
 MKARCO/ISTOCK/GETTY IMAGES PLUS
MKARCO/ISTOCK/GETTY IMAGES PLUS
The Problem With Bruxism
Clenching while awake or asleep is a predictor of temporomandibular disorder, and a causative factor in its persistence.
Part 1 of a two-part series: The first article in this two-part series explores how terminology related to grinding and clenching can lead to misunderstandings in clinical practice. Appearing in a future issue, Part 2 will focus on the consequences of persistent temporomandibular disorders on the central nervous system.
The first installment of this two-part series will attempt to clarify the misunderstandings that arise when the word bruxism is used, because different authors define bruxism in different ways. The common oral parafunctions of grinding and clenching are sufficient to describe the consequences that result from their actions. Tooth clenching activity is most important in studies of non-temporomandibular disorder (TMD) subjects, as well as acute and chronic TMD patients. Scheduled for a future issue, the concluding installment of this series will discuss the consequences of persistent TMD on the central nervous system, and explore the concept that tooth clenching during sleep may have both beneficial and harmful consequences.
 The terms tooth clenching, tooth grinding and bruxism — all of which describe the most common forms of oral parafunctional behavior — have been a long-standing subject of discussion among dental professionals. In 2000, Christenson1 separated tooth clenching from bruxism by asserting bruxism meant tooth grinding, but not tooth clenching. Other authors have also addressed the confusion about whether bruxism means tooth clenching and tooth grinding.2–5 On the other hand, an often-used definition of bruxism combines tooth grinding and tooth clenching.6–9 Thus, at present, there is no consensus on the meaning of bruxism.
The terms tooth clenching, tooth grinding and bruxism — all of which describe the most common forms of oral parafunctional behavior — have been a long-standing subject of discussion among dental professionals. In 2000, Christenson1 separated tooth clenching from bruxism by asserting bruxism meant tooth grinding, but not tooth clenching. Other authors have also addressed the confusion about whether bruxism means tooth clenching and tooth grinding.2–5 On the other hand, an often-used definition of bruxism combines tooth grinding and tooth clenching.6–9 Thus, at present, there is no consensus on the meaning of bruxism.
The term sleep bruxism has been defined as a repetitive activity of the jaw muscles, identified mainly as tooth grinding or clenching during sleep.10,11 Thereupon, the definition of sleep bruxism as a sleep movement disorder conflates both grinding and clenching. Moreover, sleep bruxism has been described as grinding of the teeth, and wake bruxism being characterized mainly by tooth clenching,12–15 yet the interrelationships between sleep bruxism and awake bruxism remain uncertain.10,16 Even though sleep bruxism and awake bruxism may coexist in the same individual,10 oral parafunctions of tooth clenching and grinding appear to have characteristic differences.14,17
Tooth clenching requires little or no jaw movement, is considered to be a static tooth-together jaw position in maximum intercuspation or centric occlusion, and creates no significant parafunctional attrition to the dentition. In addition, when comparing tooth clenching to grinding, marked dissimilarities exist with respect to their respective pathophysiology.10,18,19 Christenson1 crystallized the issue of the disparate meanings of bruxism, noting, “This subject is highly controversial. I fully expect to stimulate discussion on differences of opinion.” Therefore, for the purpose of clarity, this paper will avoid using the term bruxism, and instead use the terms tooth clenching and tooth grinding. This clarifying teaching method is a clinical complement in the dental office and facial pain clinic, and has academic utility in the postgraduate classroom.20
Based on a systematic literature review, the authors of this paper present evidence-based research and expert opinion regarding tooth clenching that may help the practicing dentist advance the caliber of care for patients experiencing TMD.
Tooth grinding is another matter. Evidence supporting a causal relationship between tooth grinding and TMD pain is unconvincing.6,21 The presence of tooth wear facets caused by tooth grinding (parafunctional attrition) has little value as it relates to any predictive power to forecast the first onset or development of TMD.22–24 In addition, tooth wear cannot be understood to be an indicator of sleep bruxism or masseter muscle activity during sleep.25 Tooth grinding events during sleep have been shown to immediately follow a linear series of autonomic, cardiac and electroencephalography events associated with micro-arousals.26 Overall, patients who complain of TMD pain appear to grind less when compared to those who grind their teeth more often.27 Parafunctional tooth grinding has been shown to be closely associated with pediatric and adult tooth wear.28

CONTRIBUTORS TO PARAFUNCTIONAL HABITS
A panel of international dental and pain experts undertook an orofacial pain prospective evaluation and risk assessment project (OPPERA) designed to characterize the etiology and the persistence of TMD pain.29 The efforts of their scientific, evidence-based enterprise resulted in the development of a dual axis assessment for research purposes termed the research diagnostic criteria for temporomandibular disorders (RDC/TMD). A recent OPPERA update of the dual axis RDC/TMD assessment, entitled the diagnostic criteria for TMD, was designed to be used by both clinicians and researchers.30 Axis I spelled out the standard diagnostic criteria based on the most common TMD clinical signs and symptoms. Axis II spelled out associated disabilities of the psychosocial and behavioral components of TMD pain, which included oral parafunctional behaviors, such as clenching. In prospective cohort studies, no single risk factor was identified as the cause of TMD. However, oral parafunctional behaviors, such as tooth clenching or maintaining a rigid jaw, were shown to be significant predictors of TMD onset and associated with the development of persistent TMD pain.24,31
Supported by RDC/TMD guidelines, a self-reporting, 21 item, validated screener entitled the oral behaviors checklist was developed to estimate the status of oral parafunctional behavior in TMD patients.32 Using a laboratory version of the checklist, and studying both TMD and non-TMD subjects, researchers demonstrated significantly higher electromyography (EMG) activity of the masseter and temporalis muscles (though not the suprahyoid muscles) during awake tooth clenching.33 Nine other non-clenching behaviors were similarly evaluated, which were shown to have significantly lower EMG activity of the temporalis and masseter muscles, including holding the jaw rigid and tenseness (Figure 1). In this study, surface EMG technique was used as an appropriate methodology for detecting muscle activity — for perspective, EMG has been widely used in both clinical and research dentistry for patients with myofascial pain in the face and jaws.34–36

AWAKE TOOTH CLENCHING IN NON-TMD SUBJECTS
Svensson and Arendt-Nielsen37 conducted a 5-day experimental tooth clenching study on a small population of awake healthy females (n = 10) who apparently had no history of tooth clenching. A once-daily trial for five consecutive days of clenching on a bite force transducer for 15 minutes at 25% of maximum voluntary contraction (MVC) failed to produce any continuing increase in pain or tenderness of the muscles of mastication. On the other hand, awake non-TMD subjects who had a history of tooth clenching were shown to be susceptible to limited periods of subsequent jaw pain.38 In addition, tooth clenching tasks showed low level increases in jaw pain and fatigue during and after two separate clenching sessions compared to a non-clenching control group.39 Moreover, this study found that even in the absence of tooth clenching, when the dental arches are fully engaged in centric occlusion, the elevator muscles of the mandible were more active compared to the physiological rest position of the mandible.39
 The physiological rest position of the mandible at a free-way space or postural vertical dimension is a 2 to 4 mm separation between the occlusal surfaces of the maxillary and mandibular teeth.40 Several studies have shown that non-TMD subjects tested with the mandible at physiological rest position demonstrated an average EMG value of 3.13 millivolt (mv) for the masseter and temporalis muscles.41,42 Subsequently, Glaros and Burton43 employed a submaximal tooth clenching model using an EMG biofeedback design studying the activity of the bilateral temporalis and masseter muscles for a small population (n = 14) of non-TMD subjects. The clenching trials lasted 20 minutes for five successive days. The results showed EMG activity of 10 mv or above produced significantly higher levels of pain in all subjects compared to a 2 mv or less level of EMG activity. The authors concluded that low-level bite forces produced by tooth clenching at or above 10 mv may play a role in the development of myofascial-related TMD pain. Other EMG experiments designed to achieve a submaximal bite force by voluntary awake sustained tooth clenching trials have produced symptoms resembling myofascial TMD pain.44,45
The physiological rest position of the mandible at a free-way space or postural vertical dimension is a 2 to 4 mm separation between the occlusal surfaces of the maxillary and mandibular teeth.40 Several studies have shown that non-TMD subjects tested with the mandible at physiological rest position demonstrated an average EMG value of 3.13 millivolt (mv) for the masseter and temporalis muscles.41,42 Subsequently, Glaros and Burton43 employed a submaximal tooth clenching model using an EMG biofeedback design studying the activity of the bilateral temporalis and masseter muscles for a small population (n = 14) of non-TMD subjects. The clenching trials lasted 20 minutes for five successive days. The results showed EMG activity of 10 mv or above produced significantly higher levels of pain in all subjects compared to a 2 mv or less level of EMG activity. The authors concluded that low-level bite forces produced by tooth clenching at or above 10 mv may play a role in the development of myofascial-related TMD pain. Other EMG experiments designed to achieve a submaximal bite force by voluntary awake sustained tooth clenching trials have produced symptoms resembling myofascial TMD pain.44,45
AWAKE TOOTH CLENCHING IN TMD SUBJECTS
Recent studies have associated wake-time tooth clenching with TMD.46,47 Self-recognition of awake tooth clenching or holding the jaw rigid were reported to be the two strongest predictors of TMD.24 In a study on the frequency of nonfunctional tooth contact, patients with TMD exhibited four times more wake-time nonfunctional static tooth contact compared to healthy control subjects.48 Huang et al49 investigated risk factors associated with subgroups of awake TMD patients compared to non-TMD controls. Their results showed a significantly high proportion of patients with TMD reported they held their teeth together or clenched during waking hours.
A low EMG level of 1 to 2 mv, which is equivalent to the physiological mandibular rest position, is unlikely to significantly activate jaw elevator muscle nociceptors, whereas the magnitude of muscle activity in patients with TMD is less important than the persistence of muscle activity when the teeth are held together.50 That is, low-level EMG activity of jaw elevator muscles with the teeth together or during clenching may persist for long periods.43
AWAKE TOOTH CLENCHING IN CHRONIC TMD SUBJECTS
Wang et al51 utilized a chronic jaw pain model to investigate if submaximal tooth clenching could be associated with motor-evoked jaw pain for patients with chronic TMD during variable and precisely controlled submaximal tooth clenching forces. The experimental paradigm involved visually guided tooth grip static force tasks. The chronic TMD group was chosen, in part, by utilizing a screening instrument derived from an enlarged RDC-TMD assessment protocol.52 All subjects in the chronic TMD patient groups had experienced jaw pain for at least six months. In addition, when compared to controls, all subjects in the chronic TMD patient groups reported a higher frequency of parafunctional activity (i.e., tooth clenching). Bite force during tooth clenching was measured by a force transducer incorporated into a bite device with two bite plates. All subjects were placed in a supine position, with the bite plates held between the maxillary and mandibular dental arches.
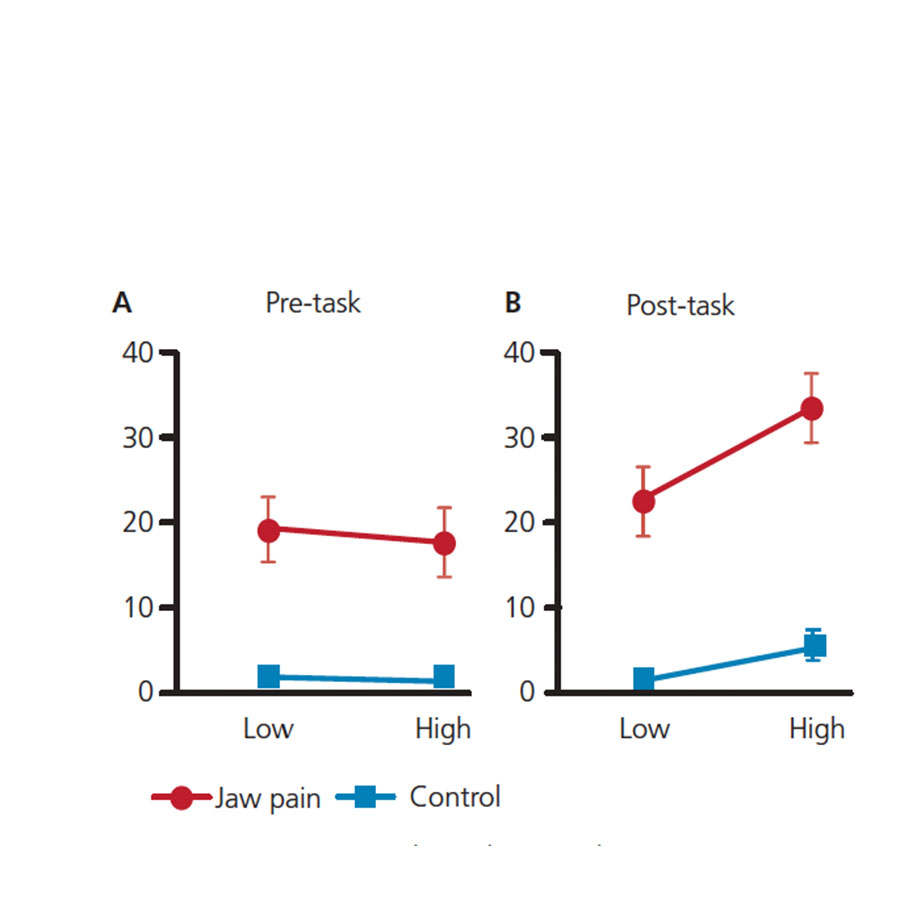
An alternating series of three clenching efforts on the bite plates were performed. All subjects were instructed to clench on the bite plates for five seconds in order to produce a MVC value. Data was collected during a series of clenching efforts on the bite plates at a low clenching effort of 2% of MVC for 30 seconds, and a higher clenching effort of 15% of MVC for 30 seconds. Measurements of pre-task and post-task jaw pain were collected for all clenching efforts by means of a visual analog scale. Figure 2A shows the pre-task jaw pain intensity measurements before and after the alternating isometric grip-force clenching efforts. The pre-task clenching efforts at the low 2% of MVC for both the chronic TMD patient groups and controls were essentially unchanged compared to the pre-task efforts at the higher 15% of MVC.
Importantly, Figure 2B shows a statistically significant increase in jaw pain in post-task efforts for the chronic jaw pain patients compared to control subjects. At the 15% post-task level, jaw pain increase in the chronic pain patient group was three times greater compared to controls. The results of this study support the position that production of isometric voluntary jaw force contraction, akin to tooth clenching, elicits increases in motor-evoked jaw pain. In addition, Wang et al51 reported their chronic jaw pain subjects experienced significantly greater jaw pain compared to controls when the tooth clenching task required subjects to produce a bite force equal to 15% of MVC for 30 seconds per trial.
Chronic pain syndromes can activate nociceptive neurons with distinct supraspinal projections, thus altering brain activity at diverse loci.53 Roy et al54 utilized functional magnetic resonance imaging to identify neuronal metabolic activity in regions of the brains of patients with chronic jaw pain. The results may portray neural networks reactive to the output of trigeminal nociception during changes in static forces generated by the elevator muscles of the mandible during submaximal bite force tooth clenching trials. The resultant functional activity areas included the prefrontal cortex and rostral ventral premotor cortex.
LOOKING AHEAD
The concluding installment of this series, appearing in an upcoming issue, will highlight the consequences of persistent TMD on the central nervous system. In addition, it will explore the concept that tooth clenching during sleep appears to have both beneficial and harmful consequences. Moreover, studies of low-level EMG background muscle activity offer evidence of the nature of tooth clenching during sleep, as well as the intraoral tissue formations of linea alba and scalloped tongue.
KEY TAKEAWAYS
- The terms tooth clenching, tooth grinding and bruxism — all of which describe the most common forms of oral parafunctional behavior — have been a long-standing topic of controversy among dental professionals.
- This paper attempts to clarify the misunderstandings that arise when the word bruxism is used, because different authors define bruxism in different ways.
- Some have asserted that bruxism means tooth grinding, but not tooth clenching, while others suggest bruxism combines tooth grinding and clenching.6–9 Thus, at present, there is no consensus on the meaning of bruxism.
- Furthermore, this activity may involve awake bruxism and/or sleep bruxism, yet the interrelationships between the two remain uncertain.10,16
- Even though sleep bruxism and awake bruxism may coexist in the same individual,10 oral parafunctions of tooth clenching and grinding appear to have characteristic differences.14,17
- Based on a systematic literature review, the authors present evidence-based research and expert opinion regarding tooth clenching that may help the practicing dentist advance the caliber of care for patients experiencing temporomandibular disorders.
REFERENCES
- Christenson GJ. Treating bruxism and clenching. J Am Dent Assoc. 2000;131:233–235.
- Bell WE. Orofacial Pain: Classification Diagnosis Management. 3rd ed. Chicago Ill: Year Book Medical Publishers Inc; 1985:131.
- Mahan PE, Alling CC. Facial Pain. 3rd ed. Philadelphia, Pa: Lea & Febiger; 1991:187.
- Dao TT, Lund JP, Lavigne GJ. Comparison of pain and quality of life in bruxers and patients with myofascial pain in the masticatory muscles. J Orofacial Pain. 1994;8:350–356.
- Miyake R, Ohkubo R, Takehara J, Morita M. Oral parafunctions and association with symptoms of temporomandibular disorders in Japanese university students. J Oral Rehabil. 2004;31:518–523.
- Janal MN, Raphael KG, Klausner J, Teaford M. The role of tooth grinding in the maintenance of myofascial pain: a test of alternate models. Pain Med. 2007;8:486–496.
- Koyano K, Tsukiyama Y, Ichiki R, Kuwata T. Assessment of bruxism in the clinic. J Oral Rehabil. 2008;35:495–508.
- Paesani DA. Bruxism: Theory and Practice. Chicago, Ill: Quintessence; 2010:3–19.
- Lobbezoo F, Ahlberg AG, Glaros AG, et al. Bruxism defined and graded: an international consensus. J Oral Rahabil. 2013;40:2–4.
- American Academy of Sleep Medicine. International classification of sleep disorders. AASM Sleep Related Bruxism. 3rd ed. Chicago, Ill: Westchester; 2014:303–311.
- Rugh JD, Harlan J. Nocturnal bruxism and temporomandibular disorders. Adv Neurol. 1988;49:329–341.
- Essick GK, Raphael KG, Sanders AE, Lavigne G. Orofacial pain and temporomandibular disorders in relation to sleep disorder breathing and sleep bruxism. In: Principles and Practice of Sleep Medicine. Kryger M, Roth T, Dement WC, eds. 6th ed. Philadelphia, Pa: Elsevier; 2017:1435–1444.
- Dutra K, Pereira FJ Jr, Rompre PH, Fleming N, Lavigne GJ. Oro-facial activities in sleep bruxism patients and in normal subjects: a controlled polygraphic and audio-video study. J Oral Rehabil. 2009;36:86–92.
- Carlsson GE, Egermark I, Magnusson T. Predictors of bruxism, other oral parafunctions, and tooth wear over a 20-year follow-up period. J Orofac Pain. 2003;17:50–57.
- Lavigne GJ, Khoury S, Abe S, Yamaguchi T, Raphael K. Bruxism physiology and pathology: an overview for clinicians. J Oral Rehabil. 2008;35:476–494.
- Winocur E, Buenaver L, Patil SP, Smith MT. Pharmacotherapy, complementary, and alternative medicine for sleep bruxism. In: Principles and Practice of Sleep Medicine. Kryger M, Roth T, Dement WC, eds. 6th ed. Philadelphia, Pa: Elsevier; 2017:1478–1483.
- Lobbezoo F, Koyano K, Paesani DA, Manfredini D. Sleep bruxism: diagnostic considerations. In: Principles and Practice of Sleep Medicine. Kryger M, Roth T, Dement WC, eds. 6th ed. Philadelphia, Pa: Elsevier; 2017:1427–1434.
- Huynh N, Lavigne GJ, Okura K, Yao D, Adachi K. Sleep bruxism. In: Handbook of Clinical Neurology Vol. 99 (3rd series) Sleep Disorders Part 2. Montagna P, Chokroverty S, eds. Philadelphia, Pa: Elsevier: 2011.
- Carra MC, Huynh N, Lavigne G. Sleep bruxism: a comprehensive overview for the dental clinician interested in sleep medicine. Dent Clin N Am. 2012;56:387–413.
- Fuselier B, Loughner B. Bruxism is not clenching: a heuristic rationale. Dental Society of Greater Orlando Journal. Spring;2017:22–24.
- Lobbezoo F, Lavigne G. Do bruxism and temporomandibular disorders have a cause and effect relationship? J Orofac Pain. 1997;11:15–23.
- Hirsch C, John MT, Lobbezoo F, Setz JM, Schaller HG. Incisal tooth wear and self-reported TMD pain in children and adolescents. Int J Prosthodont. 2004;17:205–210.
- Schierz O, John MT, Schroeder E, Lobbezoo F. Association between anterior tooth wear and temporomandibular disorder pain in a German population. J Prosthet Dent. 2007;97:305–309.
- Ohrbach R, Bair E, Fillingim RB, et al. Clinical orofacial characteristics associated with risk of first-onset TMD: The OPPERA prospective cohort study. J Pain. 2013;14(Suppl 12):T33–T50.
- Manfredini D, Lombardo L, Visentin A, Arreghini A, Siciliani G. Correlation between sleep-time masseter muscle activity and tooth wear: an electromyographic study. J Oral Facial Pain Headache. 2019;33:199–204.
- Lavigne GJ, Huynh N, Kato T, et al. Genesis of sleep bruxism: motor and autonomic-cardiac interactions. Arch of Oral Biology. 2007;52:381–384.
- Rompre PH, Daigle-Landry D, Guitard F, Montplaisir JY, Lavigne GJ. Identification of a sleep bruxism subgroup with a higher risk of pain. J Dent Res. 2007;86:837–842.
- Knight DJ, Leroux BG, Zhu C, Almond J, Ramsay DS. A longitudinal study of tooth wear in orthodontically treated patients. Am J Ortho Dentofacial Orthop. 1997;112:194–202.
- Dworkin SF, LeResche L. Research diagnostic criteria for temporomandibular disorders: review, criteria, examinations and specifications, critique. J Craniomandib Disord. 1992;6:301–355.
- Schiffman E, Ohrbach R, Truelove E, et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the international RDC/TMD consortium network and orofacial pain special interest group. J Oral Facial Pain Headache. 2014;28:6–27.
- Ohrbach R, Fillingim RB, Mulkey F, et al. Clinical findings and pain symptoms as potential risk factors for chronic TMD: descriptive data and empirically identified domains from the OPPERA case-control study. J Pain. 2011;12(Suppl 11):T25–T45.
- Ohrbach R, Beneduce C, Markiewicz MR, McCall WD Jr. Psychometric properties of the oral behaviors checklist: preliminary findings. J Dent Res. 2004;83(special issue A):1194.
- Ohrbach R, Markiewicz MR, McCall WD Jr. Waking-state oral parafunctional behaviors: specificity and validity as assessed by electromyography. Eur J Oral Sci. 2008;116:438–444.
- Nishi SE, Basri R, Alam MK. Uses of electromyography in dentistry: an overview with meta-analysis. Eur J Dent. 2016;10:419–425.
- Castroflorio T, Bracco P, Farina D. Surface electromyography in the assessment of jaw elevator muscles. J Oral Rehabil. 2008;35:638–645.
- Szyszka-Sommerfeld L, Machoy M, Lipski M, Woźniak K. The diagnostic value of electromyography in identifying patients with pain-related temporomandibular disorders. Front Neurol. 2019;10:180.
- Svensson P, Arendt-Nielsen L. Effects of 5 days of repeated submaximal clenching on masticatory muscle pain and tenderness: an experimental study. J Orofacial Pain. 1996;10:330–338.
- Glaros AG, Tabacchi KN, Glass EG. Effect of parafunctional clenching on TMD pain. J Orofacial Pain. 1998;13:145–152.
- Dawson A, Ghafouri B, Gerdle B, List T, Svensson P, Emberg M. Pain and intramuscular release of algesic substances in the masseter muscle after experimental tooth-clenching exercises in healthy subjects. J Orofac Pain. 2013;27:350–360.
- Pertes RA. A practical approach to the diagnosis of chronic orofacial pain, part I: somatic pain. Compend Contin Educ Dent. 1988;9:16–20.
- Glaros AG. Awareness of physiological responding under stress and non-stress conditions in temporomandibular disorders. Biofeedback Self-Reg. 1996;21:261–272.
- Fogle LL, Glaros AG. Contributions of facial morphology, age, and gender to EMG activity under biting and resting conditions: a canonical correlation analysis. J Dent Res. 1995;74:1496–1500.
- Glaros AG, Burton E. Parafunctional clenching, pain, and effort in temporomandibular disorders. J Behav Med. 2004;27:91–100.
- Koutris M, Lobbezoo F, Sümer NC, Atiş ES, Türker KS, Naeije M. Is myofascial pain in temporomandibular disorder patients a manifestation of delayed-onset muscle soreness? Clin J Pain. 2013;29:712–716.
- Farella M, Soneda K, Vilmann A, Thomsen CE, Bakke M. Jaw muscle soreness after tooth-clenching depends on force level. J Dent Res. 2010;89:717–721.
- Slade GD, Ohrbach R, Greenspan JD, et al. Painful temporomandibular disorders: decade of discovery from OPPERA studies. J Dent Res. 2016;95:1084–1092.
- Cioffi I, Landino D, Donnarumma V, et al. Frequency of daytime tooth clenching episodes in individuals affected by masticatory muscle pain and pain-free controls during standardized ability tasks. Clin Oral Investig. 2017;21:1139–1148.
- Chen CY, Palla S, Erni S, Sieber M, Gallo LM. Nonfunctional tooth contact in healthy controls and patients with myogenous facial pain. J Orofac Pain. 2007;21:185–193.
- Huang GJ, LeResche L, Critchlow CW, Martin MD, Drangsholt MT. Risk factors for diagnostic subgroups for painful temporomandibular disorders (TMD). J Dent Res. 2002;81:284–288.
- Ohrbach R, McCall WD Jr. The stress-hyperactivity-pain theory of myogenic pain: proposal for a revised theory. Pain Forum. 1996;5:51–66.
- Wang W, Roy A, Misra G, et al. Motor-evoked pain increases force variability in chronic jaw pain. J Pain. 2018;19:636–648.
- Gonzalez YM, Schiffman E, Gordon SM, et al. Development of a brief and effective temporomandibular disorder pain screening questionnaire. J Am Dent Assoc. 2011;142:1183–1191.
- Schweinhardt P, Bushnell MC. Pain imaging in health and disease — how far have we come? J Clin Investig. 2010;120:3788–3797.
- Roy A, Wang W, Ho RL, Ribeiro-Dasilva M, Fillingim R, Coombes SA. Functional brain activity during motor control and pain processing in chronic jaw pain. Pain. 2018;159:2547–2564.
The authors have no commercial conflicts of interest to disclose.
From Decisions in Dentistry. September 2020;6(8):17-18,21-23.
