

Diagnosing Developmental Tooth Anomalies
Early diagnosis of these morphological variations may help improve esthetic and functional treatment outcomes.
Early diagnosis of these morphological variations may help improve esthetic and functional treatment outcomes
The authors have no commercial conflicts of interest to disclose.
This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Identify the different types of developmental tooth anomalies.
- Discuss the etiology of these morphological variations.
- List the appropriate treatment strategies for tooth anomalies.
Dental anomalies are relatively common, with 36.7% to 40.3% of nonsyndromic patients presenting with at least one dental anomaly, depending on the population evaluated.1,2 They are caused by both genetic and environmental factors. While a few genes have been identified as being responsible for specific dental anomalies,1 the etiology for most remains unknown. Being well versed in dental anomalies can help clinicians determine appropriate management and treatment strategies.
Tooth agenesis is the lack of development of one or more teeth, and is one of the most common dental anomalies.3 Hypodontia is the absence of one or more teeth. Oligodontia refers to the missing of six or more teeth, while anodontia is the complete absence of teeth. The prevalence of hypodontia is estimated at 2.7% to 6.3% among orthodontic patients, with no significant difference noted between genders.4,5 Hypodontia can be an isolated anomaly or it may be part of a syndrome.6–8 Its prevalence in the general population varies depending on race, type of dentition (primary versus permanent), and tooth type.4 Cases of oligodontia are extremely rare in the general population and are most often associated with a syndrome, including orofaciodigital syndrome Type I and orofacial clefting syndromes — such as Van Der Woude syndrome, Ellis-Van Creveld syndrome and Rapp-Hodgkin syndrome.
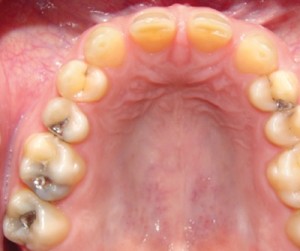
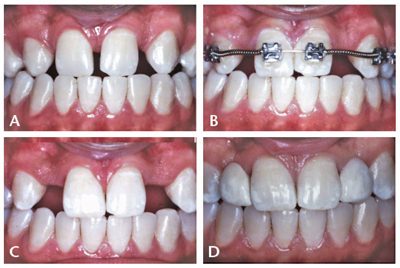
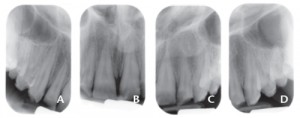
The third molars in the permanent dentition are the most commonly missing teeth, followed by the mandibular second bicuspids or the maxillary lateral incisors.9 Congenitally missing maxillary lateral incisors often present an esthetic challenge (Figure 1). Treatment is frequently performed to limit diastemata, preserve facial symmetry and improve facial esthetics. One approach involves maintaining or gaining Class I interarch canine tooth relationships while creating embrasures large enough to permit the subsequent placement of dental implants or fixed partial dentures (Figure 2A through Figure 2D). Another approach is to close the spaces with orthodontic appliances and reshape the canines using veneers to simulate the shape of the missing lateral incisors.
EXTRA TEETH
Hyperdontia is the presence of one or more extra teeth, which often include oddly shaped supernumerary teeth. Supernumerary teeth are classified according to their form and location. Mesiodens, which appears in the maxillary midline, is the most common type, but supernumerary teeth can be found in almost any region of the dental arches.10 The etiology of hyperdontia is not well understood, but one theory suggests that alterations in tooth number are the result of local hyperactivity of the dental lamina.11 The presence of multiple supernumerary teeth should raise the possibility that a disease or syndrome — such as cleft lip and palate, cleidocranial dysostosis, Gardner syndrome, Ehlers-Danlos syndrome, Fabry Anderson’s syndrome, chondroectodermal dysplasia, incontinentia pigmenti or tricho rhino-phalangeal syndrome — is ultimately responsible for this anomaly.12,13
DEVELOPMENTAL ISSUES
Dens evaginatus, also called talon cusp, is an uncommon developmental aberration of an anterior tooth. It can also result in the formation of a supernumerary tubercle that extends from the occlusal aspect of an otherwise normal posterior tooth.1,14,15 This outward projection of enamel most commonly affects the lateral incisors and premolars. Studies suggest that Asians and Native Americans are disproportionately affected by dens evaginatus.15 Occasionally, a tiny pulp horn can be found in the tubercle. This can lead to a connection from the oral cavity to the pulp due to occlusal wear.
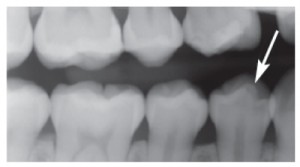
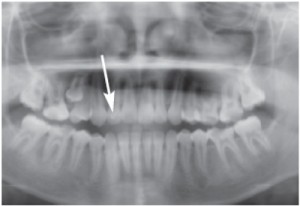
From a radiographical standpoint, dens evaginatus appears as an extra cusp on the occlusal surface of the tooth. The dentin and pulp may appear to extend beyond the occlusal surface toward the oral cavity (Figure 3 and Figure 4). Treatment includes removing the tubercle (if it has not already been worn away), followed by restoration of the occlusal surface, thereby sealing the pulp from exposure to the oral cavity. If the tubercle is so worn that the pulp becomes exposed or symptoms of irreversible pulpitis are present, endodontic therapy or extraction will be necessary. During treatment planning, clinicians should take this dental anomaly into consideration when attempting to create arch space by extracting one or more premolars. A prudent plan may involve the extraction of anomalous premolar(s), as opposed to removing the unaffected premolar(s).16
Dens invaginatus is the infolding of enamel into a pulp chamber and/or canal from the occlusal or incisal surface.17 More severe infolding that includes 50% of the canal space or more is referred to as dens in dente (tooth in a tooth). The affected dentition typically has otherwise normal anatomy. In contrast, a tooth with severe infolding is referred to as a dilated odontome.17 Clinically, a dens invaginatus may appear as a small pit on the occlusal or incisal surface and is most commonly associated with maxillary lateral incisors. It is rarely seen in mandibular and/or primary teeth.18
Radiographically, dens invaginatus presents as a well defined, inverted teardrop shape in the pulp space. The teardrop has a radiopaque border and a radiolucent center. The radiopacity of the border is similar to enamel. Sometimes the enamel border will appear continuous with the enamel of the outer surface of the crown. The infolding may be severe enough to enlarge the pulp space. Treatment typically involves sealing the pit to prevent bacterial contamination in the infolded area. If left untreated, abscesses or early pulpal necrosis can develop.18
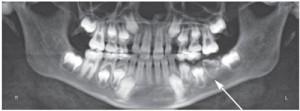
Dilaceration is an abnormal curvature of the roots (Figure 5 and Figure 6).19 This is not clearly visible in the oral cavity during the clinical examination and is typically seen only on radiographs. Dilaceration can occur with any tooth and may be caused by trauma to the apices of deciduous dentition, which lie close to the permanent tooth buds.19 An abnormal curvature of the root toward the mesial or distal is easily seen on periapical radiographs. When the root curves to the facial or lingual, it can be more difficult to detect. A target (or bull’s eye) appearance may be evident in these circumstances. Oftentimes, no treatment is necessary. If extraction is indicated, however, the procedure may prove difficult.


Enamel pearls are masses of enamel found on the roots of molars.20 They are thought to arise from the continued formation of enamel by Hertwig’s epithelial root sheath. Enamel pearls typically do not have any clinical signs, but if they are located near the cemento-enamel junction (CEJ), loss of bone or periodontal ligament attachment may be present.21,22 Enamel pearls occur in approximately 3% to 6% of individuals, depending on the population studied. Radiographically, they appear as well defined, radiopaque round masses on the roots of a molar, and are most commonly associated with maxillary molars (Figure 7). They are small, ranging from 1 mm to 3 mm in diameter (Figure 8). When diagnosing the presence of an enamel pearl, it is helpful to take two radiographs of the same tooth at different horizontal angles. This will help rule out a “pseudo pearl” caused by superimposition of the roots (most commonly seen on mandibular molars in the area of the furcation). While treatment is not necessary, challenges can arise during periodontal therapy or extraction of these teeth.
Taurodontism is a multirooted tooth with a long body and pulp chamber and shortened roots.23 Taurodontism is not visible on clinical examination, as the crown is unaffected, but it can be detected in radiographs or during extractions. It occurs in 2.5% to 11.3% of the population, and is most often associated with mandibular molars.24–27 There is an increased incidence of taurodontism among individuals with Down syndrome.28 Treatment is not necessary, but challenges may arise during endodontic therapy or extraction.


Amelogenesis imperfecta is a genetic disturbance in enamel formation leading to altered enamel morphology, but with normal dentin and pulp formation on all teeth (Figure 9A through Figure 9D). The affected enamel has decreased resistance to decay. The teeth appear yellowish brown, while the affected enamel’s appearance varies. The crowns have a square shape with multiple open contacts. It affects deciduous and permanent dentitions equally. Restorative treatment is typically performed for esthetic and functional purposes.
COURTESY OF DAVID E. KLINGMAN, DMD
Dentinogenesis imperfecta is a genetic disturbance in dentin formation leading to altered morphology of dentin on all teeth. Type I is associated with osteogenesis imperfecta. Type II has no associated skeletal defects, and Type III is isolated to the Brandywine region of Maryland. Types I and II are caused by mutations of the dentin sialophospho-protein gene on chromosome 4.29 The teeth appear bluish-gray and have a hint of translucency. The enamel easily fractures due to the altered morphology of the dentin. The crowns have a bulbous appearance due to a constricted CEJ. The roots are short and slender, with partial or complete obliteration of the pulp chamber and root canals. Dentinogenesis imperfecta is found in approximately 25% of all osteogenesis imperfecta cases. Restorative treatment is often needed to improve esthetics and function.
Regional odontodysplasia is a rare condition with hypoplastic and hypocalcified enamel and dentin (Figure 10).30,31 It is usually associated with a single quadrant in the oral cavity. The teeth are smaller than normal and brownish in color. Affected teeth have large pulp chambers and root canals, with thin enamel and dentin.32,33 Restorative treatment is usually indicated to improve esthetics and function.


Fusion occurs when two adjacent developing tooth germs fuse into one large tooth, ultimately resulting in one less tooth in the arch (Figure 11).34 This occurs most commonly in the anterior region. The crowns of the fused teeth appear much larger than normal. Sometimes there is a cleft noting the two separate crowns. No treatment is necessary, but restorative care may be completed for esthetic purposes.
Gemination occurs when a developing tooth germ attempts to divide but the process is not completed, resulting in an abnormally large tooth with a normal tooth count in the arch (Figure 12).34 When there is complete division, a supernumerary tooth is produced. Gemination typically results in one large root and pulp chamber. No treatment is necessary, but restorative care may be performed to improve esthetics.
CONCLUSION
Oral health professionals should be aware of the morphological variations and tooth anomalies observed during routine dental evaluations. If unrecognized, such abnormalities may impose treatment difficulties. Similarly, recognition of dental anomalies may give dentists an advantage while formulating a thorough and effective treatment plan.
References
- Uslu O, Akcam MO, Evirgen S, Cebeci I. Prevalence of dental anomalies in various malocclusions. Am J Orthod Dentofacial Orthop. 2009;135:328–335.
- Patil S, Doni B, Kaswan S, Rahman F. Prevalence of dental anomalies in Indian population. J Clin Exp Dent. 2013;5:e183–e186.
- Symons AL, Stritzel F, Stamation J. Anomalies associated with hypodontia of the permanent lateral incisor and second premolar. J Clin Pediatr Dent. 1993;17:109–111.
- Gomes RR, da Fonseca JA, Paula LM, Faber J, Acevedo AC. Prevalence of hypodontia in orthodontic patients in Brasilia, Brazil. Eur J Orthod. 2010;32:302–306.
- Silva Meza R. Radiographic assessment of congenitally missing teeth in orthodontic patients. Int J Paediatr Dent. 2003;13(2):112–116.
- Hall RK. Congenitally missing teeth — a diagnostic feature in many syndromes of the head and neck. J Int Assoc Dent Child. 1983;14:69–75.
- Vierucci S, Baccetti T, Tollaro I. Dental and craniofacial findings in hypohidrotic ectodermal dysplasia during the primary dentition phase. J Clin Pediatr Dent. 1994;18:291–297.
- Schalk-van der Weide Y, Beemer FA, Faber JA, Bosman F. Symptomatology of patients with oligodontia. J Oral Rehabil. 1994;21:247–261.
- Lavelle CL, Ashton EH, Flinn RM. Cusp pattern, tooth size and third molar agenesis in the human mandibular dentition. Arch Oral Biol. 1970;15:227–237.
- Lara TS, Lancia M, da Silva Filho OG, Garib DG, Ozawa TO. Prevalence of mesiodens in orthodontic patients with deciduous and mixed dentition and its association with other dental anomalies. Dental Press J Orthod. 2013;18:93–99.
- Liu JF. Characteristics of premaxillary supernumerary teeth: a survey of 112 cases. ASDC J Dent Child. 1995;62:262–265.
- Fonseca LC, Kodama NK, Nunes FC, et al. Radiographic assessment of Gardner’s syndrome. Dentomaxillofac Radiol. 2007;36:121–124.
- Rocha R, Zasso MB, Floriano G, et al. Orthodontic traction in a patient with cleidocranial dysplasia: 3 years of follow up. Am J Orthod Dentofacial Orthop. 2014;146:108–118.
- Priya M, Muthu MS, Jeevarathan J, Rathnaprabhu V. Unusual dens evaginatus on maxillary premolars: a case report. J Dent Child (Chic). 2011;78:71–75.
- Yip WK. The prevalence of dens evaginatus. Oral Surg Oral Med Oral Pathol. 1974;38:80–87.
- McCulloch KJ, Mills CM, Greenfeld RS, Coil JM. Dens evaginatus from an orthodontic perspective: report of several clinical cases and review of the literature. Am J Orthod Dentofacial Orthop. 1997;112:670–675.
- Sebastian AA, Ahsan A, George AJ, Aby J. An unusual triad: Bilateral dilated odontoma, hypodontia and peg laterals. Dent Res J (Isfahan). 2013;10:674–677.
- Spallarossa M, Canevello C, Silvestrini Biavati F, Laffi N. Surgical orthodontic treatment of an impacted canine in the presence of dens invaginatus and follicular cyst. Case Rep Dent. 2014;2014:643082.
- Xue JJ, Ye NS, Li JY, Lai WL. Management of an impacted maxillary central incisor with dilacerated root. Saudi Med J. 2013;34:1073–1079.
- Mao XQ. Root-like enamel pearl: a case report. J Med Case Rep. 2014;8:248.
- Goldstein AR. Enamel pearls as contributing factor in periodontal breakdown. J Am Dent Assoc. 1979;99:210–211.
- Croft LK. Periodontal abscess from enamel pearl. Oral Surg Oral Med Oral Pathol. 1971;32:154.
- Dineshshankar J, Sivakumar M, Balasubramanium AM, et al. Taurodontism. J Pharm Bioallied Sci. 2014;6(Suppl 1):S13–S15.
- Barker BC. Taurodontism: the incidence and possible significance of the trait. Aust Dent J. 1976;21:272–276.
- Patil S, Doni B, Kaswan S, Rahman F. Prevalence of taurodontism in the North Indian population. J Clin Exp Dent. 2013;5:e179–e182.
- Nagaveni NB, Radhika NB. Prevalence of taurodontism in primary mandibular first molars of ethnic Indian children. Gen Dent. 2012;60:e335–e340.
- Bronoosh P, Haghnegahdar A, Dehbozorgi M. Prevalence of taurodontism in premolars and molars in the South of Iran. J Dent Res Dent Clin Dent Prospects. 2012;6:21–24.
- Alpöz AR, Eronat C. Taurodontism in children associated with trisomy 21 syndrome. J Clin Pediatr Dent. 1997;22:37–39.
- Cabay RJ. An overview of molecular and genetic alterations in selected benign odontogenic disorders. Arch Pathol Lab Med. 2014;138:754–758.
- Barbería E, Sanz Coarasa A, Hernández A, Cardoso-Silva C. Regional odontodysplasia. A literature review and three case reports. Eur J Paediatr Dent. 2012;13:161–166.
- Chinn C, Kohli K. Regional odontodysplasia. A case report. N Y State Dent J. 2003;69:27–29.
- Vaikuntam J, Tatum NB, McGuff HS. Regional odontodysplasia: review of the literature and report of a case. J Clin Pediatr Dent. 1996;21:35–40.
- Carlos R, Contreras-Vidaurre E, Almeida OP, et al. Regional odontodysplasia: morphological, ultrastructural, and immunohistochemical features of the affected teeth, connective tissue, and odontogenic remnants. J Dent Child (Chic). 2008;75:144–150.
- Milazzo A, Alexander SA. Fusion, gemination, oligodontia, and taurodontism. J Pedod. 1982;6:194–199.

