

Using d-PTFE Barriers to Enhance Bone and Soft Tissue Regeneration
An exploration of novel clinical applications for dense polytetrafluorethylene barriers.
An exploration of novel clinical applications for dense polytetrafluorethylene barriers
PURCHASE COURSE
This course was published in the July 2017 issue and expires July 2020. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- List various applications for dense polytetrafluorethylene (d-PTFE) barriers in periodontal procedures, and explain clinical considerations for their use.
- Describe using the “ice cream cone technique” with a d-PTFE barrier.
- Identify various factors and timing considerations for therapies involving implant placement for extracted teeth.
A recent paper reviewed research data and demonstrated the use of a dense polytetrafluorethylene (d-PTFE) barrier in conjunction with a bone allograft to regenerate a resorbed bony wall of an extraction socket.1 As the authors noted, the main advantage of this type of barrier is that it facilitates predictable guided bone regeneration in defective sockets without having to attain primary closure.1 Further experimentation with d-PTFE barriers revealed other clinical applications. This article will describe innovative uses of this material. Specifically, d-PTFE barriers can be used to regenerate a defective socket wall without flap elevation, repair an oral antral perforation, and restore a large amount of lost vertical keratinized tissue. The discussion will also address the clinical management of issues that can arise when using d-PTFE barriers.
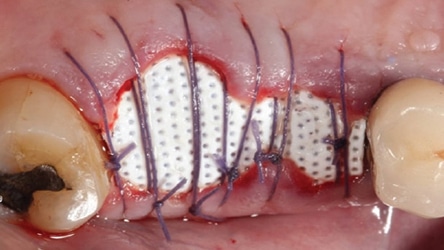
These barriers are marketed under various brand names, such as Cytoplast (Osteogenics Biomedical), TefGen FD (Lifecore Biomedical) and Symbios OsteoShield (Dentsply Sirona). The clinical cases presented in this paper were done with Cytoplast d-PTFE. Featuring a shelf life of four years, the barrier has a shiny side and a dimpled side.2 The shiny side is placed facing bone and the dimpled aspect is directed upward, toward the flap so that fibroblast can adhere to the indentations and provide flap adherence. The pore size of the barriers is 0.2 µm, which makes it impervious to bacteria (that are usually between 1 and 10 µm).2 This helps avoid infections that can occur when expanded-PTFE (i.e., e-PTFE) barriers (with a pore size 30 µm) are employed. Available barrier sizes are 12 mm x 24 mm and 25 mm x 30 mm.2 For molars with large osseous defects, larger barriers are preferable because they provide enough length bucco-lingually to ensure that the barrier can be tucked 4 mm under the flap onto intact bone. Besides suturing, tucking d-PTFE barriers underneath the flaps protects the barriers from becoming dislodged. In this regard, in order to maintain barrier stability, patients are advised not to suck on the barrier location and to refrain from using a water pulsating device. Oral hygiene is performed with a cotton swab and chlorhexidine gluconate at the surgical site until the barrier is removed after four to six weeks.
GUIDED BONE REGENERATION
Guided bone regeneration (GBR) is based on guided tissue regeneration (GTR) principles.3 These concepts include use of barriers to exclude epithelium and connective tissue from invading osseous grafts, and to provide space maintenance and clot stabilization. The endpoint of a GBR procedure is regeneration of bone, whereas GTR is used around teeth to restore bone, periodontal ligament (PDL) and cementum. Previously, primary closure was considered necessary to attain GBR; however, in certain situations (such as a defective socket wall), d-PTFE barriers can help achieve horizontal bone regeneration without primary closure.1 This reduces patient morbidity and accelerates the speed of the GBR procedure. It also helps avoid alterations to the level of the mucogingival junction and shallowing of the buccal vestibule.
BLOOD SUPPLY INTERRUPTION AND BONE LOSS
There are three sources of blood supply to a tooth: PDL, periosteal and endosteal vasculature.4 Upon tooth removal, the blood supply from the PDL is interrupted and, if a flap is raised, the periosteal blood source is also disturbed.5 Accordingly, if a tooth is extracted and a flap is not raised, there is less bone loss than when a tooth is extracted in conjunction with flap elevation. A systematic review by Tan et al6 indicated that if a flap is elevated, the average vertical bone and horizontal bone resorption are 1.24 mm and 3.39 mm (means), respectively.6 In contrast, without flap elevation, the mean vertical bone decrease is 1 mm and the horizontal bone width reduction is 0.9 to 1.2 mm.7 To ensure less bone loss and recession, it is therefore preferable not to raise a buccal flap in the esthetic zone.
HEALING EVENTS SUBSEQUENT TO TOOTH EXTRACTION
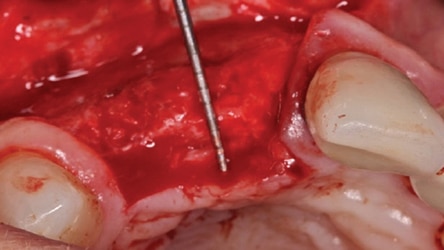
Once a tooth is extracted, a blood clot fills the socket and granulation tissue is formed within 96 hours.8 In seven to 21 days, granulation tissue is converted to connective tissue.8 Osteoid forms after 21 days and this type of connective tissue will be converted to bone as it becomes mineralized.8 Epithelium is avascular and cannot grow across the socket until there is a connective tissue base; thus, it takes epithelium approximately five weeks to cover a socket. After three months, woven bone is present in the socket.1 This immature bone does not have Haversian systems (concentric layers of lamellar bone around a blood vessel). Nevertheless, an implant can usually be placed into woven bone that has formed in a four-walled socket. At an appointment prior to placing an implant, it is prudent to sound the bone by probing with an anesthetic needle to determine osseous hardness. This assessment is performed at different aspects of the regenerated socket (e.g., occlusally, buccally and lingually). If the bone is penetrable, the clinician should wait a few more months for additional mineralization to occur and sound the bone again. Bone continues to mineralize for 12 months.9 After four months, lamellar bone is usually present.1 This is mature bone with Haversian systems. When a socket wall has been regenerated, it is prudent to wait four to six months after the grafting procedure to allow bone mineralization to occur before placing an implant; sometimes, it is necessary to wait longer for bone maturation.
d-PTFE BARRIER REMOVAL
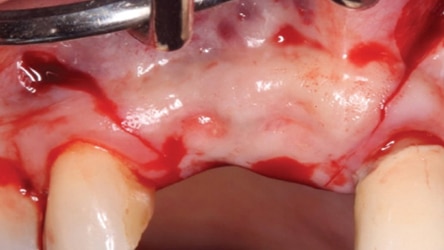
Usually, a d-PTFE barrier is removed four to six weeks after its placement over a bone graft.1 The barrier can be removed with a hemostat or college pliers if it does not dislodge easily. This can be done without anesthetizing the patient. Upon barrier removal, osteoid tissue (red connective tissue) is seen over the bone graft. The epithelium creeps across the connective tissue and begins to turn pink in approximately two weeks. If bone particles remained exposed, nothing needs to be done when the barrier is removed, as they will be covered with soft tissue in one to two weeks.
ICE CREAM CONE TECHNIQUE
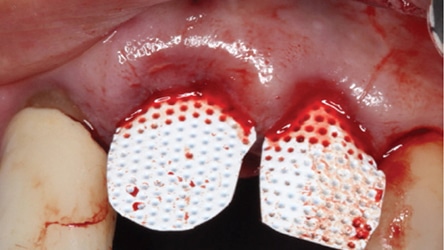
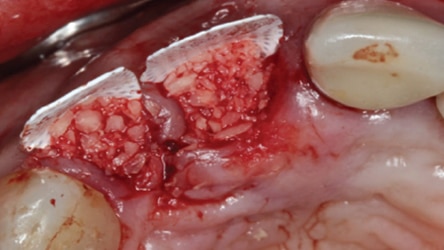
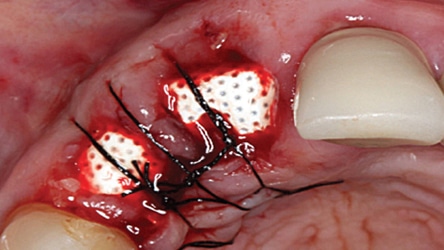
In 2007, Elian et al5 published a procedure that was originally presented by Tarnow,10 which is referred to as the “ice cream cone technique.” Its purpose is to facilitate bone regeneration of a defective bony buccal plate in the esthetic zone without elevating a flap.5,10,11 After a flapless tooth extraction, a resorbable barrier is contoured into a shape like an ice cream cone and inserted into the socket and pushed against the buccal plate of bone. The barrier is not fixed in place on the buccal (other than being inserted into the socket). Next, a bone graft is placed into the socket and the barrier is sutured to the palatal tissue. It is important to note that a resorbable barrier begins to deteriorate within two weeks (due to degradation by salivary enzymes),12 which could result in loss of bone graft material, gingival tissue collapse, or invasion of the graft by connective tissue — thereby precluding graft mineralization. To avoid these dilemmas, the authors use a d-PTFE barrier when employing the ice cream cone technique. The barrier is placed 3 to 4 mm under a small palatal flap to ensure retention. After the barrier is inserted into the socket, a bone graft is placed so it extends 1 to 2 mm coronal to the osseous crest. This facilitates providing a convex, rather than concave, gingival contour at the extraction site when the barrier is removed. Previously, it was suggested that the barrier should be removed after four weeks to provide sufficient time for osteoid tissue to become impenetrable to invading epithelium or fibroblasts.1 However, if bone is placed coronal to the osseous crest, the authors suggest the barrier be left in place for five or six weeks. This allows extra time for bone graft material (placed coronal to the osseous crest) to become covered with osteoid tissue. If the buccal or palatal bony plate is deficient, a minimum of four to six months should be allowed for bone graft mineralization before implant placement. Steps for this procedure are outlined in Figure 1 through Figure 8.


The use of a modified ice cream cone technique is also possible to address buccal defects. Instead of placing the barrier within the socket, a trough can be made under the periosteum on the outer aspect of the buccal plate without opening a flap across papillae. This facilitates placing the barrier on the outer aspect of the buccal and may result in a thicker ridge (when compared to the barrier being placed on the inner aspect of the buccal bony). However, since a partial flap has been elevated, there is an increased risk of recession.

REPAIR OF AN ORAL ANTRAL DEFECT
An oral antral fistula can occur due to several reasons, such as extraction of a tooth with roots penetrating into the sinus, removal of an implant that protrudes into the sinus, or an infection. If an oral antral fistula occurs, usually a pedicle flap is advanced to occlude the opening. However, if a d-PTFE barrier is employed, it is possible to close an opening into the sinus and resolve an oral antral fistula without attaining primary closure.
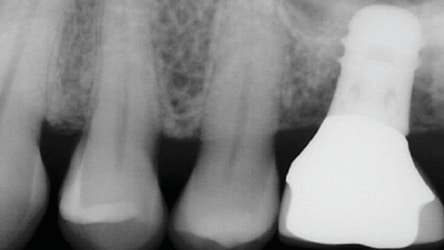


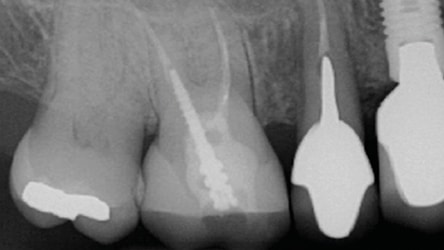
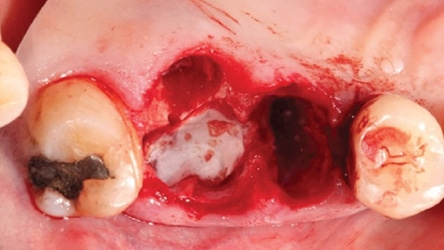
Figure 9 is a radiograph of a patient who presented with a failed mobile implant that protruded into the sinus. It was recognized that upon implant removal there would be a hole into the sinus that would require buccal flap advancement or a palatal pedicle flap to ensure primary closure. The patient had a shallow vestibule, tight musculature and low pain threshold; therefore, it was decided to attempt closure of the perforation into the sinus in a different manner. The technique is illustrated in Figure 10. A full thickness mucoperiosteal flap was elevated buccally and lingually and the implant was removed. After debriding the granulomatous tissue, a resorbable barrier was placed over the hole to the sinus. Next, a bone graft was placed above the resorbable barrier and a d-PTFE barrier was placed over the bone graft. Flap repositioning was performed without attempting to attain primary closure. The barrier was removed after four weeks and osteoid tissue was noted. The patient healed uneventfully. After several months, enough bone was available to perform a transcrestal sinus floor elevation (4 mm). However, the patient elected to have a bridge fabricated to replace #14 (Figure 11). In Figure 12 through Figure 18, this double-barrier technique was used to close a perforation into the sinus associated with extraction of tooth #3.




REGENERATING A LARGE AMOUNT OF VERTICAL KERATINIZED TISSUE
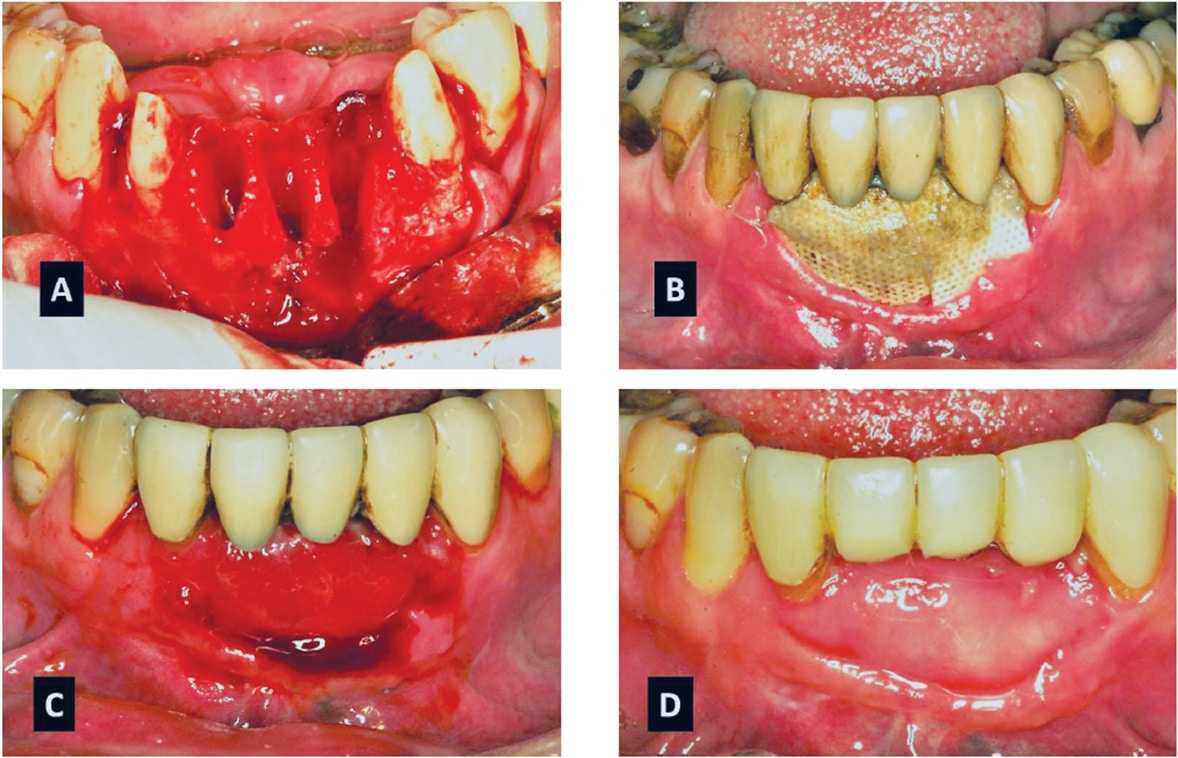
When a d-PTFE barrier is removed, a layer of osteoid is found over the bone graft and epithelium usually grows across the osteoid within two weeks. As noted, osteoid is the connective tissue that becomes mineralized and converts to bone. The ability to regenerate bone and overlying osteoid can be used advantageously when there is a large amount of recession on the buccal of a tooth and the interproximal bone is intact. In this type of situation, it is possible to regenerate a large amount of mucosa and keratinized tissue over the osteoid tissue and eliminate recession — without extrusion of the tooth or flap advancement with gingival augmentation. As shown in Figure 19A, a hopeless maxillary canine (tooth #6) had 6 mm of recession; the tooth was hypermobile, manifested deep periodontal pockets, and was scheduled for extraction. The canine was extracted and a bone graft was covered with a d-PTFE barrier to regenerate bone and overlying tissue (Figure 19B). After five weeks, the barrier was removed and 5 mm of vertical osteoid tissue was noted (Figure 19C). Subsequently, a paracrestal incision was made at the lingual line angles of the adjacent teeth to facilitate transposing additional gingiva to the buccal to fully restore gingival contour. Another example of vertical osteoid tissue that becomes covered with keratinized tissue is seen in Figures 20A through 20D.

Possible issues WITH d-PTFE Utilization
A variety of issues can arise when employing d-PTFE barriers. The following is a description of solutions to several clinical problems and an alternative technique to consider when using d-PTFE barriers.
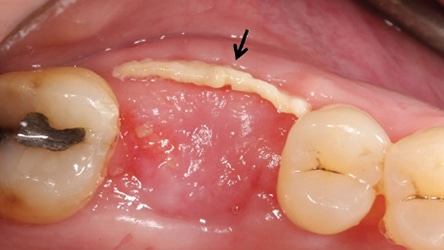
Loose Barrier: If a barrier becomes loose from under the flap on the side of the socket (in situations where no attempt is being made to regenerate a lost wall of a socket), the clinician should trim off the movable part of the barrier. The operator should leave the rest of the barrier submerged for the predetermined time to regenerate a missing plate of bone (Figure 21). This incident does not preclude attaining an excellent result. On the other hand, if the part of the barrier placed to regenerate a resorbed socket wall becomes prematurely loose, the procedure needs to be redone.
Patient Discomfort: When a patient complains that the tissue adjacent to the barrier is uncomfortable and pulsing, it is usually due to premature loss of sutures. This results in a loose flap that needs to be resutured. In this regard, it is advantageous to use nonresorbable Gore-tex sutures. With respect to reducing gingival inflammation adjacent to a barrier, clinicians are advised to avoid curling the barrier edges underneath the facial or lingual flap.
Papilla Retention: If multiple teeth are removed and a d-PTFE barrier is used across several sockets, it is advisable to remove papillae because they do not usually adhere well to d-PTFE material. Furthermore, if they traverse totally across the barrier, they can interfere with barrier removal.
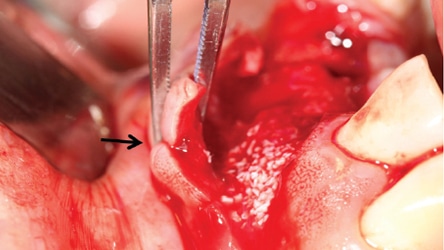
Deep Osseous Defects: In cases with advanced resorption of a buccal bony plate, a facial vertical releasing incision should be made adjacent to the tooth being extracted to gain access to the apical part of the defect and facilitate barrier placement. After the barrier is in place, the clinician should suture the vertical releasing incision first, and add the bone graft to the defective socket. If the bone graft material is added prior to closing the vertical incision, the flap may be distended by the graft and preclude attaining tension-free primary closure of the vertical releasing incision. Vertical releasing incisions should be avoided in the maxillary palatal or mandibular lingual regions to avoid damage to underlying structures.
Avoiding Papilla Height Loss: Papilla-sparing incisions can be used in the esthetic zone or adjacent to an implant to facilitate barrier placement and help avoid loss of papillary height (Figure 7).13
Managing Gingival Troughs: When a barrier is left in place for a long period (e.g., seven or eight weeks), the epithelium invaginates along its periphery and forms a trough between the flap and barrier (Figure 22). Subsequently, when the barrier is removed, the connective tissue (i.e., osteoid tissue) faces invaginated epithelial tissue and these surfaces will not adhere to each other. To correct this situation, clinicians should insert a diamond bur into the trough and create bleeding points along the epithelial tissues (i.e., expose connective tissue) and suture the opposing surfaces together.
CONCLUSION
This paper discusses the versatility of d-PTFE barriers and presents novel techniques to enhance patient treatment. Procedures such as vertical or horizontal augmentation beyond the alveolar housing using d-PTFE barriers without primary closure are interesting concepts that need to be further explored.
REFERENCES
- Greenstein G, Carpentieri JR. Utilization of d-PTFE barriers for post-extraction bone regeneration in preparation for dental implants. Compend Contin Educ Dent. 2015;36:465–473.
- Cytoplast Regeneration Products Catalog. Available at: osstem.de/data/library/2014enCytoplast.pdf. Accessed June 12, 2017.
- Bashutski J, Oh TJ, Chan HL, Wang HL. Guided tissue regeneration: a decision-making model. J Int Acad Periodontol. 2011;13:48–57.
- Al-Sabbagh M. Complications in implant dentistry. Dent Clin North Am. 2015;59:8–15.
- Elian N, Cho SC, Froum S, Smith RB, Tarnow DP. A simplified socket classification and repair technique. Pract Proced Aesthet Dent. 2007;19:99–104.
- Tan WL, Wong TL, Wong MC, Lang NP. A systematic review of post-extraction alveolar hard and soft tissue dimensional changes in humans. Clin Oral Implants Res. 2012;23(Suppl 5):1–21
- Lee CT, Chiu TS, Chuang SK, Tarnow D, Stoupel J. Alterations of the bone dimension following immediate implant placement into extraction socket: systematic review and meta-analysis. J Clin Periodontol. 2014;41:914–926.
- Amler MH. Age factor in human alveolar bone repair. J Oral Implantol. 1993;19:138–142.
- Minichetti JC, D’Amore JC, Hong AY, Cleveland DB. Human histologic analysis of mineralized bone allograft (Puros) placement before implant surgery. J Oral Implantol. 2004;30:74–82.
- Tarnow D. Ice cream cone technique. Lecture American Academy of Periodontics. 2000.
- Tan-Chu JH, Tuminelli FJ, Kurtz KS, Tarnow DP. Analysis of buccolingual dimensional changes of the extraction socket using the “ice cream cone” flapless grafting technique. Int J Periodontics Restorative Dent. 2014;34:399–403.
- Soldatos NK, Stylianou P, Koidou VP, Angelov N, Yukna R, Romanos GE. Limitations and options using resorbable versus nonresorbable membranes for successful guided bone regeneration. Quintessence Int. 2017;48:131–147.
- Greenstein G, Tarnow D. Using papillae-sparing incisions in the esthetic zone to restore form and function. Compend Contin Educ Dent. 2014;35:315–322.
From Decisions in Dentistry. July 2017;3(7):46–51.

