
 LUCHSCHEN / ISTOCK / GETTY IMAGES PLUS
LUCHSCHEN / ISTOCK / GETTY IMAGES PLUS
Precision Dentistry in Practice
Personalized dental medicine helps improve outcomes while also reducing the cost of care.
PURCHASE COURSE
This course was published in the July 2022 issue and expires July 2025. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the July 2022 issue and expires July 2025. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify the prevalence of oral disease in the United States.
- Define precision medicine and precision dentistry.
- Note the progress in expanding precision dentistry and explain
the additional steps necessary to further its implementation.
In spite of significant advances in science and medicine, the rates of oral disease in the United States (including caries, periodontal disease, and head and neck cancer) are staggering: 47.2% of adults ages 30 and older have some form of periodontal disease, and more than 90% of adults ages 20 and older have had at least one caries lesion.1 Dental caries is rampant in the nation’s children, as well, with 57% of adolescents ages 12 to 19 having experienced caries in their permanent teeth.1 Cases of head and neck cancers, however, have been steadily declining for the past 20 years.2 Additionally, the United States has an access-to-care problem, with persistent oral health disparities.3,4
A paradigm shift is necessary to improve healthcare delivery and outcomes. Precision medicine and precision dentistry may be able to shift the burden of disease and improve the nation’s oral and overall health.
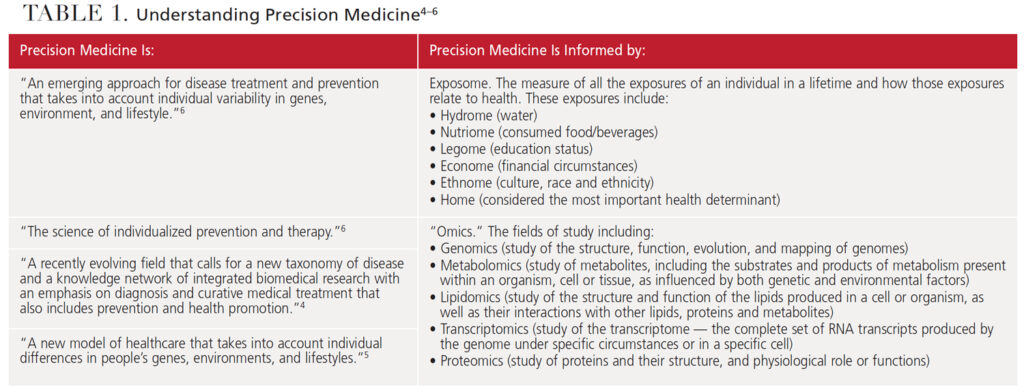
Precision medicine, also referred to as personalized medicine, is modernizing and improving the U.S. healthcare system. This advanced form of care refers to the use of personal data and biomarkers to create protocols and treatments that improve health outcomes (Table 1).4–6 It is a departure from the current, one-size-fits-all paradigm that focuses on treating disease instead of enhancing wellness. The National Institutes of Health (NIH) defines precision medicine as “an emerging approach for disease treatment and prevention that takes into account individual variability in genes, environment, and lifestyles.”5 Scientists and oral healthcare advocates suggest that health can be maintained and disease avoided by creating personalized interventions that consider an individual’s specific genes and biomarkers, as well as environmental factors.7
Precision dentistry is a data-driven approach that classifies patients into subgroups that allow tailored treatments and interventions.8,9 The success of this approach depends on its ability to be predictive, preventive, personalized and participatory.
Overlapping similarities exist between precision medicine and personalized medicine. Much like precision medicine, personalized medicine involves tailoring medical treatment to the individual characteristics of each patient. Risk assessment, prevention, early detection, and accurate diagnosis, treatment and management are hallmarks of both personalized and precision medicine. The term “personalized medicine” seems to insinuate that drugs or medical devices are created specifically for a patient. The term “precision medicine” more accurately captures the concept as accurate and precise. Since the introduction of the Precision Medicine Initiative research project in 2018, the term personalized medicine is used less in favor of precision medicine. These descriptions are often used interchangeably in the literature, however.
PRECISION MEDICINE INITIATIVE
Demonstrating the strength of this country’s commitment to precision medicine, President Obama launched the Precision Medicine Initiative in 2015. A foundational part of this effort is the “All of Us” study, the largest longitudinal study ever conducted in the United States. It seeks to enroll 1 million Americans and examine the effects of environment, lifestyle and biology on human health.
The 10-year study, which began in 2018, is groundbreaking for other reasons, as well. First, its main focus is to enroll participants who are traditionally underrepresented in health research, such as ethnic minorities, those with cognitive impairments, and medically underserved populations.5 Second, in order to fulfill its mandates, new technologies and information technology infrastructure had to be created to gather and analyze the data collected. Precision medicine requires the use of advanced hardware and concepts, such as knowledge discovery, data mining (algorithms that find patterns in the information), natural language processing (analyzing free-form text entered into electronic health records [EHRs], and discovering patterns in the data).4 Third, participants are required to play an active role in the study by contributing data freely (including DNA samples and other biologic specimens), agreeing to ongoing accessibility of their EHRs, sharing results of clinical and behavioral assessments, and participating in mobile health activities to collect geospatial and environmental data.5 Such participation requires researchers to gain patients’ trust and cooperation in order to meet the study’s goals.
Some challenges to the “All of Us” study include ensuring participants’ privacy and addressing concerns regarding exacerbation of health disparities due to availability of technology. Historically, individuals of low socioeconomic status have not benefitted from technological advances as much as those with higher socioeconomic status.4
One of the key challenges is the lack of data on minority populations. Unless data are gathered on these populations, the genetic technologies available will be implemented in ways that perpetuate and even widen health disparities. The effectiveness of genomic therapies relies on the availability of genetic data. As the diversity of the American population is so vast, data on all groups are necessary to create effective treatments. Currently, people of non-European ancestry are underrepresented in the genetic databases on which researchers base their studies.
In 2021, Oral Health in America: Advances and Challenges was released by the NIH. The report provides updates on the findings of the 2000 study, Oral Health in America: A Report of the Surgeon General. It notes that oral health inequity remains 20 years later, and key areas of research should be identified in order to improve the oral health of all Americans.10 Section 6 of the report, “Emerging Science and Promising Technologies to Transform Oral Health,” reviews the findings made possible by technology, such as web-based human oral microbiome databases (e.g., the Human Oral Microbiome Database and CORE database). It also increases researchers’ ability to conduct clinically relevant studies by identifying new species, biomaterials and nanotechnologies, as well as advances in regenerative periodontal medicine.
New approaches based on these advances must be well planned, grounded in scientific evidence, and equitable.10 Active recruitment for the “All of Us” study is ongoing, and researchers are seeking to enroll minority populations. For more information and to participate, visit joinallofus.org.
PERSONALIZED CARE IN ACTION
The ZOE 2.0 study is a large-scale, genetic epidemiologic study of early childhood caries conducted among a community-based sample of preschool-age children enrolled in Head Start centers in North Carolina. This NIH-funded study was conducted in phases, with data collection occurring from August 2016 to February 2019. Recognizing the need for high-fidelity, large-scale information to support precision medicine approaches, the researchers identified six major building blocks necessary to further precision dentistry:11
- Phenotype definition and measurements
- Accounting for, and operationalization of, proximal and distal influences
- Leveraging big data
- Development and utilization of health and disease biomarkers
- Training of precision-health-minded dental professionals
- Advocacy for investments in science, technology, education and policy change
Data collection will include:11
- Administrative data, including public health insurance claims and EHRs
- Caregiver reports, such as children’s oral health status, diet, dental attendance and medication use
- Clinical measures — for example, caries experience, occlusion, dental trauma, and behavior/cooperation
- Genome, including the microbiome
- Family history and demographics, such as age, race/ethnicity, education, and systemic and oral health status
- Imaging
- Environmental exposures — fluoride would be one example
- Geographical and community characteristics
FISHER-OWENS FRAMEWORK
One of the challenges to applying precision medicine is the lack of large-scale valid studies from which to create models. Several reasons account for this issue, including a lack of research methodologies that balance bias and variance. The University of California, San Francisco, has developed the Fisher-Owens framework to conceptualize child, family and community influences on children’s oral health outcomes. Researchers sought to create a framework that would reduce confounding, a major concern when comparison groups are not randomized. Comparable dental patient groups were successfully created by evaluating the need for, and feasibility of, matching; considering various matching methods; and evaluating matching quality.12 The Fisher-Owens framework illustrates the complexity of precision medicine and necessity for valid, reliable data from which to build multifactorial, multilevel conceptual frameworks.
PERIODONTAL DISEASE
Precision dentistry is key to periodontal care, as periodontitis results from a highly individualized sequence of events derived from environmental, genetic and epigenetic factors. The pathogenic biofilm present in periodontitis induces an inflammatory host response in which epigenetic and environmental factors alter gene expressions not encoded in the DNA sequence. These alterations cause a remodeling of the chromatin and activate or inactivate genes. Smoking, for example, is a powerful epigenetic factor (primarily via DNA methylation). Genome-wide association studies have identified variants in at least 65 genes involved in periodontal disease initiation and progression. Additionally, researchers have discovered four shared genetic loci between periodontal disease and atherosclerotic cardiovascular disease (CDKN2B‐AS1, VAMP3, VAMP8 and PLG).13 This suggests periodontitis and atherosclerotic disease are not only causally linked, but also share a similar inflammatory track.13
In support of these scientific advances, the American Academy of Periodontology and European Federation of Periodontology developed a new model of periodontal and peri-implant disease classification in 2017 (see “Decision Points in Periodontal Therapy,” page 26). Four stages indicate the severity of disease and complexity of case management. The model also includes a grading system that gauges disease progression, which depends on biological factors, such as predicted rate of progression, individual risk factors and potential health threats.9
The Periodontal Profile Class Model, also introduced in 2017, utilizes a latent class analysis system. The hallmark of this analysis is the use of data-driven multidimensional disease patterns, as opposed to traditional disease classification (e.g., mild, moderate or severe) that only classifies disease state and does nothing to prevent disease. The Periodontal Profile Class Model lists seven types of periodontal statuses and includes such factors as teeth that are healthy or have recession, presence of crowns, high gingival index, and a reduced periodontium.9,13,14
In a systematic review by Baima et al,15 more than 40 metabolites were found in periodontitis sites. These included malondialdehyde, generated by the peroxidation of membrane polyunsaturated fatty acid and a biomarker for oxidative stress, and 8-hydroxy-deoxyguanosine, a measurement of endogenous oxidative DNA damage and a risk factor for many diseases, including cancer.
BIG DATA
The absence of evidence-based clinical practice guidelines, integration of massive data sets, and adoption of new knowledge as the standard of care are three major challenges to the full implementation of precision dentistry.7 The Institute of Medicine has introduced the Learning Healthcare System, which aligns “science, informatics, incentives and culture” to improve healthcare delivery via the use of big data.7
Efforts to aggregate that data include:
- BigMouth Dental Data Repository, which uses de-identified EHR data contributed by dental schools
- Consortium for Oral Health Related Informatics, which includes a data repository involving more than 20 dental schools
- National Dental Practice-Based Research Network, which collects data from practicing oral health professionals and academicians
The data from clinical trials are also adding to big data repositories. These massive amounts of data are analyzed in four domains: sociobehavioral, educational, clinical and translational science. The end goal is to recognize clinical disease phenotypes and create guidelines to effectively manage them.
PRECISION MEDICINE IN DENTAL EDUCATION
Previous educational paradigms will not facilitate the expansion of precision medicine and dentistry. Successful implementation requires changes in practice patterns and management strategies for oral health professionals. Zheng et al6 studied the development of personalized dentistry in the curricula of North American dental schools and discovered that while the majority of respondents believed it should be taught, most had yet to include it in their didactic curricula. Additionally, the researchers discovered that when precision dentistry was included, it was done as nongenetics-based diagnostics (e.g., caries risk assessment), as opposed to genetics-based methodologies (e.g., salivary diagnostics).
CONCLUSION
Precision medicine and dentistry hold promise for improving healthcare delivery while also reducing costs. This approach relies on EHRs, genetic and molecular data, big data analytics, supercomputing, and the social determinants of health, along with the collaboration of clinicians, researchers, bioinformaticians, data scientists, and, most importantly, patients. Successful implementation of precision dentistry requires training of “precision-minded” practitioners.13 Thus, expansion of this model will require the incorporation of these concepts and frameworks in dental educational curricula.
Currently, little scientific research is available to support the use of precision dentistry in clinical practice.13 This is understandable, as genomics in oral healthcare is in its infancy, and more genome-wide association studies are needed in order for precision dentistry to become the standard of care. Fortunately, the paradigm shift toward personalized care continues to gain momentum and acceptance by patients, practitioners, researchers, and other stakeholders in the nation’s healthcare system.
REFERENCES
- U.S. Centers for Disease Control and Prevention. Oral Health: Cavities. Available at: https://www.cdc.gov/oralhealth/fast-facts/cavities/index.html. Accessed June 1, 2022.
- American Cancer Society. Key Statistics for Oral Cavity and Oropharyngeal Cancers. Available at: https://www.cancer.org/cancer/oral-cavity-and-oropharyngeal-cancer/about/key-statistics.html/www.cdc.gov/oralhealth/fast-facts/cavities/index.html. Accessed June 1, 2022.
- Slavkin HC. From high-definition precision healthcare to precision public oral health: opportunities and challenges. J Public Health Dent. 2020;80:S23–S30.
- Gansky SA, Shafik S. At the crossroads of oral health inequities and precision public health. J Public Health Dent. 2020;80:S14–S22.
- Sankar PL, Parker LS. The Precision Medicine Initiative’s All of Us research program: an agenda for research on its ethical, legal, and social issues. Genet Med. 2017;19:743–750.
- Zheng LY, Rifkin BR, Spielman AI, London L, London SD. The teaching of personalized dentistry in North American dental schools: changes from 2014 to 2017. J Dent Educ. 2019;83:1065–1075.
- Finkelstein J, Zhang F, Levitin SA, Cappelli D. Using big data to promote precision oral health in the context of a learning healthcare system. J Public Health Dent. 2020;80:S43–S58.
- Bartold PM. Personalized/precision dentistry — the future of dentistry? Aust Dent J. 2017;62:257.
- Beck JD, Philips K, Moss K, Divaris K, Morelli T, Offenbacher S. Advances in precision oral health. Periodontol 2000. 2020;82:268–285.
- National Institute of Dental and Craniofacial Research. Oral Health in America: Advances and Challenges. Available at: https://www.nidcr.nih.gov/research/oralhealthinamerica. Accessed June 1, 2022.
- Divaris K, Joshi A. The building blocks of precision oral health in early childhood: the ZOE 2.0 study. J Public Health Dent. 2020;80:S31–S36.
- Fisher-Owens SA, Gansky SA, Platt LJ, et al. Influences on children’s oral health: a conceptual model. Pediatrics. 2007;120:e510–e520.
- Divaris K, Moss K, Beck JD. Biologically informed stratification of periodontal disease holds the key to achieving precision oral health. J Periodontol. 2020;91:S50–S55.
- Loos BG, Van Dyke TE. The role of inflammation and genetics in periodontal disease. Periodontol 2000. 2020;83:26–39.
- Baima G, Corana M, Iaderosa G, et al. Metabolomics of gingival crevicular fluid to identify biomarkers for periodontitis: a systematic review with meta‐analysis. J Periodontal Res. 2021;56:633–645.
From Decisions in Dentistry. July 2022;8(7)34-36,39.

