecchymosis at the surgical site are all common occurrences post-implant surgery.36 Patients should avoid wearing a provisional prosthesis for 2 weeks after implant placement. After the 2 weeks, a provisional prosthesis can be worn, but not while eating and not overnight.37 Brushing or flossing near the surgical site should be avoided for a few days. In immediate loading cases, mastication on implant crown should be avoided for 6 weeks to 8 weeks.38
Sutures will be removed 2 weeks post-surgery. Patients should be advised to call the office if they experience fever, excessive bleeding, unusual pain, or reaction to medications. If a sinus lift procedure was performed, patients should not blow their nose for 2 weeks, as this creates pressure and spreads air through confluent soft tissue planes, creating soft tissue emphysema. Patients should try not to sneeze or cough. If such is unavoidable, patients should keep their mouths open to decrease internal natural pressure and elevate their heads to prevent airway obstruction and aspiration of blood and saliva, and diminish edema. If a sinus communication has occurred during surgery, patients should avoid swimming and strenuous exercise for at least 1 week. If a sinus communication persists, a second procedure may be required to close communication. If a block graft is performed, contact sports and toothbrushing should be avoided immediately after the surgery, but can be resumed the second day after surgery.
Conclusion
Although we have much to learn about potential implant therapy complications, this summary of pre- and post-implant surgery complications can serve as a guide for clinicians. Remaining abreast of new research regarding implant complications will help clinicians prepare for potential problems and help improve patient outcomes and implant success rates.
References
- Genco RJ, Borgnakke WS. Risk factors for periodontal disease. Periodontol 2000. 2013;62:59–94.
- Nunn ME. Understanding the etiology of periodontitis: an overview of periodontal risk factors. Periodontol 2000. 2003;32:11–23.
- Bergström J, Preber H. Tobacco use as a risk factor. J Periodontol. 2012;65:545–550.
- Grossi SG, Zambon JJ, Ho AW, et al. Assessment of risk for periodontal disease. I. Risk indicators for attachment loss. J Periodontol. 1994;65:260–267.
- Tonneti MS. Cigarette smoking and periodontal diseases: etiology and management of disease. Ann Periodontol. 1998;3:88–101.
- Tonetti MS, Eickholz P, Loos BG, et al. Principles in prevention of periodontal diseases: consensus report of group 1 of the 11th European Workshop on Periodontology on effective prevention of periodontal and peri-implant diseases. J Clin Periodontol. 2015;42:S5–S11.
- Albandar JM, Susin C, Hughes FJ. Manifestations of systemic diseases and conditions that affect the periodontal attachment apparatus: case definitions and diagnostic considerations. J Clin Periodontol. 2018;45:S171–S189.
- Nelson RG, Shlossman M, Budding LM, et al. Periodontal disease and NIDDM in Pima Indians. Diabetes Care. 1990;13:836–840.
- Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: framework and proposal of a new classification and case definition. J Periodontol. 2018;89:S159–S172.
- Taylor JJ, Preshaw PM, Lalla E. A review of the evidence for pathogenic mechanisms that may link periodontitis and diabetes. J Clin Periodontol. 2013;40:S113–134.
- Lalla E, Papapanou PN. Diabetes mellitus and periodontitis: a tale of two common interrelated diseases. Nat Rev Endocrinol. 2011;7:738–748.
- Polak D, Shapira L. An update on the evidence for pathogenic mechanisms that may link periodontitis and diabetes. J Clin Periodontol. 2018;45:150–166.
- Sanz M, Ceriello A, Buysschaert M, et al. Scientific evidence on the links between periodontal diseases and diabetes: consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International diabetes Federation and the European Federation of Periodontology. Diabetes Res Clin Pract. 2018;137:231–241.
- Engebretson S, Kocher T. Evidence that periodontal treatment improves diabetes outcomes: a systematic review and meta-analysis. J Periodontol. 2013;84(4 Suppl):S153–S169.
- Chapple IL, Genco R. Diabetes and periodontal diseases: consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J Clin Periodontol. 2013;40(Suppl 14):S106–S112.
- Katz J. Elevated blood glucose levels in patients with severe periodontal disease. J Clin Periodontol. 2001;28:710–712.
- Nishida N, Tanaka M, Hayashi N, et al. Determination of smoking and obesity as periodontitis risks using the classification and regression tree method. J Periodontol. 2005:76:923–928.
- Chaffee BW, Weston SJ. Association between chronic periodontal disease and obesity: a systematic review and meta-analysis. J Periodontol. 2010:81:1708–1724.
- Genco RJ, Borgnakke WS. Risk factors for periodontal disease. Periodontol 2000. 2013;62:59–94.
- Eke PI, Thornton-Evans GO, Wei L, Borgnakke WS, Dye BA, Genco RJ. Periodontitis in US adults: National Health and Nutrition Examination Survey 2009-2014. J Am Dent Assoc. 2018;149:576–588.
- Eke PI, Wei L, Thornton-Evans GO, et al. Risk indicators for periodontitis in US adults: NHANES 2009 to 2012. J Periodontol. 2016;87:1174–1185.
- Eke PI, Wei L, Borgnakke WS, et al. Periodontitis prevalence in adults ≥ 65 years of age, in the USA. Periodontol 2000. 2016;72:76–95.
- Michalowicz BS, Aeppli D, Virag JG, et al. Periodontal findings in adult twins. J Periodontol. 1991;62:293–299.
- Michalowicz BS, Diehl SR, Gunsolley JC, et al. Evidence of a substantial genetic basis for risk of adult periodontitis. J Periodontol. 200071:1699–1707.
- Shiau HJ, Reynolds MA. Sex differences in destructive periodontal disease: a systematic review. J Periodontol. 2010;81:1379–1389.
- Shiau HJ, Reynolds MA. Sex differences in destructive periodontal disease: exploring the biologic basis. J Periodontol. 2010;81:1505–1517.
- Eke PI, Dye BA, Wei L, et al. Update on prevalence of periodontitis in adults in the United States: NHANES 2009 to 2012. J Periodontol. 2015;86:611–622.
- Bissada NF, Abdelmalek RG. Incidence of cervical enamel projections and its relationship to furcation involvement in Egyptian skulls. J Periodontol. 1973;44:583–585.
- Hou GL, Tsai C-C. Relationship between periodontal furcation involvement and molar cervical enamel projections. J Periodontol. 1987;58:715–721.
- Ainamo J. Relationship between malalignment of the teeth and periodontal disease. Scand J Dent Res. 1972;80:104–110.
- el-Mangoury NH, Gaafar SM, Mostafa YA. Mandibular anterior crowding and periodontal disease. Angle Orthod. 1987;57:33–38.
- Withers JA, Brunsvold MA, Killoy WJ, Rahe AJ. The relationship of palato-gingival grooves to localized periodontal disease. J Periodontol. 1981;52:41–44.
- American Academy of Periodontology. Statement on risk assessment. J Periodontol. 2008;79:202.
- Garcia RI, Compton R, Dietrich T. Risk assessment and periodontal prevention in primary care. Periodontol 2000. 2016;71:10–21.
- Page RC, Krall EA, Martin J, Mancl L, Garcia RI. Validity and accuracy of a risk calculator in predicting periodontal disease. J Am Dent Assoc. 2002;133:569–576.
- Lang NP, Tonetti MS. Periodontal risk assessment (PRA) for patients in supportive periodontal therapy (SPT). Oral Health Prev Dent. 2003;1:7–16.
- Trombelli L, Farina R, Ferrari S, Pasetti P, Calura G. Comparison between two methods for periodontal risk assessment. Minerva Stomatol. 2009;58:277–287.
- Kye W, Davidson R, Martin J, Engebretson S. Current status of periodontal risk assessment. J Evid Based Dent Pract. 2012;12(3 Suppl):2–11.

[…] post Supporting Success in Implant Therapy appeared first on Decisions in […]