
Oral Biofilm’s Role in Disease Pathogenesis
Understanding biofilm-associated diseases is key to successful prevention, diagnosis and treatment.
Understanding biofilm-associated diseases is key to successful prevention, diagnosis and treatment.
With the growing rate of antimicrobial resistance and the increasing cost of health care in the United States, an improved understanding of prevention, diagnosis and treatment of biofilm-associated disease has become a major focus in medical and oral health care. Periodontal disease, dental caries and endodontic infections are among the most commonly encountered oral conditions, and additional research is needed to better characterize and develop treatment modalities to reduce their destructive nature. Pathogenic organisms in oral microbial communities are a major risk factor in the development and progression of these diseases. If left untreated, destruction of the tooth and its supporting structures can occur, leading to tooth loss. And in the case of plaque biofilm, specifically, periodontal maintenance with periodic recare intervals is critical for the prevention of plaque/biofilm-related disease and for reinforcing effective patient self-care regimens.
TINA CARVALHO, UNIVERSITY OF HAWAII AT MANOA/NATIONAL CANCER INSTITUTE/SCIENCE PHOTO LIBRARY
DOWSETT, PUBLIC HEALTH ENGLAND/SCIENCE PHOTO LIBRARY
HOW DOES THE SUBGINGIVAL BIOFILM THAT FORMS FOLLOWING PERIODONTAL MAINTENANCE DIFFER FROM BIOFILM FOUND ELSEWHERE IN THE ORAL CAVITY?
Periodontal maintenance is aimed at minimizing the recurrence or severity of disease in patients previously treated for periodontal or peri-implant disease. Clinicians perform several therapies during the maintenance visit, which directly or indirectly impact the composition of supragingival and subgingival biofilm in diseased and nondiseased sites. Treatment involves mechanical removal of subgingival and supragingival biofilm/calculus with hand and/or ultrasonic instruments, followed by behavioral modification strategies, as needed. Furthermore, systemic antibiotics, local antimicrobials and surgical interventions may also be necessary for disease management.1
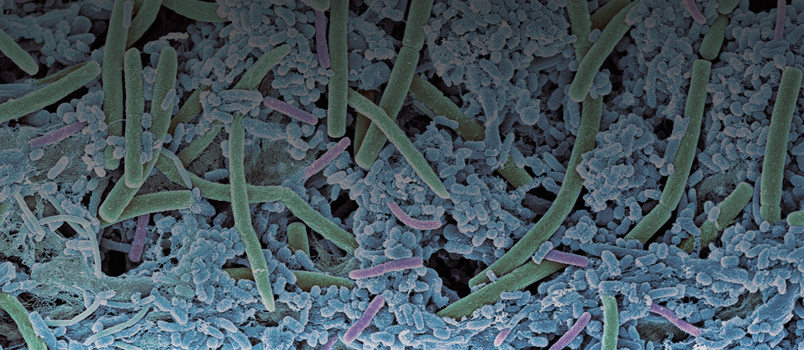
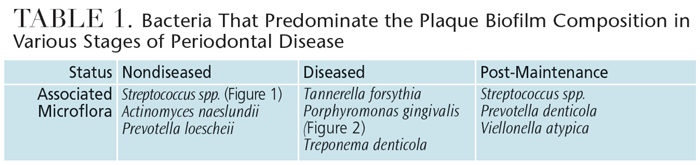
Healthy gingival sulci have a different microbial composition than the flora associated with periodontal disease. Supragingival biofilm is dominated by aerobic Gram-positive cocci and short rods, which are classified as commensal microorganisms. Subgingival biofilm is predominated by anaerobic Gram-negative rods and filaments, as well as spirochetes, any of which can be involved in the etiopathogenesis of periodontal disease (Table 1). Individuals with periodontal disease have subgingival biofilm and may have calculus on the teeth proximate to their periodontal pockets. These infections elicit several reactions from the host’s immune system. A periodontal infection combined with inflammation can cause clinical attachment loss.
The gold standard for periodontal treatment is thorough subgingival scaling and root planing, which may require periodontal surgery to ensure adequate access. When detecting calculus, a dental endoscope may be more effective than a tactile explorer.2 Following thorough debridement of diseased periodontal pockets, the population of Gram-negative bacteria is reduced, which enables the number of Gram-positive bacteria to increase within 24 hours to 48 hours post-treatment.3 The use of subantimicrobial tetracycline family drugs that inhibit proteolytic enzymes in gingival tissue may enhance the outcomes of scaling and root planing — at least in the short term.4 According to a recent systematic review that included meta-analyses, other therapies, such as systemic antimicrobials, chlorhexidine chips, and photodynamic therapy with a diode laser, may also be effective adjuncts to scaling and root planing.5
key takeaways
- The multifactorial nature and evolving composition of oral biofilm pose health risks to hard and soft oral tissues.
- In the case of plaque biofilm, periodontal maintenance seeks to minimize the recurrence or severity of disease in patients previously treated for periodontal or peri-implant conditions.
- Healthy gingival sulci have a different microbial composition than the flora associated with periodontal disease. Maintenance therapies directly or indirectly impact the composition of supragingival and subgingival biofilm in diseased and nondiseased sites.
- The gold standard for periodontal treatment is thorough subgingival scaling and root planing, which may require periodontal surgery to ensure adequate access.
- Putative periodontal pathogens show differences in susceptibility to therapy, suggesting that maintenance intervals need to be individualized based on the results of frequent monitoring.
- Oral biofilm significantly impacts the initiation and progression of periodontal disease and its repeated removal, both supragingivally and subgingivally, is paramount to improving and maintaining oral health.
- Evidence suggests that multiple bacterial combinations are responsible for the disease process, and that the composition and interactions of biofilm communities may predispose individuals to infections.19
DO CHANGES IN BIOFILM COMPOSITION IMPACT RECARE FREQUENCY?
Periodic maintenance and recare visits form the foundation of a meaningful long-term effort to prevent or limit subsequent attachment loss.6 The duration of initial and delayed healing responses to periodontal therapy depends on the nature and extent of the disease, modality of therapy, and type of care provided during the healing stage.1
Previous research has illustrated that in patients with chronic generalized mild to severe periodontitis, improvements in periodontal health (e.g., decreased bleeding on probing and pocket depths, and gains in clinical attachment) were noted during the initial four weeks after a single episode of scaling and root planing.7 Studies conducted on bacterial repopulation suggest that it takes several months for pathogenic bacteria to reestablish themselves.8 Improvements in clinical and microbiological parameters following periodontal treatment support a three-month interval between periodontal maintenance visits. Although research suggests that longer intervals (e.g., six months) may be appropriate for patients who are able to maintain adequate plaque control, other patients may need more frequent periodontal maintenance visits.7
A multicenter, split-mouth study assessed several putative periodontal pathogens associated with chronic periodontitis and their responses to traditional periodontal therapy. With the exception of Porphyromonas gingivalis, the number and proportion of detectable pathogens exhibited temporal responses. Other pathogens exhibited an initial decrease immediately following therapy, a rise in proportions one month to three months post-therapy, and a spontaneous decline in the absence of therapy over a three-month to 12-month period.8 Taken together, putative periodontal pathogens show differences in susceptibility to periodontal therapy, suggesting that maintenance care intervals need to be customized based on the results of frequent monitoring.
Individuals diagnosed with aggressive periodontitis generally require a greater frequency in periodic maintenance and recare visits. Evidence of rapid attachment loss and low levels of biofilm deposits presents clinical challenges in preventing disease progression, and may require an interdisciplinary approach with other dental specialists. The diagnosis of aggressive periodontitis is often made at an advanced stage of the disease, which results in clinicians treating severely compromised teeth. Consequently, after nonsurgical therapy, residual pockets will remain. Pathogenic microorganisms, such as Aggregatibacter actinomycetemcomitans, have been shown to invade the pocket epithelium and remain persistent. Hence, the conventional treatment of aggressive periodontitis may include surgical removal of the pocket epithelium and administration of systemic antibiotics.9 More recently, nonsurgical therapy with adjunct photodynamic therapy using lasers has been found to be effective in eliminating A. actinomycetemcomitans.10 Lasers may be as effective as surgical therapy in treating aggressive periodontitis.11 More research is needed, however, to substantiate these adjunctive therapies.
SIDEBAR: Composition and Interaction Of Oral Microbial Communities

The multifactorial nature and evolving composition of oral biofilm pose health risks to hard and soft oral tissues. In addition to periodontal disease and dental caries, for instance, pathogenic microbiota have been implicated in endodontic infections. And in some cases, pathogenic agents may be common to more than one condition. For example, Lins et al reported that Enterococcus faecalis, which is usually not regarded as a significant component of the oral microbiota, has been associated with caries, chronic periodontitis and apical periodontitis.18
Although the role of enterococci such as E. faecalis in endodontic infections is not clearly understood, the evidence suggests that isolating a single or major etiological species is unlikely.18 Rather, the heterogeneous etiology of apical periodontitis indicates that multiple bacterial combinations are responsible for the disease process, and that the composition and interactions of microbial communities may predispose individuals to infections.19 In the Lins study, opportunistic pathogens such as enterococci, for example, were reported to have transferred virulence traits to related species.18 E. faecalis is frequently found in the root canals of teeth with failed endodontic treatment, and there is also evidence of it as a pathogenic agent in periodontal disease.20 In particular, it has been found in high prevalence in the oral biofilm of patients with the human immunodeficiency virus and necrotizing or chronic periodontal disease.20
Ultimately, developing effective preventive and therapeutic measures hinges on our understanding of how the composition of the bacterial community and interactions among microbiota affect the disease process.
WHAT IS THE OBJECTIVE OF PERIODONTAL THERAPY?
Removal of calculus and biofilm is accomplished using hand or ultrasonic instrumentation, or a combination of both. While difficult to achieve, the ultimate goal of periodontal therapy is complete removal of nonmicroscopic calculus and biofilm. A significant reduction of pathological bacteria in periodontal pockets may permit repopulation by nonpathogenic microbes. In turn, this may down-modulate the immune response, thereby limiting or eliminating cytokines that facilitate destruction of the periodontium.
Evidence suggests that nonsurgical treatment results measuring clinical and microbiological periodontal conditions for chronic periodontitis are similar for both hand and ultrasonic scaling at six months post-operatively.12 For single-rooted teeth, a comparable effectiveness between manual and ultrasonic instrumentation has been shown for the treatment of chronic periodontitis.12 While some research has found ultrasonic instrumentation to be superior in the treatment of class II and III furcations, scaling and root planing remains more effective for improving clinical attachment loss.9 Regardless of the modality used, however, clinicians should bear in mind that periodontal maintenance must be individualized for each patient.
WHAT IS THE HOST RESPONSE TO DEEP POCKET BIOFILM AND PATHOGENS?
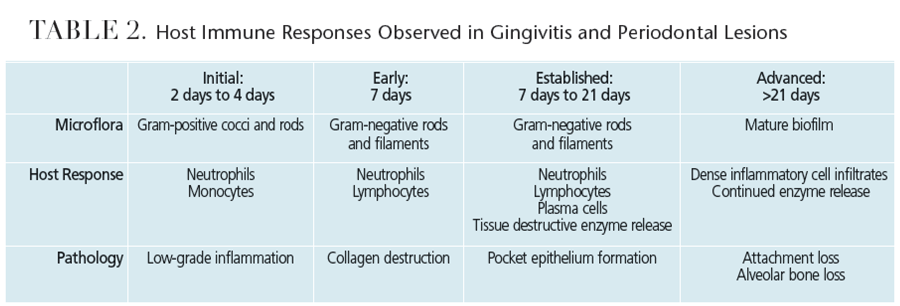
Periodontal disease results from complex interactions between subgingival biofilms and hosts’ immune systems. In gingivitis, the inflammatory lesion is largely confined to the gingiva. In periodontitis, however, the inflammatory processes extend to affect the periodontal ligament and alveolar bone. The net result of these inflammatory changes is the subsequent breakdown of the periodontal ligament fibers and gingival soft tissues, resulting in loss of attachment and bone resorption. Table 2 provides an overview of the clinical responses to biofilm and host immunity.
WHEN DO BACTERIA INVADE THE TISSUES OF PERIODONTAL POCKETS?
A clear understanding of the periodontium and its related structures is an important foundation for interpreting the advanced stages and characteristics of periodontal disease. These structures withstand the physiological forces of mastication and defend against foreign invaders, such as pathogenic microbes. Over time, inadequate oral hygiene measures can result in microbial and pathologic challenges to the periodontium.
Studies have illustrated the development and progression of gingivitis to periodontal disease. A landmark study demonstrated that subjects who refrained from performing oral hygiene measures developed gingivitis within seven days to 21 days.13 At seven days, the composition of the biofilm bacteria shifted from aerobic Gram-positive species to more virulent Gram-negative organisms. Although reversible, this microbial shift can result in bacterial invasion of the soft tissue, an increase in the body’s immune response, and bleeding on probing,14,15 which, if left untreated, can lead to periodontitis.16
HOW IS THE PERIODONTAL INFECTION RESOLVED?
As noted, treatment of aggressive periodontitis may include the surgical removal of the pocket epithelium and administration of systemic antibiotics due to the potential for tissue invasion by A. actinomycetemcomitans.9 Following successful therapy, a cascade of biochemical-based responses occur that result in a small amount of new periodontal attachment as part of the healing response. More important is that the inflammation is reduced, thereby facilitating anatomic site stability if recurrent infection is prevented. Successfully treated sulci repopulate with microbial communities typical of those found in periodontally healthy patients.17
CONCLUSION
Oral biofilm significantly impacts the initiation and progression of periodontal disease and its repeated removal, both supragingivally and subgingivally, is paramount to improving and maintaining oral health. Encouraging patients to practice effective self-care is also critically important. It should be noted that periodontal maintenance intervals are adjustable and depend on the results of frequent reassessments of oral health status in the context of self-care and previously provided clinical therapies.
References
- Ramjford SP. Maintenance care for treated periodontitis patients. J Clin Periodontol. 1987;14:433–437.
- Osborn JB, Lenton PA, Lunos SA, Blue CM. Endoscopic vs. tactile evaluation of subgingival calculus. J Dent Hyg. 2014;88:229–236.
- Socransky SS, Haffajee AD, Teles R, et al. Effect of periodontal therapy on the subgingival microbiota over a 2-year monitoring period. I. Overall effect and kinetics of change. J Clin Periodontol. 2013;40:771–780.
- Caton J, Proye M, Polson A. Maintenance of healed periodontal pockets after a single episode of root planing. J Periodontol. 1981;53:420–424.
- Smiley CJ, Tracy SL, Abt E, et al. Systematic review and meta-analysis on the nonsurgical treatment of chronic periodontitis by means of scaling and root planing with or without adjuncts. J Am Dent Assoc. 2015;146:508–524.
- Shallhorn RG, Snider LE. Periodontal maintenance therapy. J Am Dent Assoc. 1981;103:227–231.
- Caton JG, Ciancio SG, Blieden TM, et al. Treatment with subantimicrobial dose doxycycline improves the efficacy of scaling and root planing in patients with adult periodontitis. J Periodontol. 2000;71:521–532.
- Lowenguth RA, Chin I, Caton JG, et al. Evaluation of periodontal treatments using controlled-release tetracycline fibers: microbiological response. J Periodontol. 1995;66:700–707.
- Teughels W, Dhondt R, Dekeyser C, Quirynen M. Treatment of aggressive periodontitis. Periodontol 2000. 2014;65:107–133.
- Novaes AB Jr, Schwartz-Filho HO, de Oliveira RR, Feres M, Sato S, Figueiredo LC. Antimicrobial photodynamic therapy in the non-surgical treatment of aggressive periodontitis: microbiological profile. Lasers Med Sci. 2012;27:389–395.
- Mummolo S, Marchetti E, Di Martino S, Scorzetti L, Marzo G. Aggressive periodontitis: laser Nd:YAG treatment versus conventional surgical therapy. Eur J Paediatr Dent. 2008;9:88–92.
- Ioannou I, Dimitriadis N, Papadimitriou K, Sakellari D, Vouros I, Konstantinidis A. Hand instrumentation versus ultrasonic debridement in the treatment of chronic periodontitis: a randomized clinical and microbiological trial. J Clin Periodontol. 2009;36:132–141.
- Löe H, Theilade E, Jensen SB. Experimental gingivitis in man. J Periodontol. 1965;36:177.
- Cobb CM. Clinical significance of nonsurgical periodontal therapy: an evidence-based perspective of scaling and root planing. J Clin Periodontol. 2002;29(Suppl 2):6–16.
- Saglie R, Newman MG, Carranza FA Jr, Pattison GL. Bacterial invasion of gingiva advanced periodontitis in humans. J Periodontol. 1982;53:217–222.
- Schroeder HE, Page RC. Pathogenesis of inflammatory periodontal disease. A summary of current work. Lab Invest. 1976;33:235–249.
- Haffajee AD, Cugini MA, Dibart S, Smith C, Kent RL Jr, Socransky SS. The effect of SRP on the clinical and microbiological parameters of periodontal disease. J Clin Periodontol. 1997;24:324–334.
- Lins RX, de Oliveira Andrade A, Hirata Junior R, Wilson MJ, Lewis MA, Williams DW, Fidel RA. Antimicrobial resistance and virulence traits of Enterococcus faecalis from primary endodontic infections. J Dent. 2013;41(9):779–786.
- Santos, AL, Siqueira, JF Jr., Rôças, IN, et al, Comparing the bacterial diversity of acute and chronic dental root canal infections. PLoS One. 2011;6:e28088.
- Thurnheer T, Belibasakis GN. Integration of non-oral bacteria into in vitro oral biofilms. Virulence. 2015;6(3):258–264.
