
 MICROGEN/ISTOCK/GETTY IMAGES PLUS
MICROGEN/ISTOCK/GETTY IMAGES PLUS
Three Techniques for Mandibular Block Anesthesia
The conventional block, Vazirani-Akinosi block, and the Gow-Gates block can all be utilized to provide profound anesthesia in the mandible.
PURCHASE COURSE
This course was published in the December 2021 issue and expires December 2024. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the December 2021 issue and expires December 2024. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the most frequent target for block anesthesia, and various approaches to achieving profound anesthesia in the mandible.
- Explain the advantages, disadvantages and challenges associated with the conventional inferior alveolar nerve block, as well as the Vazirani-Akinosi and Gow-Gates techniques.
- Describe the nerve systems anesthetized with these methods.
Mandibular block anesthesia plays an important role in the provision of profound anesthesia to the mandible. This article describes three techniques for providing successful block anesthesia in the mandible, particularly in the posterior regions, where there is a well-recognized resistance to profound anesthesia. The target of these techniques is the trigeminal, or fifth, cranial nerve; more specifically, the inferior alveolar nerve. The trigeminal nerve has three terminal branches: ophthalmic, maxillary and mandibular. Both the maxillary and mandibular branches are of specific interest because they provide sensory innervation to the teeth, periodontium and related structures.
Block anesthesia can be achieved in both the maxillary and mandibular divisions, although mandibular blocks tend to be used far more frequently. The mandibular division has a motor branch that innervates the muscles of mastication, but it is the multiple sensory branches that are targets of interest in dentistry. These branches include the auriculotemporal, mylohyoid, mental, lingual, incisive, buccal and inferior alveolar. The inferior alveolar nerve — the most frequent target for these techniques — is the largest branch of the largest division of the largest cranial nerve — and yet its exact location is often elusive when it comes to getting within 1 mm to provide adequate anesthesia. The reasons are varied. Among other barriers, anatomical variation, the depth of soft tissue overlying the nerve, and operator inconsistency contribute to a sometimes challenging injection. As noted, this article describes three techniques and will assist the practitioner in developing a consistently reliable technique, either through modification of his or her current approach, or by adopting one of the alternative methods presented here.
ALTERNATIVE TECHNIQUES
A number of alternatives to the mandibular block have been developed to provide profound anesthesia without the technical challenges of completing successful mandibular blocks. These techniques also minimize some of the less desirable aspects of mandibular blocks; for example, lingual and labial anesthesia when not otherwise needed for comfortable therapy. These approaches include intraligamentary and intraosseous injections. Although these can be accomplished using conventional syringes, devices have been developed specifically for intraligamentary and intraosseous injections to achieve more predictable results. Mandibular infiltration can also be utilized, especially in the anterior region. Its effectiveness in the posterior can be limited, but the use of articaine has been proposed to increase effectiveness.
There are pros and cons to every approach. This article will focus on the conventional block, the Vazirani-Akinosi block, and the Gow-Gates block; it will also discuss the advantages and disadvantages of each technique.
CONVENTIONAL TECHNIQUE
The conventional inferior alveolar nerve block (IANB) is also referred to as the Halsted approach. In the late 1800s, Halsted utilized early adaptations of the hypodermic syringe and cocaine to block the inferior alveolar nerve. The first successful use was reported in the literature in 1885.1 This technique is commonly referred to as a mandibular block, although it is not a true mandibular block, as many branches of the nerve are not included in this approach. This technique anesthetizes the inferior alveolar, incisive, mental and lingual nerves. Success depends on a number of factors, but many reports suggest success rates between 80% and 85%,2 with effective onset in three to five minutes.3 Although reports vary in the literature, it is generally accepted that success rates are lower for the conventional technique compared to the Vazirani-Akinosi and Gow-Gates.3

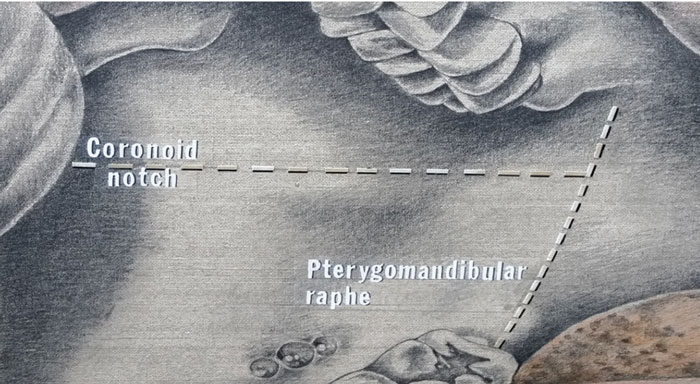
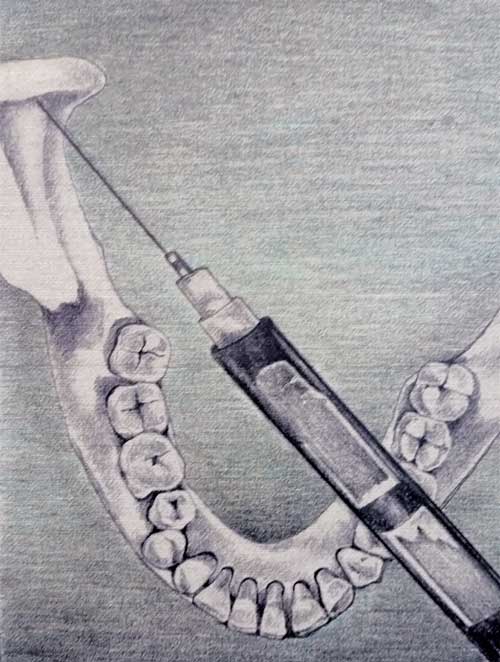
It is important to first locate the proper landmarks — in this case, the coronoid notch (the greatest depth of the anterior border of the ramus), pterygomandibular raphe, and the occlusal plane of the mandibular teeth (Figure 1). The target area is located by bisecting the thumb or index finger in the coronoid notch, keeping the needle parallel to, and 6 to 10 mm above, the mandibular occlusal plane.3,4 The needle is inserted at two-thirds to three-quarters of the distance from the anterior border of the ramus (thumb or index finger location) to the pterygomandibular raphe. It is inserted to a depth of 20 to 25 mm, or two-thirds the length of a long needle (Figure 2). The barrel of the syringe is located over the contralateral mandibular bicuspids.
This technique is not without its challenges. Many of the difficulties arise from variability in the landmarks. This can be due to normal anatomical variation, as well as the challenge of estimating the distances and locations as described above. Additional factors that can lead to challenges in effective anesthesia include an anatomical variant, such as the bifid mandibular nerve (which is estimated to be present in 1% of individuals). This technique does not include the buccal nerve, so an additional injection targeting this nerve will be necessary if the clinician wishes to anesthetize the buccal tissues of teeth in that quadrant. Accessory innervation, such as from the mylohyoid or cutaneous colli nerves, may also present challenges to effective anesthesia.
Among the reasons for failure of conventional IANBs are the anatomical challenges noted above, inadequate doses of anesthetic agent, and the presence of inflammation — including the “hot tooth” that is one of the more difficult challenges in dentistry, especially when it involves first or second mandibular molars. An extremely anxious patient also presents challenges, although this may be due to anxiety that requires a psychological approach.5 Nonetheless, this patient still presents challenges to obtain effective anesthesia, and confidence in the block technique will help the practitioner allay any fears the patient may bring to the appointment.5,6

VAZIRANI-AKINOSI
The Vazirani-Akinosi technique is also known as the closed mouth mandibular block or tuberosity block. This injection is typically administered to a patient presenting with trismus and an inability to open. Other mandibular block techniques require a patient who can open widely. If a patient with trismus requires anesthesia on mandibular posterior teeth, this is the only option available other than an extraoral block. Very few dentists have training in the extraoral block. This technique anesthetizes the inferior alveolar, incisive, mental, lingual and mylohyoid nerves, as well as the motor nerves innervating the muscles of mastication. Anesthetizing the motor branches allows progressive relaxation of the muscles, affording an opportunity to complete work on posterior mandibular teeth.
The technique was described by Akinosi7 in 1977, and in an earlier article by Vazirani8 in 1960, as an alternative to a conventional block, with the added advantage of being able to use it on a patient with severe trismus. Some of the reported advantages ascribed to this technique include a lower positive aspiration rate than the conventional block, and its reported effectiveness in the presence of a bifid nerve or canal. This is likely due to the technique’s higher target site on the nerve trunk, compared with target sites using conventional mandibular blocks. This technique is also relatively atraumatic.
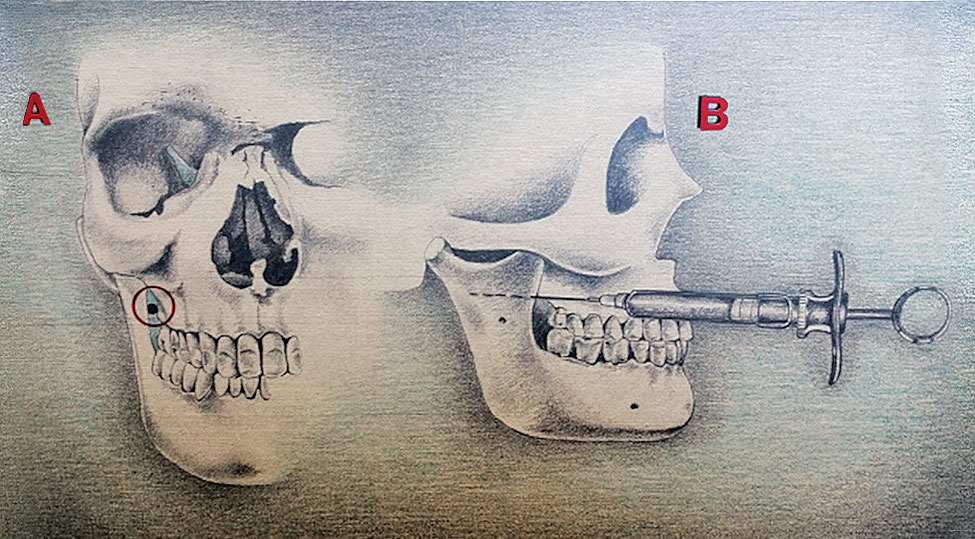
The teeth should be closed lightly for this technique and the cheek retracted. The target is the medial border of the ramus adjacent to the tuberosity, hence the alternate name of the tuberosity technique (Figure 3). This should not be confused with a tuberosity approach, Division 2 block of the maxilla.
The needle should be at the height of the mucogingival junction of the maxillary second or third molars and parallel to the maxillary occlusal plane, and advanced posteriorly and laterally to a depth of approximately 25 mm. There should be no bony contact (Figure 4). Anesthesia should be effective in five minutes.
This technique presents its own challenges; for example, it can be difficult to visualize the path of the needle, as well as its depth. Because no bony contact is expected, it is important to judge the depth. The suggested 25 mm depth is, of course, an average, and depends on the size of the patient and thickness of tissue. It is important to maintain some distance from the maxilla to avoid scraping the periosteum with the needle as it advances posteriorly (Figure 5). Besides its effectiveness in patients with trismus, another significant advantage is its usefulness when treating individuals with special needs, including children who refuse to cooperate when asked to open wide. The only modification for a pediatric patient would be to shorten the penetration depth.
GOW-GATES
The Gow-Gates block is also known as a third division block or V3 nerve block, as it is a true block of the entire mandibular nerve. Developed by Gow-Gates, a paper on the technique was initially published in 1973.9 This approach anesthetizes the inferior alveolar, incisive, mental, lingual, mylohyoid, buccal and auriculotemporal nerves.

This technique requires that the patient be supine with the mouth wide open. Having the patient open widely allows the condyle to move anteriorly and in an inferior direction, bringing it closer to the nerve trunk. The ultimate target is the neck of the condyle below the insertion of the lateral pterygoid (Figure 6). This is in contrast with the conventional technique in which the target is just above the lingula, or mandibular foramen. Of the three techniques presented in this article, this is the highest approach in relation to the nerve trunk.
The benefit of the higher approach is that the nerve trunk is larger, which offers a greater chance of success. Another advantage of the higher approach is the anesthetic is deposited in an area of the nerve trunk before any branches separate, thus effectively anesthetizing the entire nerve. This precludes needing to give a separate buccal nerve injection and also anesthetizes the auriculotemporal nerve if that is a goal.
The needle is inserted just below the mesiopalatal cusp of the maxillary second molar, approximately 10 to 25 mm above the mandibular occlusal plane. It enters the tissue just distal to the maxillary second molar to a depth of 25 mm. If possible, the patient should remain open for 20 to 30 seconds to allow the condyle to keep the nerve in its present position, bathing it in the anesthetic solution. Figure 7 shows the point of penetration of the needle in relation to the maxillary second molar.2
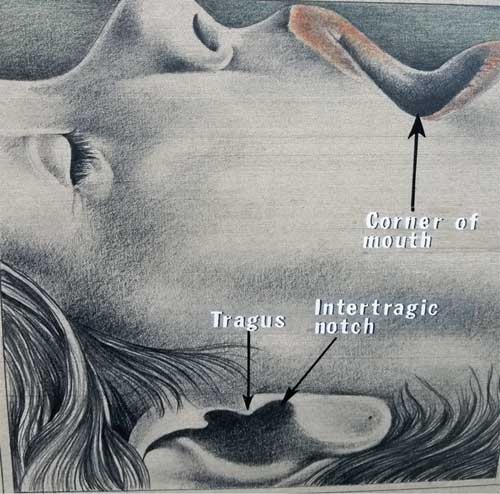
Gow-Gates based his alternative technique on anatomical findings; that is, this approach uses extraoral landmarks to confirm proper needle positioning. His research showed the syringe should be parallel with a line from the corner of the mouth to the intertragic notch of the ear. In addition, he found the angle of the syringe should parallel the angle that the ear makes with the side of the face. This matches the flare of the ramus of the mandible and can help clinicians determine how medial or lateral the approach should be. This knowledge fosters an appreciation for the markedly higher approach this technique takes compared to the Halsted technique. Figure 8 shows the extraoral landmarks used in this technique, and Figure 9 shows the syringe in relation to these extraoral landmarks.
There are several disadvantages to this technique. It takes practice and is best learned through individual instruction and hands-on practice. The onset of anesthesia, which ranges between five to seven minutes, may take longer than other approaches. Sometimes the volume of anesthetic needed is greater, necessitating a second injection, but this is variable.
There are a number of advantages to this technique, as well. There is less chance of an intravascular penetration due to the reduced vasculature in the area. Positive aspiration rates for the Gow-Gates technique average 2% compared to 10% to 15% for a conventional block.2 Aspiration before a block or infiltration injection is always indicated, however, no matter which technique is employed. There is also less discomfort and post-injection trismus associated with this technique, as there is minimal muscle penetration of the needle.9 Other than buccinator fibers on initial penetration, the needle should pass through the pterygomandibular space between the temporalis and medial pterygoid. The primary reason to utilize this technique, in the author’s opinion, is its high success rate.
DISCUSSION
Each practitioner may have his or her own idea of what success looks like when it comes to anesthesia. Here are three suggested hallmarks of success: effectiveness, speed of onset, and pain on injection. First and foremost, the patient must be numb, and most providers would agree that a consistently high success rate will help achieve this. Speed of onset is also desirable, and although the difference between four and eight minutes may not seem like much, it can be in a busy practice. The last hallmark, pain on injection, seems to garner the most attention from patients, even if it may not be a primary factor for the dentist. Practitioners are frequently judged by how well this part of the appointment goes. An effective block technique that addresses these criteria will lead to a more satisfying and efficient practice and instill confidence in the patient.

Success rates vary significantly in the literature, and range from 80% to 95% for the conventional block.2,4–6 Malamed’s3 text notes failure rates for accomplishing effective anesthesia using the conventional block, with rates reported from 31% to 46% depending on anatomical location, from the second molar to canine. Gow-Gates, in his original article,9 reported using it over 50,000 times with a negligible failure rate, and in a subsequent article10 he reported a success rate of 98.3%. While Akinosi’s7 paper does not purport to have a higher success rate, it does claim a faster onset of action, and further suggests it is easy to administer and markedly less painful than other approaches. Malamed11 reported a success rate of 97.5% in his review of the Gow-Gates technique.
MANDIBULAR INFILTRATION
Articaine was introduced to U.S. dentists in 2000 and has enjoyed a steady increase in popularity. Its ability to diffuse through soft and hard tissues has made it especially valuable in maxillary infiltrations. The thickness of the cortical bone on the mandible provides a particular challenge for use in mandibular infiltrations. While studies have reported mixed results,12,13 4% articaine has been shown to be more effective than 2% lidocaine in posterior mandibular infiltrations — although the ability to obtain effective pulpal anesthesia using infiltration alone is limited. Meechan12 did show the effectiveness of a conventional block using 2% lidocaine could be improved by supplementing it with buccal infiltration of 4% articaine.
BUFFERING AGENTS
While physicians have used sodium bicarbonate as a buffering agent for years, this technique has only recently been embraced in dental settings.3 The challenge of introducing buffering agents into dental cartridges has largely been solved by a variety of companies and their respective devices. The advantages of buffering local anesthetics are multiple, with the primary benefit being speed of onset. It has been suggested that onset of buffered anesthesia ranges from one to three minutes, cutting waiting time at least in half. Another advantage is the neutralization of the normally acidic anesthetic solution to approximately 7.4 pH, which should result in less discomfort for the patient; by comparison, unbuffered anesthetic has a pH of around 3 to 4. These two qualities make it a valuable adjunct to the anesthetic armamentarium. Speed of onset and a painless injection address two of the success parameters discussed above. These, coupled with an effective block technique, should make for a confident practitioner and satisfied patient.
An additional benefit of buffering may be an increased effectiveness on pulpally involved teeth. A recent systematic review reported that buffered anesthetics have a greater likelihood of achieving effective anesthesia in these challenging cases.14 Pulpally involved mandibular molars provide one of the most difficult challenges for a dentist. The advantages of buffered anesthetics are clear in these difficult cases, with effectiveness, speed of onset, and pain on injection all favorably impacted by the addition of the buffering agent.

SUMMARY
There are a number of techniques available to anesthetize the mandible, and each has its advantages and disadvantages. If a clinician is satisfied with his or her success rate, change is not advised. However, it is important to be aware of other options in case clinical circumstances dictate the use of alternative methods.
Although the literature reports varying success rates for different techniques, all of these approaches have the potential to provide profound anesthesia. As Hass2 notes, experience does matter, and an experienced practitioner may have success rates far higher than reported in the literature.
REFERENCES
- Jorgensen NB, Hayden J. Sedation, Local and General Anesthesia in Dentistry. 2nd ed. Philadelphia: Lea and Febiger; 1973:146.
- Haas DA. Alternative mandibular nerve block techniques, a review of the Gow-Gates and Akinosi-Vazirani closed-mouth mandibular nerve block techniques. J Am Dent Assoc. 2011;142(Suppl 3):8S–12S.
- Malamed SF. Handbook of Local Anesthesia. 6th ed. St. Louis: Elsevier Mosby; 2013:225,226–233,356–359.
- Malamed S. Is the mandibular nerve block passe? J Am Dent Assoc. 2011;142(Suppl 3):3S–7S.
- Wong MK, Jacobsen PL. Reasons for local anesthesia failures. J Am Dent Assoc. 1992;123:69–73.
- Kaufman E, Weinstein P, Milgrom P. Difficulties in achieving local anesthesia. J Am Dent Assoc. 1984;108:205–208.
- Akinosi JO. A new approach to the mandibular nerve block. Br J Oral Surg. 1977;15:83–87.
- Vazirani JS. Closed mouth mandibular nerve block: a new technique. Dent Digest. 1960;66:10–13.
- Gow-Gates GA. Mandibular conduction anesthesia: a new technique using extraoral landmarks. Oral Surg Oral Med Oral Pathol. 1973;36:321–328.
- Gow-Gates GA, Watson JE. The Gow-Gates mandibular block: further understanding. Anesth Prog. 1977;24:183–189.
- Malamed SF. The Gow-Gates mandibular block. Evaluation after 4,275 cases. Oral Surg Oral Med Oral Pathol. 1981;51:463–467.
- Meechan JG. The use of the mandibular infiltration anesthetic in adults. J Am Dent Assoc. 2011;142(Suppl 3):19S–24S.
- Robertson D, Nusstein J, Reader A, Beck M, McCartney M. The anesthetic efficacy of articaine in buccal infiltration of mandibular posterior teeth. J Am Dent Assoc. 2007;138:1104–1112.
- Kattan S, Lee Su-Min, Hersh EV, Karabucak B. Do buffered local anesthetics provide more successful anesthesia than nonbuffered solutions in patients with pulpally involved teeth requiring dental therapy? A systematic review. J Am Dent Assoc. 2019;150:165–177.
From Decisions in Dentistry. December 2021;7(11):40-44.

