
 FUNKYNATSUKI, VIA WIKIMEDIA COMMONS
FUNKYNATSUKI, VIA WIKIMEDIA COMMONS
Understanding And Managing Gingival Recession
Proper prevention, treatment and maintenance are integral to achieving positive outcomes for patients with gingival recession.
PURCHASE COURSE
This course was published in the July 2022 issue and expires July 2025. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the July 2022 issue and expires July 2025. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Explain gingival recession and its prevalence, as well as site and patient-related risk factors.
- Discuss indications for covering exposed root surfaces or treating deficient bands of attached keratinized tissue.
- Educate this patient cohort regarding proper self-care practices when there is existing recession and associated dentinal hypersensitivity.
A lack of attached keratinized tissue and gingival recession are the most common soft tissue conditions encountered by the dental team. In fact, 50% to 80% of adults present with at least one site of recession.1 Exposed root surfaces compromise esthetics and function, leading to an unfortunate sequela of dentinal hypersensitivity, caries, noncarious cervical lesions, and/or impaired plaque control. If these defects are not treated aptly, they can worsen and complicate future surgical, restorative or orthodontic treatment.2
Mucogingival therapy has evolved with newer grafting materials and techniques. The surgical approach is unique to each patient and differs by etiology of the condition, oral hygiene compliance, and other risk factors. It is important for oral healthcare teams to understand preventive and maintenance practices designed to stop the occurrence and progression of gingival recession. Such knowledge will improve chairside patient education, including self-care instructions intended to prevent further attachment loss.
Gingival recession is the apical shift of the gingival margin from the cementoenamel junction.3 Recession can result from bacterial, anatomical, chemical or mechanical trauma, but the presence of inflammation and bone loss are what truly drives this process (Table 1).3 The influences of a patient’s phenotype are also considered. Dehiscence and recession more frequently occur in patients with thin phenotypes, especially following orthodontic treatment.4 If a probe is visualized through the facial gingival sulcus, the patient is classified as a thin phenotype.5 This should be documented as part of the initial workup, as it may complicate treatment. 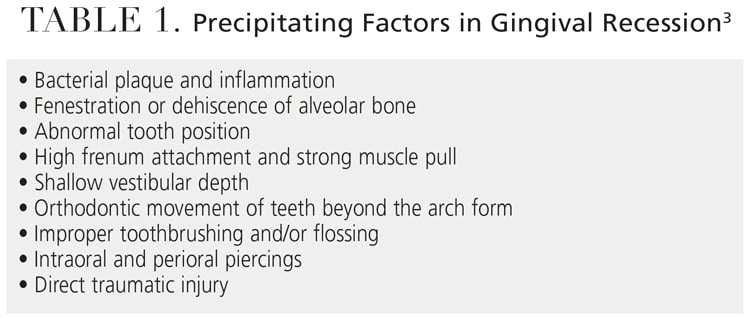
MATERIALS AND TECHNIQUES
Today, a variety of materials and techniques are used to minimize recession. A systematic review of 48 randomized clinical trials with short- and long-term follow-ups found that connective tissue grafts, combined with coronally advanced flaps, best managed single and multiple recession defects, resulting in the most significant gains in attachment, keratinized tissue width, and root coverage.6 This is often considered the gold standard in root coverage procedures.

In this same study, chemical root modification and the type of mechanical debridement did not affect therapeutic outcomes.6 Chemical agents, including ethylenediaminetetraacetic acid, can be used to decontaminate the root surface, remove the smear layer, and expose the dentinal tubules for improved connective tissue reattachment.7 They can be cytotoxic to wound-healing cells at specific concentrations, however, and should be applied in the appropriate indications.7
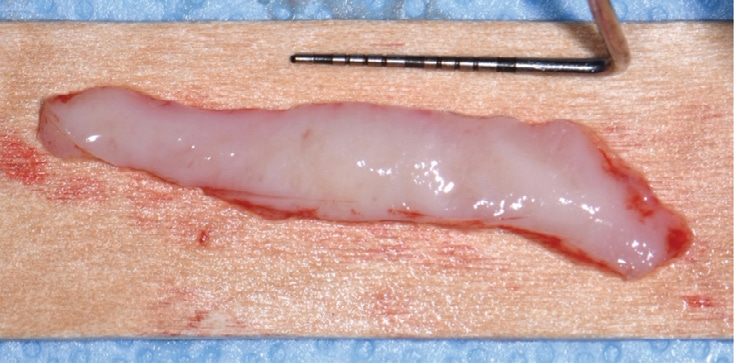
The connective tissue graft is harvested from the palate in a single incision, underneath the overlying epithelium, or de-epithelialized after removal from the donor site. It is then introduced to the recipient site as part of a coronally advanced or rotated flap or tunnel (Figure 1 and Figure 2).6 The use of nonautogenous materials, such as allografts or xenografts, provides a viable alternative to the connective tissue graft to reduce patient comorbidities.6 Table 2 includes a list of available materials and techniques.
Growth factors, including platelet-derived growth factor and bone morphogenetic protein, can also be used to accelerate healing. They stimulate the chemotaxis, mitogenesis, and matrix formation of wound-healing cells.6 Another molecular mediator, enamel matrix derivative, contains different proteins and enzymes from developing pig enamel and enhances fibroblast recruitment, adhesion and angiogenesis.8 These products can hydrate grafts and matrices extraorally, or be used directly at the recipient site.

Caries, lesions or cervical restorations may affect root coverage procedures. Noncarious cervical lesions vary in appearance and result from abrasion, erosion and corrosion from marginal restorations. The decision to graft or restore noncarious cervical lesions is often debated. If the lesion extends more than 2 mm into the root surface, it should be restored.9 The lesion’s depth and shape, root convexity, thickness, amount of attached tissue present, and esthetic interests should all be considered.9 Root reshaping with burs or hand instruments shortens the distance cells need to travel for graft vascularization.10 These defects, along with root caries and compromised restorative margins, should be diagnosed and treated before surgery.
If left untreated, recession can worsen to the depth of the mucogingival junction and compromise the band of attached keratinized tissue. The 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions did not numerically specify the amount or thickness of keratinized tissue needed to maintain health. However, tissue that is not inflamed, minimizes further recession, and supports patient comfort, esthetics and oral hygiene should be considered healthy.3 With this in mind, ongoing recession warrants clinical treatment.
A wide band of keratinized tissue is protective against future recession, and more so in patients with poor oral hygiene who are noncompliant with recare. This was observed in a split-mouth study in which grafted sites that were not maintained for five years were still free of inflammation.11 According to a meta-analysis, the amount of keratinized tissue at the initial recare visit ranks among the most important indicators of long-term marginal stability.12 Keratinized tissue width should therefore be recorded as part of a comprehensive evaluation. This can be manually charted or imported with an intraoral scanner.
In cases in which a gain in keratinized tissue width is the goal, a free soft tissue autograft or free gingival graft is preferred.13 A 1- to 2-mm-thick graft that includes epithelium and connective tissue is harvested from the palate. The donor site is sutured with a hemostatic agent, and a plastic palatal stent is delivered for immediate hemostasis. The graft is transplanted and secured to a recipient site deficient in attached keratinized tissue (Figure 3 through Figure 5). Approximately 44% to 58% shrinkage is expected over the grafted area, mainly in the first 30 days.14 This is commonly performed at low-esthetic-risk sites. Nonautogenous materials also work well when there is concern for donor site anatomy, postoperative discomfort, or treatment of multiple defects.15

While patients should not initially anticipate root coverage with this procedure, a phenomenon called creeping attachment occurs from 30 days to one year after surgery. The coronal migration of the gingival sulcus is about 0.8 mm on average and can, in turn, cover exposed roots, especially in areas of narrow, shallow recession.16 Setting appropriate clinical expectations is important. Tooth malposition, high frenum attachment, strong muscle pull, shallow vestibule, and other anatomical factors can predispose patients to mucogingival problems and negatively affect therapeutic outcomes (Figure 6).
The timing of any orthodontic, restorative and/or implant treatment should be outlined in the treatment planning phase. For example, gingival augmentation may be needed to minimize recession when teeth are moved beyond their normal alveolar housing to establish proper occlusal relations.4 A best-evidence consensus showed that 20% to 25% of patients develop mucogingival defects within five years of orthodontic treatment.4 While recession can at least be maintained with regular prophylaxis and proper self-care, patients must understand the treatment objectives and potential complications of interdisciplinary care. They should also be alerted to the added time and treatment expense required.

PREVENTION AND MAINTENANCE
As part of the initial recall, oral hygiene technique should be reviewed. Studies show that improper toothbrushing can harm gingival tissues, with brushing pressure and bristle type serving as the most important determinants.17 In fact, a hard bristle toothbrush was used in the vast majority of dentinal hypersensitivity cases.18 Patients should use a soft toothbrush or a power toothbrush with a pressure indicator. Evidence suggests these tools help minimize aggressive brushing patterns.2 Technique and angulation affect plaque removal regardless of the toothbrush type. Proper oral hygiene reduces bacterial load and inflammation, which, in turn, mitigates discomfort and attachment loss.2
Selecting the proper dentifrice is equally important in patients with sensitivity concerns. The relative dentin abrasivity (RDA) value measures the abrasiveness of toothpaste. This value is directly related to dentin loss, which contributes to dentinal hypersensitivity. Although this presentation is multifactorial, using a toothpaste with a low RDA can help minimize its symptoms and progression.18 Toothpaste with an RDA value of 0 to 70 is categorized as “low abrasion” and should be recommended to patients with existing sensitivity or exposed root surfaces.18

Patients should also consider a toothpaste with ingredients such as calcium sodium phosphosilicate, arginine and calcium carbonate, strontium, or potassium nitrate. These agents depolarize the nerves or block dentinal tubules, thereby decreasing nerve conduction and hypersensitivity.2 Because of the different mechanisms by which sensitivity-relief toothpastes work, patients may need to try several first or use them for weeks at a time before finding one that alleviates symptoms. For some patients, a high-fluoride concentration-toothpaste may also prove beneficial.18
When surgery is pursued, patients should establish regular recare appointments, in addition to the recommended postoperative follow-ups with their specialist. Significantly greater root coverage and better long-term marginal stability were achieved in patients who followed up with the treating surgeon compared to the general dentist.19 Furthermore, evidence suggests patients who have undergone surgery benefit from an alternating maintenance schedule between their general dentist and periodontist.19 At each visit, a periodontal exam, prophylaxis and evaluation by the dentist should take place. The aforementioned tools and habits should be reinforced at each visit, and regular maintenance and proper oral hygiene stressed as the key to long-term treatment success.

If patients are not surgical candidates due to medical or financial limitations, their symptoms can still be managed during recare visits. Fluoride varnish application provides longer relief than the potassium nitrate found in many sensitivity-relief toothpastes.2 Laser therapy is a more novel approach to relieving hypersensitivity and includes low- and mid-output-power lasers, such as diode, Nd:YAG, Er:YAG and CO2,18 although their exact mechanism of action is unknown. Each laser affects the tissues differently, depending on its wavelength, power density and mode. It is assumed they provide an analgesic effect by occluding the dentinal tubules when used directly over the tooth surface.20 However, a weak association exists with this technology given its strong placebo effect in which patients feel immediate relief afterward.21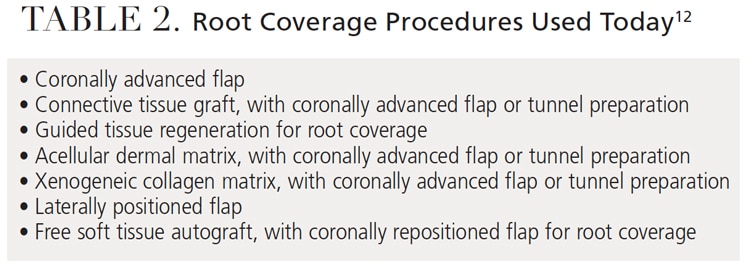
CASE REPORT
This case outlines the steps taken to correct a complete lack of attached tissue thickness and amount by means of a free gingival graft. A 29-year-old woman was concerned about worsening recession (Figure 7 through Figure 9). The patient had no significant medical history. After a patient evaluation and review of varying techniques and materials, a surgical treatment plan was developed and consents were obtained. The treatment plan included a free gingival graft at sites #24 to 25 using an enamel matrix-derived growth factor and a coronally repositioned flap to obtain root coverage.22 After initial findings were charted both manually and with an intraoral scan, an increase in keratinized tissue width was deemed the primary goal. The patient had a shallow vestibule, absent attached tissue around #24 and 25, thin phenotype, labial tooth position at #25 due to ongoing orthodontic treatment, and fair oral hygiene. Complete root coverage was not initially guaranteed due to these site-related risk factors.

The recipient site was carefully prepared with partial-thickness dissection from #24 to 25 and distal oblique vertical releases. A free gingival graft measuring 8 mm long by 10 to 12 mm wide by 1.5 mm thick was harvested from the right palate, trimmed to remove excess adipose tissue, and hydrated in an enamel matrix-derived growth factor. Ethylenediaminetetraacetic acid root surface conditioner (24% concentration) was used over #24 and 25 before applying the growth factor. The graft was secured and stabilized at the #24 to 25 site with simple interrupted, nonresorbable sutures. Gauze pressure was applied to the palatal wound and multiple layers of hemostatic gauze were placed and sutured along the donor site for profound hemostasis. A palatal stent was delivered to further minimize postoperative bleeding risk, and a periodontal dressing was placed over the recipient site. The patient was discouraged from looking at or manipulating the operated sites for at least two weeks.
The patient returned for weekly follow-ups and was initially maintained by the specialty practice. Proper oral hygiene techniques were demonstrated at each visit to establish better self-care. A power toothbrush with a pressure indicator was recommended. The recipient site was scaled and polished as needed. Further root coverage can reasonably be expected during this time owing to the gradual and coronal reformation of the gingival sulcus. She will finish her orthodontic treatment and alternate prophylaxis every six months with her general dentist and periodontist. The patient denied any esthetic or sensitivity concerns following treatment.

SUMMARY
Procedures to cover exposed roots or increase keratinized tissue width have evolved over time. Site- and patient-related risk factors should be discussed as part of the initial exam, especially if interdisciplinary treatment is planned. Gingival recession can be treated successfully when identified early. Esthetic concerns, sensitivity and worsening recession are important indications for surgical treatment. Throughout the care continuum, a coordinated clinical team plays an important role in the prevention and maintenance of mucogingival defects.
REFERENCES
- Kassab MM, Cohen RE. The etiology and prevalence of gingival recession. J Am Dent Assoc. 2003;134:220–225.
- Imber JC, KasaJ A. Treatment of gingival recession: When and how? Int Dent J. 2021;71:178–187.
- Cortellini P, Bissada NF. Mucogingival conditions in the natural dentition: narrative review, case definitions, and diagnostic considerations. J Periodontol. 2018;89(Suppl 1):S204–S213.
- Kao RT, Curtis DA, Kim DM, et al. American Academy of Periodontology best evidence consensus statement on modifying periodontal phenotype in preparation for orthodontic and restorative treatment. J Periodontol. 2020;91:289–298.
- De Rouck T, Eghbali R, Collys K, De Bruyn H, Cosyn J. The gingival biotype revisited: transparency of the periodontal probe through the gingival margin as a method to discriminate thin from thick gingiva. J Clin Periodontol. 2009;36:428–433.
- Chambrone L, Salinas Ortega MA, Sukekava F, et al. Root coverage procedures for treating localised and multiple recession-type defects. Cochrane Database Syst Rev. 2018;10:CD007161.
- Blomlöf JP, Blomlöf LB, Lindskog SF. Smear layer formed by different root planing modalities and its removal by an ethylenediaminetetraacetic acid gel preparation. Int J Periodontics Restorative Dent. 1997;17:242–249.
- Gestrelius S, Lyngstadaas SP, Hammarström L. Emdogain-periodontal regeneration based on biomimicry. Clin Oral Investig. 2000;4:120–125.
- Allen EP, Winter RR. Interdisciplinary treatment of cervical lesions. Compend Contin Educ Dent. 2011;32:16–20.
- Gordon HP, Sullivan HC, Atkins JH. Free autogenous gingival grafts. II. Supplemental findings — histology of the graft site. Periodontics. 1968;6:130–133.
- Kennedy JE, Bird WC, Palcanis KG, Dorfman HS. A longitudinal evaluation of varying widths of attached gingiva. J Clin Periodontol. 1985;12:667–675.
- Tavelli L, Barootchi S, Cairo F, Rasperini G, Shedden K, Wang HL. The effect of time on root coverage outcomes: a network meta-analysis. J Dent Res. 2019;98:1195–1203.
- Kim DM, Neiva R. Periodontal soft tissue non-root coverage procedures: a systematic review from the AAP regeneration workshop. J Periodontol. 2015;86:S56–S72.
- Silva CO, Ribeiro Edel P, Sallum AW, Tatakis DN. Free gingival grafts: graft shrinkage and donor-site healing in smokers and non-smokers. J Periodontol. 2010;81:692–701.
- Dai A, Huang JP, Ding PH, Chen LL. Long‐term stability of root coverage procedures for single gingival recessions: a systematic review and meta‐analysis. J Clin Periodontol. 2019;46:572–585.
- Matter J, Cimasoni G. Creeping attachment after free gingival grafts. J Periodontol. 1976;47:574–579.
- Addy M, Hunter ML. Can toothbrushing damage your health? Effects on oral and dental tissues. Int Dent J. 2003;53:177–186.
- Clark D, Liran L. Nonsurgical management of tooth hypersensitivity. Int Dent J. 2016;66:249–256.
- McGuire MK, Scheyer ET, Snyder MB. Evaluation of recession defects treated with coronally advanced flaps and either recombinant human platelet-derived growth factor-BB plus β-tricalcium phosphate or connective tissue: comparison of clinical parameters at 5 years. J Periodontol. 2014;85:1361–1370.
- Matsumoto K, Kimura Y. Laser therapy of dentin hypersensitivity. J Oral Laser Application. 2007;7:7–25.
- Sgolastra F, Petrucci A, Gatto R, Monaco A. Effectiveness of laser in dentinal hypersensitivity treatment: a systematic review. J Endod. 2011;37:297–303.
- Bernimoulin JP, Lüscher B, Mühlemann HR. Coronally repositioned periodontal flap. Clinical evaluation after one year. J Clin Periodontol. 1975;2:1–13.
From Decisions in Dentistry. July 2022;8(7)30-33.

